Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Hoosieroncologygroup.org
F l u o x e t i n e V e r s u s P l a c e b o i n A d v a n c e d C a n c e r O u t p a t i e n t s : A D o u b l e - B l i n d e d T r i a l o f t h e H o o s i e r O n c o l o g y G r o u p
By Michael J. Fisch, Patrick J. Loehrer, Jean Kristeller, Steven Passik, Sin-Ho Jung, Jianzhao Shen, Matthew A. Arquette,
Purpose: To determine whether fluoxetine improves modeling revealed that patients treated with fluoxetine overall quality of life (QOL) in advanced cancer patients exhibited a significant improvement in QOL as shown by the with symptoms of depression revealed by a simple survey. Functional Assessment of Cancer Therapy–General, com- Patients and Methods: One hundred sixty-three patients pared with patients given placebo (P ؍ .01). Specifically, the with an advanced solid tumor and expected survival be- level of depressive symptoms expressed was lower in pa- tween 3 and 24 months were randomly assigned in a tients treated with fluoxetine (P ؍ .0005), and the subgroup double-blinded fashion to receive either fluoxetine (20 mg of patients showing higher levels of depressive symptoms daily) or placebo for 12 weeks. Patients were screened for on the two-question screening survey were the most likely at least minimal depressive symptoms and assessed every 3 to benefit from treatment. to 6 weeks for QOL and depression. Patients with recent Conclusion: In this mix of patients with advanced cancer exposure to antidepressants were excluded. who had symptoms of depression as determined by a Results: The groups were comparable at baseline in two-question bedside survey, use of fluoxetine was well terms of age, sex, disease distribution, performance status, tolerated, overall QOL was improved, and depressive and level of depressive symptoms. One hundred twenty- symptoms were reduced. nine patients (79%) completed at least one follow-up as- J Clin Oncol 21:1937-1943. 2003 by American sessment. Analysis using generalized estimating equation Society of Clinical Oncology.
THE CARE of patients with advanced cancer is becoming outpatients.6 An 11-item version of the ZSDS, the Brief Zung
increasingly challenging because of the growing numbers
Self-Rating Depression Scale (BZSDS), has been found to have
of patients living with cancer and the increasing expectations of
acceptable levels of criterion validity.7 However, several studies
patients and their families for effective palliative care. According
have demonstrated the utility of one- or two-item questionnaires
to a recent report from the Institute of Medicine, “A major
in both primary care and palliative care settings.8,9 We have
problem in palliative care is the underrecognition, underdiagno-
piloted the use of a two-item questionnaire that assesses the
sis, and thus undertreatment of patients with significant distress
cardinal symptoms of depressed mood and anhedonia in ad-
ranging from existential anguish to anxiety and depression.”1
vanced cancer outpatients and have found it easy to administer
Significant depressive symptoms occur in roughly 25% to
35% of cancer patients.2,3 However, there are several inherent
For patients who are treated for the syndrome of major
difficulties in diagnosing depression in this population. The most
depression, 50% to 60% respond to initial therapy with antide-
obvious problem is that sadness and grief are normal responses
pressants, psychotherapy, or both.11 Compared with placebo,
to the changes associated with the diagnosis of cancer and attransitional points in the disease. In addition, the physical signsof depression may be caused by the malignancy or by medica-tions commonly used for cancer patients. Furthermore, patients
From the Department of Palliative Care and Rehabilitation, University of
and their family caregivers often do not recognize or accept the
Texas M.D. Anderson Cancer Center, Houston, TX; Division of Hematology/Oncology, Indiana University; Walther Cancer Institute, and Division ofBiostatistics, Indiana University School of Medicine, Indianapolis; Depart-
A symptom-based approach is commonly used for the man-
ment of Psychology, Indiana State University, Terre Haute, IN; Department
agement of phenomena such as pain and nausea, as well as
of Palliative Care, University of Kentucky, Lexington, KY; Department of
psychologic distress in cancer patients. This involves ascertain-
Biostatistics and Bioinformatics, Duke University, Durham, NC; and Divi-
ing whether the symptom is present, elucidating further details,
sion of Medical Oncology, Washington University, St Louis, MO.
and deciding on the proper management approach for the patient. Submitted August 2, 2002; accepted February 20, 2003. Supported in part by the Mary Margaret Walther Program for Cancer
In addition, there are no universally accepted criteria for diag-
Care Research, Indianapolis, IN. Fluoxetine, placebo, and the study note-
nosing depression in the terminally ill.4 Multiple depression
books were provided by the Eli Lilly Company, Indianapolis, IN.
questionnaires have been developed for the primary-care popu-
Presented in part at the Thirty-Seventh Annual Meeting of the American
lation, with instruments ranging in length from one to 30 items
Society of Clinical Oncology, San Francisco, CA, May 12-15, 2001.
and ranging in administration times from less than 1 to 5
Address reprint requests to Michael J. Fisch, MD, MPH, University ofTexas M.D. Anderson Cancer Center, Box 008, Room P12.2911, 1515
minutes.5 In the largest survey of depressive symptoms in
Holcombe Blvd, Houston, TX 77030-4009; email: [email protected].
ambulatory cancer patients, the 20-item Zung Self-Rating De-
2003 by American Society of Clinical Oncology.
pression Scale (ZSDS) was administered to more than 1,000
Journal of Clinical Oncology, Vol 21, No 10 (May 15), 2003: pp 1937-1943
Information downloaded from jco.ascopubs.org and provided by Indiana University School of Medicine Libraries on July 23,
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
patients with subsyndromal depression or dysthymia also benefit
epines) within 6 weeks of the baseline study evaluation; uncontrolled brain or
from treatment with an antidepressant or psychotherapy with
leptomeningeal disease; bilirubin more than 2.0 mg/dL; current use of amonoamine oxidase inhibitor; enrollment onto another clinical trial with QOL as
similar response rates.12 Fluoxetine is a familiar antidepressant
the primary end point; recent or active substance abuse; and major depression
to many oncologists, and it is the first and most widely studied
diagnosed by a psychiatrist in the past 6 months. Informed consent was obtained
selective serotonin-reuptake inhibitor. Uncontrolled trials pub-
for each patient with appropriate institutional review.
lished in the late 1980s and 1990s indicated that antidepressantsmight also be helpful in selected cancer patients.13-18 Only six
published, randomized, placebo-controlled trials have compared
Before random assignment to a treatment group, patients were stratified on the
an antidepressant drug (a tricyclic antidepressant or serotonin-
basis of Eastern Cooperative Oncology Group performance status (0 to 1 v Ն 2). Patients were then randomly assigned in a double-blind manner to receive either
reuptake inhibitor) with placebo for the treatment of depression
fluoxetine (20-mg tablets) or an identical placebo tablet. The randomization was
in patients with cancer.18-23 The trend in these data shows a
performed centrally through a preprinted randomization table, and the study drug
modest benefit of an antidepressant compared with placebo, but
was sent by overnight mail directly to the patient. The study drug was
there is concern about the generalizability of the data because of
self-administered by the patient once daily in the morning.
patient dropout and the relative preponderance of women with
Longitudinal assessments were performed at baseline and every 3 to 6
weeks thereafter and included the measurement of QOL and depression. The
breast or gynecologic malignancies in these studies.
visit interval varied among patients and often depended on the schedule for
It is clear that patients with depressive disorders benefit from
anticancer therapy. Patients were assessed for 12 weeks, and complete
treatment, but it is also evident that there are major barriers to
assessment involved three to five sessions of data collection (depending on
diagnosing depressive disorders in outpatients with advanced
the individual patient’s visit intervals). After the 12-week study period, the
cancer. The purpose of this study was to explore the efficacy and
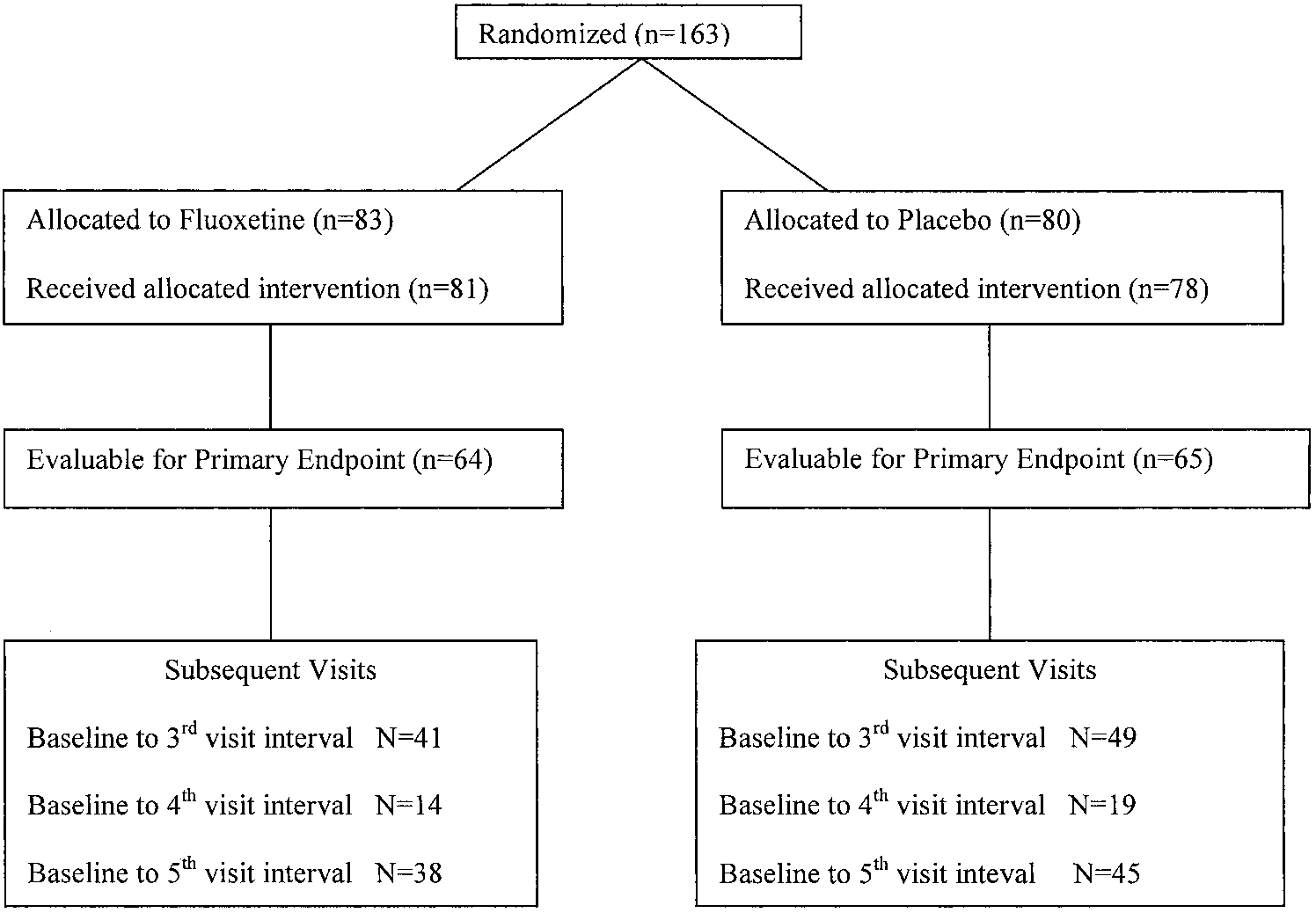
patients were given the option to continue the study drug (blinded) for up to9 more months. The flow of study participants is summarized in Fig 1.
feasibility of treating outpatients with advanced cancer with anantidepressant on the basis of the presence of at least minimal
depressive symptoms. A randomized, placebo-control design
QOL was measured using a reliable and valid 28-item self-report instru-
was needed to obtain an accurate assessment of efficacy. The
ment called the Functional Assessment of Cancer Therapy–General
primary objective was to compare the change in quality of life
(FACT-G, version 3).24 Spiritual well-being was measured using a related
(QOL) of these patients; the secondary objective was to compare
instrument, the Functional Assessment of Chronic Illness Therapy–Spiritual,
with 12 items25 (data for the latter will be reported separately). Depressivesymptoms were measured using the 11-item BZSDS.6 Higher scores repre-
sent better QOL, better spiritual well-being, and more depressive symptoms(worse health) in these assessment tools, respectively. These assessmenttools were chosen because they can easily be used in outpatient cancer-care
settings and because of their face validity.
Between July 1998 and October 2000, 163 adult ambulatory patients with
advanced, incurable malignancy were enrolled from one of 15 sites of theHoosier Oncology Group (three academic centers and 12 community sites).
The primary end point of the study was overall QOL as determined by the
Patients with an expected survival between 3 and 24 months were eligible for
FACT-G. The generalized estimating equation (GEE) method of regression
study participation. Expected survival was judged by clinicians on the basis of
was used because it is useful for analyzing data with variable measurement
the histology, stage, and comorbid status of the patient and any other prognostic
times and when there is a high probability of missing data. The GEE method
data typically used by the individual clinician (physician or nurse). Clinician-
relates predictors to the mean response variable (as in standard regression),
predicted survival was 3 to 12 months for 59% of the patients.
but it does not require that the distribution of the response variable or the
During the study period, all participating Hoosier Oncology Group
correlation structure among repeated measurements be specified.26 Fisher’s
clinicians made available to each outpatient a two-item screening survey to
exact test was used to analyze differences in the categorical variables
assess depressed mood and anhedonia. These data were used for clinical
between the study groups. Continuous variables and ordinal baseline vari-
purposes and were not limited to patients who were possible candidates for
ables were compared between treatment groups using Wilcoxon rank sum
this study. The questions were as follows: (1) “During the past month, have
tests and independent sample t tests. All hypothesis testing was carried out
you often been bothered by feeling down, depressed, or hopeless?” and (2)
using a two-sided alternative hypothesis and a 5% type I error rate.
“During the past month, have you often been bothered by having little
An additional analysis planned a priori involved a comparison of the
interest or pleasure in doing things?” To be eligible for this study, each
best-change score between the patient groups. The best-change score was
patient had to have a score of 2 or greater on this Two-Question Screening
defined as the difference between the baseline FACT-G score and the
Survey (TQSS). Each of the items (depressed mood and anhedonia) in the
average of the best consecutive scores. The use of summary measures, such
survey has five possible responses that were assigned values of 0 to 4 as
as the best change score, has been described as a relevant and statistically
follows: 0, not at all; 1, a little bit; 2, somewhat; 3, quite a bit; and 4, very
valid way to evaluate longitudinal data,27 and it has been used to analyze
much. The score on the survey was the sum of the two questions. As it
QOL data in clinical cancer research.28 We defined a best-change score of 6
pertains to this trial, the TQSS was not being used as a casefinding
points or greater as showing a response. This 6-point change was chosen as
instrument; rather, it was being used to eliminate from consideration
the response threshold because a 6-point change in the FACT-G is roughly
enrollment of patients who have no problems at all with depressed mood or
equivalent to a one-level change in the Eastern Cooperative Oncology Group
anhedonia. This was an ethical issue raised by study reviewers because these
performance status and because, in similar patient populations, it represents
asymptomatic patients were believed to have a very low possibility of
an effect size of 0.4 to 0.5, which is generally considered a small-to-moderate
benefiting from treatment with an antidepressant.
effect.24 For example, a patient with a baseline FACT-G score of 90 who had
Patients could be receiving any anticancer therapy or only the best supportive
a follow-up score of 100 and then was lost to follow-up would be considered
care. Exclusion criteria included the following: serious suicidal risk or psychotic
a nonresponder with a best-change score of 5 points. If this same patient had
behaviors; inability to swallow oral medications; regular use of antidepressants
one more follow-up with a score of 94, the best-change score of 7 points
or psychotropic drugs (other than phenothiazine-type antiemetics or benzodiaz-
would have been sufficient for the patient to be considered a responder.
Information downloaded from jco.ascopubs.org and provided by Indiana University School of Medicine Libraries on July 23,
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
FLUOXETINE VERSUS PLACEBO IN CANCER PATIENTS
Fig 1. Study flow.
Patients in each study arm were comparable at baseline with
We estimated that the SD of the FACT-G in advanced cancer patients
respect to age, sex, performance status, symptom status regarding
would be approximately 15 points. Assuming a correlation of 0.5 between
pain and depression, disease distribution, and current treatment with
the baseline and 3-month measures and adjusting for the stratification
chemotherapy. These patient characteristics are listed in Table 2. A
variable of performance status, we estimated that 80 patients per study arm
family history of depression in first-degree relatives and current or
would provide 82.7% power to detect a 6-point difference in the total score
prior psychologic counseling (individual or group) since their
between arms. This estimate was deliberately conservative because of ourintent to analyze these data primarily using either a model with patient-level
diagnosis was more frequent in patients randomly assigned to
random effects or another appropriate regression technique (such as GEE).
receive placebo. The mean interval between visits (in weeks) wassimilar for patients in each treatment arm. The patients’ cancer
treatments are listed in Table 3. There were significantly more
The baseline questionnaires were completed by 159 patients
fluoxetine patients currently receiving radiation therapy, and more
(98%), and at least one follow-up assessment was completed by
placebo patients had undergone surgery.
129 patients (81%). The baseline characteristics of the 30
Patient compliance to the study drug was not assessed with
patients who did not complete at least one follow-up are listed in
pill counts but by patient self-report at follow-up. Six patients
Table 1. Patients who completed at least one follow-up assess-
discontinued the study drug (3.7%). Four patients dropped out of
ment were assessable for the primary outcome variable of
the fluoxetine arm (two because of daily headaches and two
because of nausea or vomiting), and two patients dropped out of
Table 1. Baseline Assessments of the Assessable and Inassessable Patients
NOTE. t tests are used to test for differences of means. Abbreviations: TQSS, Two-Question Screening Survey; ECOG PS, Eastern Cooperative Oncology Group performance
status; FACT-G, Functional Assessment of Cancer Therapy–General; BZSDS, Brief Zung Self-Rating Depression Scale.
*Missing baseline TQSS data were the result of a systematic error, but 75% of the data were retrieved by subsequent
†Higher scores represent better quality of life. ‡Higher scores represent more severe depression.
Information downloaded from jco.ascopubs.org and provided by Indiana University School of Medicine Libraries on July 23,
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Table 2. Patient Characteristics Table 4. Longitudinal Data on Quality of Life and Depressive Symptoms
Abbreviations: FACT-G, Functional Assessment of Cancer Therapy–General;
BZSDS, Brief Zung Self-Rating Depression Scale.
*Numbers in parentheses represent the number of patients in the fluoxetine group
the study completion visit, compared with two (4.6%) of 43
The longitudinal data regarding QOL are listed in Table 4. The
pattern of missing data was similar in the two groups. There were
no significant differences in the best-change scores for the
FACT-G or BZSDS between the groups or in the proportion of
responders whose best-change score exceeded the 6-point
threshold for the FACT-G (Table 5). Moreover, the FACT-Gsubscales (functional, social, emotional, and physical well-being) showed similar best-change score findings, as summa-
the placebo arm (one because of nonspecific side effects and one
because of nausea or vomiting). Fifteen patients had unexpected
There was a statistically significant improvement in the total
hospitalizations during the study; nine in the fluoxetine arm and
FACT-G scores in the fluoxetine group, compared with the
six in the placebo arm (P ϭ .59 by two-sided Fisher’s exact test).
placebo group, using the GEE method of regression (P ϭ .05).
To assess a common side effect of fluoxetine, clinicians were
This difference remained highly significant after multivariate
asked to report at each follow-up the number of times the patient
adjustments were made for age, sex, the two-question screening
vomited in the past week. There was no difference in the
score, performance status, family history of depression, and
frequency of emesis for the second, third, and fourth visits, but
current cancer therapy (P ϭ .01). The fluoxetine group also
the frequency was significantly greater in patients in the fluox-
improved significantly, compared with placebo, on the depres-
etine arm at the study completion visit; nine (33%) of 27 patients
sion scale (P ϭ .0005). The full GEE model characteristics for
in the fluoxetine arm reported one or more episodes of emesis at
depression and QOL are listed in Table 7. In both the QOL and
Table 3. Cancer Treatment Exposure of the Study Population
Information downloaded from jco.ascopubs.org and provided by Indiana University School of Medicine Libraries on July 23,
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
FLUOXETINE VERSUS PLACEBO IN CANCER PATIENTS
Table 5. Best-Change Scores for Quality of Life and Depression
of the GEE model, but there were no significant differences in
the mean best-change scores for any of the subscales.
The TQSS score was less than 4 in 32% of the patients. In this
subgroup, the GEE model showed no treatment effect on QOL
(P ϭ .19) or depression (P ϭ .35). However, the treatment effect
was more pronounced in the subset of patients whose TQSS
score was 4 or greater, with significant improvement in QOL
ϭ .05) and depression (P ϭ .0008). This subgroup analysis on
the basis of the TQSS was unplanned and is considered explor-
atory. The conclusions were the same when the subset analysis
was performed using the baseline BZSDS data dichotomized by
those patients scoring in the normal range (0 to 21; 64 patients)
versus patients with mild or moderate depression at baseline
The survival of the treatment groups is illustrated using the
NOTE. Higher scores represent better health for the FACT-G, but lower scores (or
more negative best-change scores) represent better health (less depressive symptoms)
Kaplan-Meier method in Fig 2. An eligibility requirement for
this study was a projected survival between 3 and 24 months.
Abbreviations: FACT-G, Functional Assessment of Cancer Therapy–General;
Sixty-four percent of patients (102 of 160 patients) had a
BZSDS, Brief Zung Self-Rating Depression Scale.
survival in that projected range. Twenty-three percent of patients
*The best-change score refers to the difference between the baseline total score
(37 of 160 patients) survived fewer than 3 months, and three
and the average of the best consecutive scores on the respective instruments (FACT-Gfor quality of life or BZSDS for depression).
patients were lost to follow-up for survival. The median survival
of the patients is listed according to the category of clinician-
‡Responders were those patients whose best-change score was Ն 6 points for the
This study is the first to explore an oncologist-driven, symp-
tom-management solution to the prevalent problem of depressive
depression model, female sex was associated with significantly
symptoms in advanced cancer patients. To our knowledge, it is
better outcomes (P ϭ .004 for QOL and P ϭ .04 for depression).
also the largest study examining the placebo response rate
Moreover, the TQSS was a significant predictor of overall QOL
associated with the FACT-G instrument for QOL assessment of
and depression (P ϭ .001 and P ϭ .01, respectively), having a
outpatients with advanced cancer. Our findings show that simple
stronger association with both outcomes (QOL and depression)
symptom screening followed by antidepressant treatment is both
than did performance status. Patients with no family history of
feasible and associated with improvement in overall QOL and
depression had less depression (P ϭ .02). Two subscales of the
FACT-G, social well-being and emotional well-being, showed
The overall benefit to QOL in the fluoxetine arm, although
statistically significant improvement with fluoxetine on the basis
statistically significant, is of uncertain clinical significance be-
Table 6. FACT-G Subscales: Best-Change Scores and GEE Results
Abbreviations: FACT-G, Functional Assessment of Cancer Therapy–General; GEE, generalized estimating
equations; FWB, functional well-being; SWB, social well-being; EWB, emotional well-being; PWB, physicalwell-being.
*The results are obtained from GEE models for FACT-G subscales with adjustment of a set of covariates. Slope
estimates indicate the outcome improvement in the fluoxetine group with the placebo group as a reference.
†P is for test of significance of differences of means.
Information downloaded from jco.ascopubs.org and provided by Indiana University School of Medicine Libraries on July 23,
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Table 7. Generalized Estimating Equations for the FACT-G and BZSDS
NOTE. Age, TQSS, and ECOG performance status were considered continuous variables in this model. Abbreviations: FACT-G, Functional Assessment of Cancer Therapy–General; BZSDS, Brief Zung Self-Rating Depression Scale; CL,
confidence limits; TQSS, Two-Question Screening Survey; ECOG PS, Eastern Cooperative Oncology Group Performance Status.
cause the proportion of patients with a 6-point difference in their
kind of clinical problem. Somerfield et al30 have argued persua-
best-change score, indicating clinically important improvement,
sively that a more reasonable expectation of an intervention is
did not differ between the treatment arms. Determining the
that it would be effective at the more proximal target problem (in
clinical significance of changes in self-reported health measures
this case depression) rather than a more distal, global outcome
measured longitudinally is difficult, and this is an area of active
such as overall QOL. This was indeed borne out in our study, in
research and debate.29 The best-change score represented an
which there was a more convincing proximal effect of the
attempt to provide a very conservative summary of change of
antidepressant (decrease in the depressive symptoms) and a
longitudinal data that was both meaningful and simple to
statistically significant but less convincing distal effect. It seems
calculate. By taking the difference between the baseline measure
that the depressive symptoms did not abate as the result of
and the average of the best consecutive measures, this method
adaptation and regression to the mean but, instead, as a result of
gives greater weight to any sustained improvements and dis-
a real effect from the antidepressant. In addition, for those who
counts the treatment effect when there are missing data. If there
might speculate that use of an antidepressant might cause the
had been a significant difference between the treatment arms
average patient worse problems than the depression itself be-
with this best-change score method, the clinical significance of
cause of polypharmacy, drug interactions, or antidepressant side
the statistical findings would have been convincing, but it is
effects, there are reassuring data that the overall QOL was
clearly more difficult to interpret a no-difference result. There-
fore, more research is needed to validate this method.
Just as overall QOL might be regarded as a distal outcome for
In addition to the controversy surrounding the definition of
an antidepressant trial, survival would be even more distal.
clinically significant changes, there is also controversy regarding
Survival was measured in this trial as a descriptive end point to
the appropriate use and interpretation of QOL end points in
better understand this patient population and its generalizability
studies in which the intervention is expected to affect a specific
to other groups of patients. As expected, there was no differencein survival between the treatment arms.
Since United States Food and Drug Administration approval of
fluoxetine in 1987, there has been a national trend toward greateruse of psychotropic drugs and greater involvement of physicians inthe management of depression in outpatients.31 Thus, our data maybroaden the comfort zone of oncologists for prescribing antidepres-sants for some patients. A particular factor favoring the use ofantidepressants in patients with advanced cancer is that access tobehavioral health professionals and psychologic interventions is notalways feasible for very sick patients. It is also important that theTQSS proved to be quite easy to adapt to clinical practice as an
Table 8. Comparison of Clinician-Expected Survival With Estimated Survival Fig 2. Estimated survival. The overall median survival of this patient population was 7.77 months. The median survival in the fluoxetine group was 6.26 months compared with 9.39 months in the placebo group (P ؍ .50 by the log-rank test).
Information downloaded from jco.ascopubs.org and provided by Indiana University School of Medicine Libraries on July 23,
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
FLUOXETINE VERSUS PLACEBO IN CANCER PATIENTS
initial assessment of psychologic distress. The exploratory analysis
cancer outpatient research, and it was no worse in this study than
revealed that the subset of patients with mild or moderate depressive
in other similar studies. Nevertheless, nonrandom reasons for
symptoms (on the basis of the baseline TQSS or the baseline
missing data introduce possible bias into this study. Although
BZSDS) benefited the most from the fluoxetine intervention.
new methods for the analysis of studies with missing data such
Therefore, the TQSS, as an example of simple bedside screening, is
as this study are being explored, more important innovations for
worthy of additional research as a predictor of response to antide-
preventing missing data also are being pursued. Better funding
pressant therapy in this population.
for symptom research projects and use of telephone assessments
Selection bias is one of several important limitations to this
may lessen the missing data problem in future research.
study. These 163 patients were enrolled over a period of 30
In summary, this study demonstrated that simple two-question
months and represent a small fraction of the total eligible
screening for depressive symptoms followed by treatment with a
patients. The pace of accrual was affected by the physicians’ lack
once-a-day pill proved effective in identifying and treating
of familiarity with placebo-controlled symptom research, and
depressive symptoms and, hence, improving QOL in patients
there was a substantial learning curve in this regard. More
important, collecting questionnaire data using existing officestaff is cumbersome and was not always feasible on a day-to-day
basis. This group’s willingness to pursue this research is a credit
We thank the nurses and physicians of the Hoosier Oncology Group and
to oncologists and their drive to learn more about their patients’
study design consultants Ian Tannock, PhD, and Jimmie Holland, MD, and
psychologic distress. Another important limitation was the sub-
we acknowledge the generosity and courage of the patients who agreed to
stantial missing data. This is an inherent problem in advanced
1. Foley KM, Gelband H (eds): Improving Palliative Care for Cancer:
17. Holland J, Romano S, Heiligenstein J, et al: A controlled trial of
Summary and Recommendations. Washington, DC, National Academy
fluoxetine and desipramine in depressed women with advanced cancer.
2. Massie MJ, Popkin MK: Depressive disorders, in Holland JC (ed):
18. Razavi D, Allilaire J, Smith M, et al: The effect of fluoxetine on
Psycho-Oncology. New York, NY, Oxford University Press, 1998, 518-540
anxiety and depression symptoms in cancer patients. Acta Psychiatr Scand
3. Wilson KG, Chochinov HM, de Faye B, et al: Diagnosis and manage-
ment of depression in palliative care, in Chochinov HM, Breitbart W (eds):
19. van Heeringen K, Zivkov M: Pharmacological treatment of depression
Handbook of Psychiatry in Palliative Care. Oxford, United Kingdom, Oxford
in cancer patients: A placebo-controlled study of mianserin. Br J Psychiatry
4. Lloyd-Williams, M: Screening for depression in palliative care. Am J
20. Eija K, Tiina T, Pertti NJ: Amitriptyline effectively relieves neuro-
pathic pain following treatment of breast cancer. Pain 64:293-302, 1996
5. Williams JW Jr, Noel PH, Cordes JA, et al: Is this patient clinically
21. Purohit DR, Navlakha PL, Modi RS, et al: The role antidepressants in
depressed? J Am Med Assoc 287:1160-1170, 2002
hospitalised cancer patients: A pilot study. J Assoc Physicians India
6. Passik SD, Dugan W, McDonald MV, et al: Oncologists’ recognition of
depression in their patients with cancer. J Clin Oncol 16:1594-1600, 1998
22. Costa D, Mogos I, Toma T: Efficacy and safety of mianserin in the
7. Passik SD, Kirsh K, Donaghy KB, et al: An attempt to employ the Zung
treatment of depression of women with cancer. Acta Psychiatr Scand
Self-Rating Depression Scale as a “lab test” to trigger follow-up in
ambulatory oncology clinics: Criterion validity and detection. J Pain Symp-
23. Musselman DL, Lawson DH, Gumnick JF, et al: Paroxetine for the
prevention of depression induced by high-dose interferon alfa. N Engl J Med
8. Whooley M, Avins A, Miranda J, et al: Case-finding instruments for
depression: Two questions are as good as many. J Gen Intern Med
24. Cella DF, Tulsky DS, Gray G, et al: The Functional Assessment of
Cancer Therapy Scale: Development and validation of the general measure.
9. Chochinov H, Wilson K, Enns M, et al: “Are you depressed?” Screening
for depression in the terminally ill. Am J Psychiatry 154:674-676, 1997
25. Brady MJ, Peterman AH, Fitchett G, et al: A case for including
10. Fisch M, Marx R, Brames M, et al: Use of a two-question screening
spirituality in quality of life measurement in oncology. Psychooncology
survey for depression in outpatients with advanced cancer. Proc Am Soc Clin
26. Liang KY, Zeger SL: Longitudinal data analysis using generalized
11. Whooley MA, Simon GE: Managing depression in medical outpa-
27. Matthews JN, Altman DG, Campbell MJ, et al: Analysis of serial
12. Williams JW Jr, Barrett J, Oxman T, et al: Treatment of dysthymia
measurements in medical research. Br Med J 300:230-235, 1990
and minor depression in primary care: A randomized controlled trial in older
28. Tannock IF, Osoba D, Stockler MR, et al: Chemotherapy with
adults. J Am Med Assoc 284:1519-1526, 2000
mitoxantrone plus prednisone or prednisone alone for symptomatic hormone-
13. Breitbart W: Psycho-oncology: Depression, anxiety, delirium. Semin
resistant prostate cancer: A Canadian randomized trial with palliative end
14. Evans DL, McCartney CF, Haggerty JJ Jr, et al: Treatment of
29. Sloan JA, Cella D, Frost M, et al: Assessing clinical significance in mea-
depression in cancer patients is associated with better life adaptation: A pilot
suring oncology patient quality of life: Introduction to the symposium, con-
tent overview, and definition of terms. Mayo Clin Proc 77:367-370, 2002
15. Massie M, Holland J: Depression and the cancer patient. J Clin
30. Somerfield M, Jatoi A, Nguyen PL, et al: Hazards of quality of life
data for clinical decision making. J Clin Oncol 19:594-595, 2001
16. Mermelstein H, Lesko L: Depression in patients with cancer. Psy-
31. Olfson M, Marcus SC, Druss B, et al: National trends in the outpatient
treatment of depression. J Am Med Assoc 287:203-209, 2002
Information downloaded from jco.ascopubs.org and provided by Indiana University School of Medicine Libraries on July 23,
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Fortbildung Laktose in Pille & Co. Was tun bei Patientinnen Die Aufnahme von Laktose über Medikamente wird von Frauen mit einer Laktoseintoleranz bisweilen als potenzielles Problem die unter einer Laktoseintoleranz leiden, angesehen oder führt zumindest zu Verunsicherung. Jedoch stellt die Zufuhr von Laktose insbesondere mit gynäkologischen Arznei-Thema besitzen und darauf ach
LEGI, DECRETE, HOTĂRÂRI ȘI ALTE ACTE stat pentru dezvoltarea regională prin sprijinireainvestițiilor în turism din cadrul Programului operațional 1.055. — Hotărâre privind darea în administrarea MinisteruluiSănătății a unor imobile transmise în domeniul public al statului . — Ordin al ministrului transporturilor și infrastructuriipentru modificarea anexelor la Ordinul
 FLUOXETINE VERSUS PLACEBO IN CANCER PATIENTS
Fig 1. Study flow.
FLUOXETINE VERSUS PLACEBO IN CANCER PATIENTS
Fig 1. Study flow.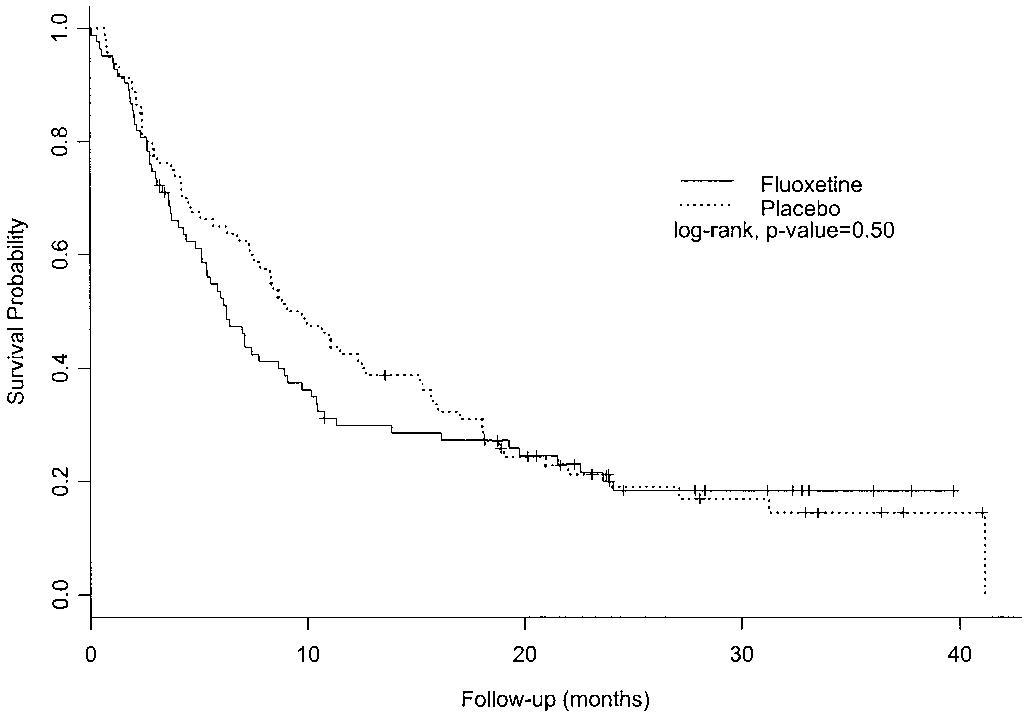 Table 7. Generalized Estimating Equations for the FACT-G and BZSDS
Table 7. Generalized Estimating Equations for the FACT-G and BZSDS