Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Doi:10.1016/j.radonc.2004.03.016
Radiotherapy and Oncology 72 (2004) 83–85
Undifferentiated sinonasal carcinoma may respond to single-fraction
Mauri Kouria,l,*, Leena Kankaanrantaa,l, Tiina Seppa¨la¨g,l, Leena Tervob, Merja Rasilainenc,
Heikki Minni, Olli Eskolaj, Jyrki Va¨ha¨taloh, Anders Paetaud, Sauli Savolainenb,f,l,
Iiro Auterinenk, Juha Ja¨a¨skela¨inene, Heikki Joensuua,l
aDepartment of Oncology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
bDepartment of Laboratory Diagnostics, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
cDepartment of Pharmacy, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, FinlanddDepartment of Pathology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
eDepartment of Neurosurgery, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
fDepartment of Radiology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
gDepartment of Physical Sciences, University of Helsinki, Helsinki, Finland
hLaboratory of Radiochemistry, University of Helsinki, Helsinki, Finland
iDepartment of Oncology and Radiotherapy, University of Turku, Turku, Finland
jTurku PET Centre, University of Turku, Turku, Finland
kVTT Processes, Technical Research Centre of Finland, P.O. Box 1608, FIN-02044 VTT, Finland
lBoneca Corporation, Haartmaninkatu 8, FIN-00290 Helsinki, Finland
Received 14 January 2004; received in revised form 23 February 2004; accepted 15 March 2004
A large, rapidly progressing, unresectable undifferentiated sinonasal head and neck carcinoma regressed rapidly following single fraction
boron neutron capture therapy (BNCT). The main toxicity consisted of mucositis lasting for a few days. The quality of life improved and wasexcellent until tumour recurrence 6 months after the date of BNCT.
q 2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Boron neutron capture therapy; Head and neck carcinoma; Sinonasal carcinoma; Boronophenylalanine; Positron emission tomography
Boron neutron capture therapy (BNCT) is based on a
treatment of other human tumours than glioblastomas and
nuclear capture reaction that occurs when boron-10 captures
melanomas We describe here a patient whose sinonasal
a low energy (, 0.5 eV) neutron, which results in
undifferentiated carcinoma (SNUC) recurred in spite of
production of a high energy a particle and a lithium ion.
repeated surgery and photon radiation therapy but
Low energy (thermal) neutrons can be produced by
responded remarkably well to a single fraction of L-BPA
irradiating the target with neutrons of epithermal energy
(0.5 – 10 keV) . At present, epithermal neutron beams
A 44-year-old male was admitted to the Department of
used for BNCT exist only at nuclear research reactors,
Oncology, Helsinki University Central Hospital, in January
which has limited the availability of BNCT .
2003 with a progressing SNUC. The patient had undergone
Boron-10 is delivered into the tumour using a carrier
supraorbital craniotomy with a grossly complete tumour
molecule, such as 4-dihydroxyboryl-L-phenylalanine
removal in August 2001. Pathological examination revealed
(L-BPA). L-BPA is administered as an anionic fructose
an undifferentiated large cell carcinoma compatible with
complex (BPA-F) prior to neutron irradiation to improve
the diagnosis of SNUC. Most tumour cells expressed cyto-
solubility Thus far BNCT has not been evaluated in the
keratin in immunostaining, and were negative for chromo-granin, synaptophysin, S-100, HMB-45, and the leukocyte
common antigen (LCA). The patient received postoperative
0167-8140/$ - see front matter q 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.radonc.2004.03.016
M. Kouri et al. / Radiotherapy and Oncology 72 (2004) 83–85
radiotherapy to a total cumulative dose of 50.4 Gy using
described elsewhere was injected as a 15-s bolus into a
1.8 Gy daily fractions with concurrent weekly cisplatin
peripheral vein 20-min prior to imaging. The injected tracer
40 mg/m2 in September to October 2001. Magnetic
activities were 259 and 372 MBq, respectively, in PET
resonance imaging (MRI) revealed a recurrent intraorbital
studies carried out prior to and after BNCT. Tracer
mass that extended to the floor of the anterior cranial fossa
accumulation in the regions of interest (ROIs) was measured
in April 2002. He underwent craniotomy, where the tumour
as the standardized uptake value (SUV) In the
and the right eye were removed, followed by a micro-
pretreatment PET study the average SUV of [18F]FBPA in
vascular muscle flap reconstruction in June 2002. A large
the entire tumour over the 6 planes showing the highest
recurrent tumour growing on the dural linings and extending
activity ranged from 4.8 to 5.7 (maximum, 6.4 to 7.8), while
into the frontal lobe was found in MRI 4 months later. The
that of the contralateral frontal lobe grey matter ranged only
tumour was considered unresectable, and progressed rapidly
from 0.8 to 1.0. This suggested that a sufficient BPA uptake
forming cysts in the right frontal lobe and causing a midline
gradient was likely to be achieved in the tumour relative to
shift panel A). Since no effective standard treatment
the adjacent normal structures for successful BNCT (,
was available, experimental therapy with BNCT was
panel A). Of the normal tissue sites, the highest SUV was
considered. An Institutional Review Board and the National
measured in the palatine mucosa ranging from 3.3 to 4.3.
Agency for Medicines agreed with carrying out the BNCT
BNCT was given as a single fraction therapy at the FiR 1
procedure. The patient signed an informed consent.
reactor facility, Espoo, Finland, on February 25, 2003 .
Tumour BPA uptake was first assessed with positron
L-BPA (purchased from Katchem Ltd, Praque, Czech
emission tomography (PET) using fluorine-18 labelled
Republic) was complexed with fructose and BPA-F
4-dihydroxyboryl-2-[18F]fluoro-L-phenylalanine
was given at the dose of 400 mg/kg L-BPA as a 2-h
([18F]FBPA), as the tracer. [18F]FBPA, synthesized as
intravenous infusion, following which epithermal neutronswere delivered using 2 circular 14-cm-diameter beams withirradiation times of 15.3 and 16.5 min. The blood boronconcentration was monitored with inductively coupledplasma-atomic emission spectrometry (ICP-AES) . The peak blood boron concentration was 28 mg/g at the endof the L-BPA-F infusion, and the average concentrationsduring the first and the second irradiation periods were 18.1and 15.9 mg/g, respectively Assuming a brain-to-bloodboron concentration ratio of 1:1, the calculated normal brainphysical peak boron capture, nitrogen capture, fast neutron,and gamma doses were 3.3, 0.39, 0.12, and 2.3 Gy,respectively. Carbamazepine and dexamethasone weregiven to prevent brain oedema and seizures.
A marked shrinkage of the contrast enhancing tumour
was found in an MRI performed 2 weeks after BNCT (,panel B). Practically all visible tumour had regressed inMRI studies performed 1 and 2 months following BNCT,although some patchy contrast enhancement was stillpresent at the tumour site in the ethmoidal region (,panel C). A large frontal tumour with a metabolically active
Fig. 1. Axial and sagittal T1 weighted MRI showing the response of
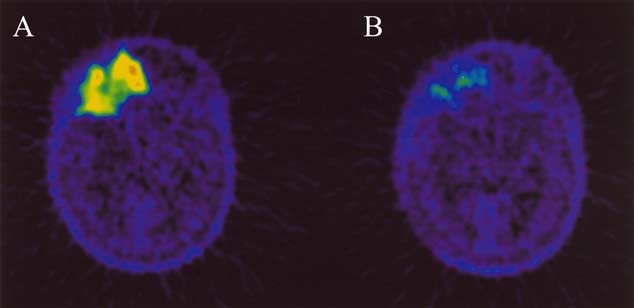
Fig. 2. Positron emission tomography using 18F-labelled boronophenyla-
sinonasal undifferentiated carcinoma to single-fraction BNCT. MR images
lanine (BPA) as the tracer. Left: a PET image taken prior to BNCT; right:
taken prior to BNCT (A), and images taken 2 weeks (B) and 2 months (C)
an image taken 7 weeks after single-fraction BNCT showing a marked
M. Kouri et al. / Radiotherapy and Oncology 72 (2004) 83–85
volume measuring 62 £ 66 £ 90 mm3 and a small separate
tumour focus in the right temporal lobe were present in thepretreatment [18F]FBPA PET scan taken 3 weeks prior to
[1] Barth RF. A critical assessment of boron neutron capture therapy: an
BNCT. In an [18F]FBPA PET study performed 7 weeks after
overview. J Neurooncol 2003;62:1 – 5.
[2] Busse PM, Harling OK, Palmer MR, et al. A critical examination of
BNCT the mean tumour activity had decreased markedly,
the results from the Harvard – MIT NCT program phase I clinical trial
and the tumour SUV now ranged only from 1.9 to 2.5
of neutron capture therapy for intracranial disease. J Neurooncol
(maximum, 2.6 to 3.3, panel B). In addition, the small
active focus in the right temporal lobe disappeared (not
[3] Capala J, Stenstam BH, Skold K, et al. Boron neutron capture therapy
for glioblastoma multiforme: clinical studies in Sweden. J Neurooncol2003;62:135 – 44.
BNCT was generally well tolerated. Grade 1 skin
[4] Coderre JA, Morris GM. The radiation biology of boron neutron
erythema and temporal subcutaneous edema were present
capture therapy. Radiat Res 1999;151:1 – 18.
during the first few days following BNCT The patient
[5] Common toxicity criteria manual, Version 2.0. National Cancer
was hospitalized 9 days after BNCT for 5 days because of
grade 3 vomiting and oral mucositis. Hair loss was complete
[6] Diaz AZ. Assessment of the results from the phase I/II boron neutron
capture therapy trials at the Brookhaven National Laboratory from a
on the right temporal and parietal scalp. Only transient
clinician’s point of view. J Neurooncol 2003;62:101– 9.
grade 2 fatigue, and purulent rhinitis lasting for a few days
[7] Eckelman WC, Tatum JL, Kurdziel KA, Croft BY. Quantitative
and requiring antibiotics were recorded as probable BNCT-
analysis of tumor biochemisty using PET and SPECT. Nucl Med Biol
related adverse events during the first 4 months of follow-
up. The quality of life post-BNCT was excellent, and the
[8] Gorelick J, Ross D, Marentette L, Blaivas M. Sinonasal undiffer-
entiated carcinoma: case series and review of the literature.
patient returned to work for 5 months until the tumour
Neurosurgery 2000;47:750– 4. discussion, 754 – 5.
recurred 6 months after the date of BNCT. Brain metastases
[9] Gupta N, Gahbauer RA, Blue TE, Albertson B. Common challenges
were found at the time of treatment failure.
and problems in clinical trials of boron neutron capture therapy of
The present data suggest that previously irradiated head
brain tumors. J Neurooncol 2003;62:197 – 210.
and neck carcinomas may be retreated with single fraction
[10] Jeng YM, Sung MT, Fang CL, et al. Sinonasal undifferentiated
carcinoma and nasopharyngeal-type undifferentiated carcinoma: two
BNCT with acceptable acute toxicity. Since the estimated
clinically, biologically, and histopathologically distinct entities. Am J
radiation dose to the normal structures may remain low,
little late toxicity is expected from such therapy. Based on
[11] Joensuu H, Kankaanranta L, Seppa¨la¨ T, et al. Boron neutron capture
the encouraging response achieved in this single patient, we
therapy of brain tumors: clinical trials at the finnish facility using
have now initiated a phase I study on BPA-based BNCT in
boronophenylalanine. J Neurooncol 2003;62:123 – 34.
[12] Kulvik M, Va¨ha¨talo J, Buchar E, et al. Clinical implementation of
the treatment of patients with inoperable, locally advanced
4-dihydroxyborylphenylalanine synthesised by an asymmetric path-
head and neck carcinoma who have prior photon radiation
way. Eur J Pharm Sci 2003;18:155 – 63.
[13] Laakso J, Kulvik M, Ruokonen I, et al. Atomic emission method for
total boron in blood during neutron-capture therapy. Clin Chem 2001;47:1796 – 803.
[14] Musy PY, Reibel JF, Levine PA. Sinonasal undifferentiated
carcinoma: the search for a better outcome. Laryngoscope 2002;112:1450– 5.
The expenses of the boron neutron capture treatment
[15] Nakagawa Y, Pooh K, Kobayashi T, et al. Clinical review of the
Japanese experience with boron neutron capture therapy and a
were covered by Boneca Corporation, owned by Clinical
proposed strategy using epithermal neutron beams. J Neurooncol
Research Institute HUCH Ltd, Finnish National Fund for
Research and Development Sitra and VTT Technical
[16] Ryyna¨nen PM, Kortesniemi M, Coderre JA, et al. Models for
Research Centre. This work was supported by the Helsinki
estimation of the (10)B concentration after BPA-fructose complex
University Central Hospital Research Funds (H.J.), and
infusion in patients during epithermal neutron irradiation in BNCT. Int J Radiat Oncol Biol Phys 2000;48:1145– 54.
Academy of Finland (S.S., T.S.). The authors thank Mika
[17] Va¨ha¨talo J, Eskola O, Bergman J, et al. Synthesis of 4-dihydrox-
Kortesniemi, Petri Kotiluoto and Jouni Uusi-Simola for
yboryl-2[18F]fluorophenylalanine with relatively high specific
activity. J Label Compd Radiopharm 2002;45:697 – 704.
Casa di Cura Ambrosiana S.p.a. ISTRUZIONE OPERATIVA PREPARAZIONE ALLA COLONSCOPIA • Nei 7 giorni che precedono l’esame evitare accuratamente frutta, verdura e cibi integrali. Aumentare • Nei 3 giorni che precedono la vigilia dell’esame, assumere alla sera una compressa di purgante (es • Sospendere eventuali terapie a base di ferro almeno 2 giorni prima dell’esame. •
Canadian Pharmaceutical Corporation® Products CPC PRODUCTS BRANDED NAMES CPC PRODUCT DESCRIPTION CPC TABLET/CAPSULE IMAGES Off white, round, beveled edge, unscored film coated tablet with "CPC" over "200" engraved on one side of the tablet and blank on the CPC-ALBENDAZOLE 200MG TABS Albenza ® other side of the tablet. White, octagonal shape, un-c
 Radiotherapy and Oncology 72 (2004) 83–85
Undifferentiated sinonasal carcinoma may respond to single-fraction
Mauri Kouria,l,*, Leena Kankaanrantaa,l, Tiina Seppa¨la¨g,l, Leena Tervob, Merja Rasilainenc,
Heikki Minni, Olli Eskolaj, Jyrki Va¨ha¨taloh, Anders Paetaud, Sauli Savolainenb,f,l,
Iiro Auterinenk, Juha Ja¨a¨skela¨inene, Heikki Joensuua,l
aDepartment of Oncology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
bDepartment of Laboratory Diagnostics, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
cDepartment of Pharmacy, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, FinlanddDepartment of Pathology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
eDepartment of Neurosurgery, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
fDepartment of Radiology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
gDepartment of Physical Sciences, University of Helsinki, Helsinki, Finland
hLaboratory of Radiochemistry, University of Helsinki, Helsinki, Finland
iDepartment of Oncology and Radiotherapy, University of Turku, Turku, Finland
jTurku PET Centre, University of Turku, Turku, Finland
kVTT Processes, Technical Research Centre of Finland, P.O. Box 1608, FIN-02044 VTT, Finland
lBoneca Corporation, Haartmaninkatu 8, FIN-00290 Helsinki, Finland
Received 14 January 2004; received in revised form 23 February 2004; accepted 15 March 2004
A large, rapidly progressing, unresectable undifferentiated sinonasal head and neck carcinoma regressed rapidly following single fraction
boron neutron capture therapy (BNCT). The main toxicity consisted of mucositis lasting for a few days. The quality of life improved and wasexcellent until tumour recurrence 6 months after the date of BNCT.
Radiotherapy and Oncology 72 (2004) 83–85
Undifferentiated sinonasal carcinoma may respond to single-fraction
Mauri Kouria,l,*, Leena Kankaanrantaa,l, Tiina Seppa¨la¨g,l, Leena Tervob, Merja Rasilainenc,
Heikki Minni, Olli Eskolaj, Jyrki Va¨ha¨taloh, Anders Paetaud, Sauli Savolainenb,f,l,
Iiro Auterinenk, Juha Ja¨a¨skela¨inene, Heikki Joensuua,l
aDepartment of Oncology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
bDepartment of Laboratory Diagnostics, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
cDepartment of Pharmacy, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, FinlanddDepartment of Pathology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
eDepartment of Neurosurgery, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
fDepartment of Radiology, Helsinki University Central Hospital, P.O. Box 180, FIN-00029 HUCH, Finland
gDepartment of Physical Sciences, University of Helsinki, Helsinki, Finland
hLaboratory of Radiochemistry, University of Helsinki, Helsinki, Finland
iDepartment of Oncology and Radiotherapy, University of Turku, Turku, Finland
jTurku PET Centre, University of Turku, Turku, Finland
kVTT Processes, Technical Research Centre of Finland, P.O. Box 1608, FIN-02044 VTT, Finland
lBoneca Corporation, Haartmaninkatu 8, FIN-00290 Helsinki, Finland
Received 14 January 2004; received in revised form 23 February 2004; accepted 15 March 2004
A large, rapidly progressing, unresectable undifferentiated sinonasal head and neck carcinoma regressed rapidly following single fraction
boron neutron capture therapy (BNCT). The main toxicity consisted of mucositis lasting for a few days. The quality of life improved and wasexcellent until tumour recurrence 6 months after the date of BNCT.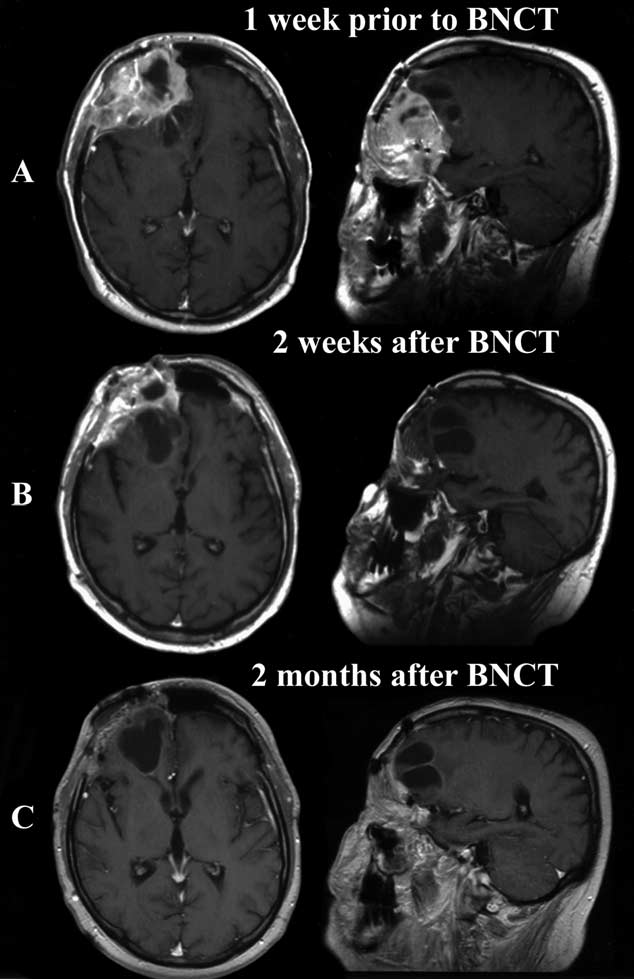
 M. Kouri et al. / Radiotherapy and Oncology 72 (2004) 83–85
radiotherapy to a total cumulative dose of 50.4 Gy using
described elsewhere was injected as a 15-s bolus into a
1.8 Gy daily fractions with concurrent weekly cisplatin
peripheral vein 20-min prior to imaging. The injected tracer
40 mg/m2 in September to October 2001. Magnetic
activities were 259 and 372 MBq, respectively, in PET
resonance imaging (MRI) revealed a recurrent intraorbital
studies carried out prior to and after BNCT. Tracer
mass that extended to the floor of the anterior cranial fossa
accumulation in the regions of interest (ROIs) was measured
in April 2002. He underwent craniotomy, where the tumour
as the standardized uptake value (SUV) In the
and the right eye were removed, followed by a micro-
pretreatment PET study the average SUV of [18F]FBPA in
vascular muscle flap reconstruction in June 2002. A large
the entire tumour over the 6 planes showing the highest
recurrent tumour growing on the dural linings and extending
activity ranged from 4.8 to 5.7 (maximum, 6.4 to 7.8), while
into the frontal lobe was found in MRI 4 months later. The
that of the contralateral frontal lobe grey matter ranged only
tumour was considered unresectable, and progressed rapidly
from 0.8 to 1.0. This suggested that a sufficient BPA uptake
forming cysts in the right frontal lobe and causing a midline
gradient was likely to be achieved in the tumour relative to
shift panel A). Since no effective standard treatment
the adjacent normal structures for successful BNCT (,
was available, experimental therapy with BNCT was
panel A). Of the normal tissue sites, the highest SUV was
considered. An Institutional Review Board and the National
measured in the palatine mucosa ranging from 3.3 to 4.3.
M. Kouri et al. / Radiotherapy and Oncology 72 (2004) 83–85
radiotherapy to a total cumulative dose of 50.4 Gy using
described elsewhere was injected as a 15-s bolus into a
1.8 Gy daily fractions with concurrent weekly cisplatin
peripheral vein 20-min prior to imaging. The injected tracer
40 mg/m2 in September to October 2001. Magnetic
activities were 259 and 372 MBq, respectively, in PET
resonance imaging (MRI) revealed a recurrent intraorbital
studies carried out prior to and after BNCT. Tracer
mass that extended to the floor of the anterior cranial fossa
accumulation in the regions of interest (ROIs) was measured
in April 2002. He underwent craniotomy, where the tumour
as the standardized uptake value (SUV) In the
and the right eye were removed, followed by a micro-
pretreatment PET study the average SUV of [18F]FBPA in
vascular muscle flap reconstruction in June 2002. A large
the entire tumour over the 6 planes showing the highest
recurrent tumour growing on the dural linings and extending
activity ranged from 4.8 to 5.7 (maximum, 6.4 to 7.8), while
into the frontal lobe was found in MRI 4 months later. The
that of the contralateral frontal lobe grey matter ranged only
tumour was considered unresectable, and progressed rapidly
from 0.8 to 1.0. This suggested that a sufficient BPA uptake
forming cysts in the right frontal lobe and causing a midline
gradient was likely to be achieved in the tumour relative to
shift panel A). Since no effective standard treatment
the adjacent normal structures for successful BNCT (,
was available, experimental therapy with BNCT was
panel A). Of the normal tissue sites, the highest SUV was
considered. An Institutional Review Board and the National
measured in the palatine mucosa ranging from 3.3 to 4.3.