C o py r ig ht , 2 0 0 0 , by t he Ma s s ac h u s e t t s Me d ic a l S o c ie t y
V O L U M E 3 4 2 N U M B E R 1 8 VENTILATION WITH LOWER TIDAL VOLUMES AS COMPARED WITH TRADITIONAL TIDAL VOLUMES FOR ACUTE LUNG INJURY AND THE ACUTE RESPIRATORY DISTRESS SYNDROME
THE ACUTE RESPIRATORY DISTRESS SYNDROME NETWORK*
ABSTRACT Background
and the acute respiratory distress syndrome1
ventilation use tidal volumes of 10 to 15 ml per kilo-
is approximately 40 to 50 percent.2-4 Al-
gram of body weight and may cause stretch-induced
though substantial progress has been made
lung injury in patients with acute lung injury and the
in elucidating the mechanisms of acute lung injury,5
acute respiratory distress syndrome. We therefore
there has been little progress in developing effective
conducted a trial to determine whether ventilation
with lower tidal volumes would improve the clinical
Traditional approaches to mechanical ventilation
use tidal volumes of 10 to 15 ml per kilogram of body
Methods
weight.6 These volumes are larger than those in nor-
acute respiratory distress syndrome were enrolled ina multicenter, randomized trial. The trial compared
mal subjects at rest (range, 7 to 8 ml per kilogram),
traditional ventilation treatment, which involved an
but they are frequently necessary to achieve normal
initial tidal volume of 12 ml per kilogram of predicted
values for the partial pressure of arterial carbon diox-
body weight and an airway pressure measured after
ide and pH. Since atelectasis and edema reduce aer-
a 0.5-second pause at the end of inspiration (plateau
ated lung volumes in patients with acute lung injury
pressure) of 50 cm of water or less, with ventilation
and the acute respiratory distress syndrome,7,8 inspir-
with a lower tidal volume, which involved an initial
atory airway pressures are often high, suggesting the
tidal volume of 6 ml per kilogram of predicted body
presence of excessive distention, or “stretch,” of the
weight and a plateau pressure of 30 cm of water or
aerated lung. In animals, ventilation with the use of
less. The first primary outcome was death before a
large tidal volumes caused the disruption of pulmo-
patient was discharged home and was breathingwithout assistance. The second primary outcome
nary epithelium and endothelium, lung inflammation,
was the number of days without ventilator use from
atelectasis, hypoxemia, and the release of inflamma-
tory mediators.9-14 The release of inflammatory me-
Results
The trial was stopped after the enrollment
diators could increase lung inflammation and cause in-
of 861 patients because mortality was lower in the
jury to other organs.10,15 Thus, the traditional approach
group treated with lower tidal volumes than in the
to mechanical ventilation may exacerbate or perpet-
group treated with traditional tidal volumes (31.0 per-
uate lung injury in patients with acute lung injury and
cent vs. 39.8 percent, P=0.007), and the number of
the acute respiratory distress syndrome and increase
days without ventilator use during the first 28 days
the risk of nonpulmonary organ or system failure.
after randomization was greater in this group (mean[±SD], 12±11 vs. 10±11; P=0.007). The mean tidalvolumes on days 1 to 3 were 6.2±0.8 and 11.8±0.8 mlper kilogram of predicted body weight (P<0.001), re-spectively, and the mean plateau pressures were
The writing committee (Roy G. Brower, M.D., Johns Hopkins Univer-
25±6 and 33±8 cm of water (P<0.001), respectively.
sity, Baltimore; Michael A. Matthay, M.D., University of California, SanFrancisco; Alan Morris, M.D., LDS Hospital, Salt Lake City; David
Conclusions
Schoenfeld, Ph.D., and B. Taylor Thompson, M.D., Massachusetts General
the acute respiratory distress syndrome, mechanical
Hospital, Boston; and Arthur Wheeler, M.D., Vanderbilt University, Nash-
ventilation with a lower tidal volume than is tradition-
ville) assumes responsibility for the overall content and integrity of themanuscript. Address reprint requests to Dr. Brower at the Division of
ally used results in decreased mortality and increas-
Pulmonary and Critical Care Medicine, Johns Hopkins University, 600
es the number of days without ventilator use. (N Engl
*Members of the Acute Respiratory Distress Syndrome (ARDS) Net-
2000, Massachusetts Medical Society.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
The use of lower tidal volumes during ventilation
Ventilator Procedures
in patients with acute lung injury and the acute res-
The volume-assist–control mode was used for the ventilator un-
piratory distress syndrome may reduce injurious lung
til the patient was weaned from the device or for 28 days after
stretch and the release of inflammatory mediators.16-18
randomization on day 0. Because normal lung volumes are predict-ed on the basis of sex and height,26,27 a predicted body weight
However, this approach may cause respiratory aci-
was calculated for each patient from these data.28 The predicted
dosis16,17 and decrease arterial oxygenation19,20 and
body weight of male patients was calculated as equal to 50+
may therefore require changes in the priority of some
0.91(centimeters of height¡152.4); that of female patients was
objectives in the care of these patients. With the tra-
calculated as equal to 45.5+0.91(centimeters of height¡152.4).
ditional approach, the attainment of normal partial
In the group treated with traditional tidal volumes, the initial tid-al volume was 12 ml per kilogram of predicted body weight. This
pressure of arterial carbon dioxide and pH is given
was subsequently reduced stepwise by 1 ml per kilogram of pre-
a higher priority than is protection of the lung from
dicted body weight if necessary to maintain the airway pressure
excessive stretch. With an approach that involves low-
measured after a 0.5-second pause at the end of inspiration (plateau
er tidal volumes, the reverse is true. Uncontrolled
pressure) at a level of 50 cm of water or less. The minimal tidal vol-ume was 4 ml per kilogram of predicted body weight. If the pla-
studies suggested that the use of a lower tidal volume
teau pressure dropped below 45 cm of water, the tidal volume was
would reduce mortality in patients with acute lung
increased in steps of 1 ml per kilogram of predicted body weight
injury and the acute respiratory distress syndrome,17
until the plateau pressure was at least 45 cm of water or the tidal
but the results of four randomized trials of lung-
volume was 12 ml per kilogram of predicted body weight.
protecting ventilation strategies have been conflict-
In the group treated with lower tidal volumes, the tidal volume
was reduced to 6 ml per kilogram of predicted body weight within
ing.21-24 The present trial was conducted to deter-
four hours after randomization and was subsequently reduced
mine whether the use of a lower tidal volume with
stepwise by 1 ml per kilogram of predicted body weight if neces-
mechanical ventilation would improve important clin-
sary to maintain plateau pressure at a level of no more than 30 cm
of water. The minimal tidal volume was 4 ml per kilogram of pre-dicted body weight. If plateau pressure dropped below 25 cm ofwater, tidal volume was increased in steps of 1 ml per kilogram of
predicted body weight until the plateau pressure was at least 25 cm
Patients
of water or the tidal volume was 6 ml per kilogram of predictedbody weight. For patients with severe dyspnea, the tidal volume
Patients were recruited from March 1996 through March 1999
could be increased to 7 to 8 ml per kilogram of predicted body
at the 10 university centers of the Acute Respiratory Distress Syn-
weight if the plateau pressure remained 30 cm of water or less.
drome Network of the National Heart, Lung, and Blood Institute
Plateau pressures were measured with a half-second inspiratory
(the centers are listed in the Appendix). The protocol was approved
pause at four-hour intervals and after changes in the tidal volume
by the institutional review board at each hospital, and informed
or positive end-expiratory pressure. Plateau pressures of more than
consent was obtained from the patients or surrogates at all but
50 cm of water in the patients in the group treated with tradi-
one hospital, where this requirement was waived. A complete de-
tional tidal volumes and of more than 30 cm of water in patients
scription of the methods is available on the World Wide Web (at
in the group treated with lower tidal volumes were allowed if the
www.ardsnet.org) or from the National Auxiliary Publications
tidal volume was 4 ml per kilogram of predicted body weight or
Patients who were intubated and receiving mechanical ventila-
All other objectives and ventilation procedures, including wean-
tion were eligible for the study if they had an acute decrease in
ing, were identical in the two study groups (Table 1). If a patient
the ratio of partial pressure of arterial oxygen to fraction of in-
became able to breathe without assistance but subsequently re-
spired oxygen to 300 or less (indicating the onset of hypoxemia;
quired additional mechanical ventilation within a period of 28 days,
values were adjusted for altitude in Denver and Salt Lake City),
the same tidal-volume protocol was resumed.
bilateral pulmonary infiltrates on a chest radiograph consistent withthe presence of edema, and no clinical evidence of left atrial hy-
Organ or System Failure
pertension or (if measured) a pulmonary-capillary wedge pressure
Patients were monitored daily for 28 days for signs of the fail-
of 18 mm Hg or less.1 Patients were excluded if 36 hours had
ure of nonpulmonary organs and systems.29 Circulatory failure
elapsed since they met the first three criteria; they were younger
was defined as a systolic blood pressure of 90 mm Hg or less or
than 18 years of age; they had participated in other trials within
the need for treatment with any vasopressor; coagulation failure as
30 days before the first three criteria were met; they were preg-
a platelet count of 80,000 per cubic millimeter or less; hepatic fail-
nant; they had increased intracranial pressure, neuromuscular dis-
ure as a serum bilirubin concentration of at least 2 mg per deciliter
ease that could impair spontaneous breathing, sickle cell disease,
(34 µmol per liter); and renal failure as a serum creatinine concen-
or severe chronic respiratory disease; they weighed more than 1 kg
tration of at least 2 mg per deciliter (177 µmol per liter). We cal-
per centimeter of height; they had burns over more than 30
culated the number of days without organ or system failure by sub-
percent of their body-surface area; they had other conditions with
tracting the number of days with organ failure from the lesser of 28
an estimated 6-month mortality rate of more than 50 percent; they
days or the number of days to death. Organs and systems were con-
had undergone bone marrow or lung transplantation; they had
sidered failure-free after patients were discharged from the hospital.
chronic liver disease (as defined by Child–Pugh class C)25; or theirattending physician refused or was unwilling to agree to the use
Plasma Interleukin-6 Concentrations
A centralized interactive voice system was used for randomiza-
Blood samples were obtained from 204 of the first 234 patients
tion. Patients were randomly assigned to receive mechanical ven-
on day 0 and on day 3 for measurement of plasma interleukin-6
tilation involving either traditional tidal volumes or lower tidal
by immunoassay (R & D Systems, Minneapolis). Blood samples
were stored in sterile EDTA-treated glass tubes. Data Collection
*See NAPS document no. 05542 for 15 pages of supplementary materi-
al. To order, contact NAPS, c/o Microfiche Publications, 248 Hempstead
Data on demographic, physiologic, and radiographic character-
istics, coexisting conditions, and medications were recorded with-
V E N T I L AT I O N W I T H L OW E R T I DA L VO LU M E S I N PAT I E N T S W I T H T H E AC U T E R E S P I R ATO RY D I ST R E S S SY N D R O M E TABLE 1. SUMMARY OF VENTILATOR PROCEDURES.* GROUP RECEIVING GROUP RECEIVING TRADITIONAL TIDAL LOWER TIDAL VARIABLE
Initial tidal volume (ml/kg of predicted body
Ventilator rate setting needed to achieve a pH
Ratio of the duration of inspiration to the
*PaO denotes partial pressure of arterial oxygen, SpO oxyhemoglobin saturation measured by
pulse oximetry, FiO fraction of inspired oxygen, and PEEP positive end-expiratory pressure.
†Subsequent adjustments in tidal volume were made to maintain a plateau pressure of «50 cm of
water in the group receiving traditional tidal volumes and «30 cm of water in the group receivinglower tidal volumes.
‡Further increases in PEEP, to 34 cm of water, were allowed but were not required.
in four hours before the ventilator settings were changed on day 0.
ence in ventilator-free days could reflect a difference in mortality,
Physiologic and radiographic data, medication use, and use of oth-
ventilator days among survivors, or both. Other outcomes were
er investigational treatments were recorded between 6 and 10 a.m.
the number of days without organ or system failure and the oc-
on days 1, 2, 3, 4, 7, 14, 21, and 28. Data were transmitted weekly
currence of barotrauma, defined as any new pneumothorax, pneu-
to the network coordinating center. Patients were followed until
momediastinum, or subcutaneous emphysema, or a pneumatocele
day 180 or until they were breathing on their own at home.
that was more than 2 cm in diameter. Interim analyses were con-ducted by an independent data and safety monitoring board after
Assessment of Compliance
the enrollment of each successive group of approximately 200 pa-tients. Stopping boundaries (with a two-sided a level of 0.05) were
Randomly selected ventilator and blood gas variables were an-
designed to allow early termination of the study if the use of lower
alyzed for compatibility with the protocol. Quarterly reports of
tidal volumes was found to be either efficacious31 or ineffective.32
these data from each of the 10 centers were used by investigators
The comparison of traditional with lower tidal volumes was
one of two trials conducted simultaneously in the same patientsin a factorial experimental design. Ketoconazole was compared with
Statistical Analysis
placebo in the first 234 patients, and lisofylline was compared with
The first primary outcome was death before a patient was dis-
placebo in the last 194 patients; no drugs were assessed in the
charged home and was breathing without assistance. Patients who
were in other types of health care facilities at 180 days were con-
We used Student’s t-test or Fisher’s exact test to compare base-
sidered to have been discharged from the hospital and to be breath-
line variables. We used analysis of covariance to compare log-trans-
ing without assistance. The second primary outcome was ventila-
formed plasma interleukin-6 values. We used Wilcoxon’s test to
tor-free days, defined as the number of days from day 1 to day 28
compare the day 0 and day 3 plasma interleukin-6 concentrations,
on which a patient breathed without assistance, if the period of
ventilator-free days, and organ-failure–free days, which had skewed
unassisted breathing lasted at least 48 consecutive hours. A differ-
distributions. We used the 180-day cumulative incidence of mor-
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
tality to compare the proportion of patients in each group who
nificantly lower on days 1, 3, and 7 in the group
died before being discharged home and breathing without assist-
treated with lower tidal volumes than in the group
ance,33 after stratification for other experimental interventions:
treated with traditional tidal volumes (Table 3). The
treatment with ketoconazole, the ketoconazole placebo, lisofylline,the lisofylline placebo, or no other agent. We used a chi-square
mean (±SD) tidal volumes on days 1 to 3 were 6.2±
test to determine whether there was an interaction between the
0.8 and 11.8±0.8 ml per kilogram of predicted body
study group and the other experimental interventions with re-
weight (P<0.001), respectively, and the mean pla-
spect to the mean (±SE) mortality rates at 180 days. All P values
teau pressures were 25±6 and 33±8 cm of water
(P<0.001), respectively. The partial pressure of ar-
terial oxygen was similar in the two groups at all three
The trial was stopped after the fourth interim analy-
times, but the positive end-expiratory pressure and
sis because the use of lower tidal volumes was found
fraction of inspired oxygen were significantly higher
to be efficacious (P=0.005 for the difference in mor-
and the ratio of partial pressure of arterial oxygen to
tality between groups; P value for the stopping bound-
fraction of inspired oxygen was significantly lower in
ary, 0.023). The base-line characteristics of the 861
the group treated with lower tidal volumes on days
patients who were enrolled were similar, except that
1 and 3. On day 7, positive end-expiratory pressure
minute ventilation was slightly but significantly high-
and the fraction of inspired oxygen were significantly
er (P=0.01) in the group treated with lower tidal
higher in the group treated with traditional tidal vol-
umes. The respiratory rate was significantly higher in
The tidal volumes and plateau pressures were sig-
the group treated with lower tidal volumes on days1 and 3, but minute ventilation was similar in the twogroups on these days. The partial pressure of arterialcarbon dioxide was significantly higher on days 1, 3,and 7 and arterial pH was significantly lower on days1 and 3 in the group treated with lower tidal volumes. TABLE 2. BASE-LINE CHARACTERISTICS OF THE PATIENTS.*
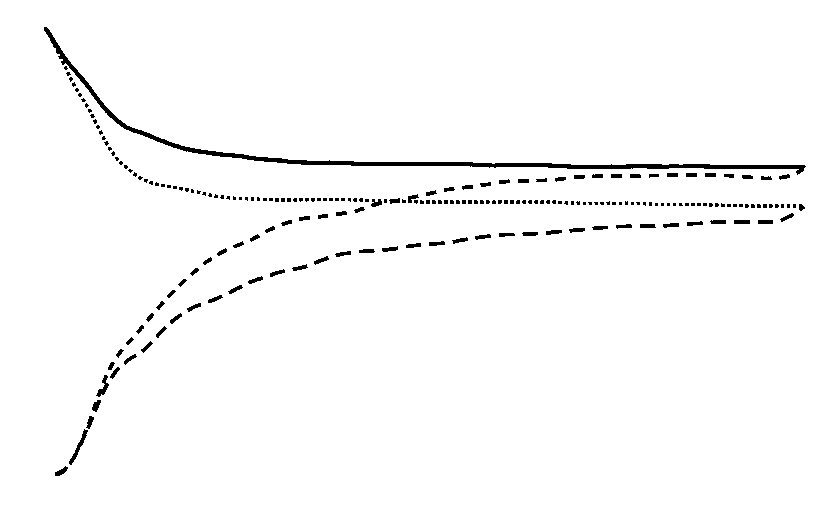
The probability of survival and of being discharged
home and breathing without assistance during the
GROUP RECEIVING GROUP RECEIVING
first 180 days after randomization is shown in Figure
TRADITIONAL TIDAL VOLUMES TIDAL VOLUMES
1. The mortality rate was 39.8 percent in the group
CHARACTERISTIC
treated with traditional tidal volumes and 31.0 per-cent in the group treated with lower tidal volumes
(P=0.007; 95 percent confidence interval for the
difference between groups, 2.4 to 15.3 percent). The
interaction between the study group and stratifica-
tion for other experimental interventions was not sig-
Data were available to calculate the static compli-
ance of the respiratory system at base line in 517 pa-
tients (Fig. 2). The interaction between the quartile
of static compliance at base line and the study group
with respect to the risk of death was not significant
The number of ventilator-free days was significantly
higher in the group treated with lower tidal volumes
than in the group treated with traditional tidal vol-
umes (Table 4). The median duration of ventilation
was 8 days among patients in both groups who were
discharged from the hospital after weaning and 10.5
*Plus–minus values are means ±SD. Because of rounding, not all per-
and 10 days, respectively, among those who died in
centages total 100. PaO denotes partial pressure of arterial oxygen, and
the group treated with lower tidal volumes and the
group treated with traditional tidal volumes. The num-
†APACHE III denotes Acute Physiology, Age, and Chronic Health Eval-
uation. Scores can range from 0 to 299, with higher scores indicating more
ber of days without nonpulmonary organ or system
failure was significantly higher in the group treated
‡Data were missing for one patient.
with lower tidal volumes (P=0.006). This group had
§Data were available for 300 patients in the group treated with lower tid-
more days without circulatory failure (mean [±SD],
al volumes and for 290 patients in the group treated with traditional tidal
19±10 vs. 17±11 days; P=0.004), coagulation fail-
ure (21±10 vs. 19±11 days, P=0.004), and renal
failure (20±11 vs. 18±11 days, P=0.005) than did
¿Organ and system failures were defined as described in the Methods
the group treated with traditional tidal volumes. The
V E N T I L AT I O N W I T H L OW E R T I DA L VO LU M E S I N PAT I E N T S W I T H T H E AC U T E R E S P I R ATO RY D I ST R E S S SY N D R O M E TABLE 3. RESPIRATORY VALUES DURING THE FIRST SEVEN DAYS OF TREATMENT IN PATIENTS WITH ACUTE LUNG INJURY
AND THE ACUTE RESPIRATORY DISTRESS SYNDROME.*
VARIABLE
*Plus–minus values are means (±SD) of the values recorded between 6 and 10 a.m. on days 1, 3, and 7 after enrollment. The numbers of
patients refers to those who were receiving ventilation and for whom data were available. FiO denotes fraction of inspired oxygen, PEEP
positive end-expiratory pressure, PaO partial pressure of arterial oxygen, and PaCO partial pressure of arterial carbon dioxide. All differences
between study groups were significant on each day (P<0.05) except for mean airway pressure on days 1, 3, and 7; the PaO :FiO on day 7;
minute ventilation on days 1 and 3; pH on day 7; and PaO on days 1, 3, and 7.
incidence of barotrauma after randomization was sim-
patients in the group treated with traditional tidal
volumes. These included prone positioning in 14 and
There were no significant differences between
groups in the percentages of days on which neuro-
The mean log-transformed plasma interleukin-6
muscular-blocking drugs were used among patients
values decreased from 2.5±0.7 pg per milliliter on
who were discharged home and breathing without
day 0 to 2.3±0.7 pg per milliliter on day 3 in the
assistance (6±14 percent in the group treated with
group treated with traditional tidal volumes and from
lower tidal volumes and 6±15 percent in the group
2.5±0.7 pg per milliliter to 2.0±0.5 pg per milliliter
treated with traditional tidal volumes) or among those
in the group treated with lower tidal volumes. The
who died (20±32 percent and 16±28 percent, respec-
decrease was greater in the group treated with lower
tively), or in the percentages of days on which seda-
tidal volumes (P<0.001), and the day 3 plasma in-
tives were used among patients who were discharged
terleukin-6 concentrations were also lower in this
home and breathing without assistance (65±26 per-
cent and 65±24 percent, respectively) or those whodied (73±24 percent and 71±28 percent, respec-
DISCUSSION
tively). Investigational treatments for acute lung in-
In this large study of patients with acute lung in-
jury and the acute respiratory distress syndrome that
jury and the acute respiratory distress syndrome, mor-
were not included in the factorial design of the ex-
tality was reduced by 22 percent and the number of
perimental interventions were given to 15 patients
ventilator-free days was greater in the group treated
in the group treated with lower tidal volumes and 12
with lower tidal volumes than in the group treated
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
TABLE 4. MAIN OUTCOME VARIABLES.* RECEIVING RECEIVING LOWER TIDAL TRADITIONAL VARIABLE TIDAL VOLUMES Figure 1. Probability of Survival and of Being Discharged Home
and Breathing without Assistance during the First 180 Days af-
of nonpulmonary organs or systems, days 1 to 28
ter Randomization in Patients with Acute Lung Injury and theAcute Respiratory Distress Syndrome.
*Plus–minus values are means ±SD. The number of ventilator-free days
The status at 180 days or at the end of the study was known for
is the mean number of days from day 1 to day 28 on which the patient had
all but nine patients. Data on these 9 patients and on 22 addi-
been breathing without assistance for at least 48 consecutive hours. Baro-
tional patients who were hospitalized at the time of the fourth
trauma was defined as any new pneumothorax, pneumomediastinum, or
subcutaneous emphysema, or a pneumatocele that was more than 2 cm indiameter. Organ and system failures were defined as described in the Meth-ods section.
on days 1 and 3. These results, coupled with the great-
er reductions in plasma interleukin-6 concentrations,
suggest that the group treated with lower tidal vol-umes had less lung inflammation.35 The greater re-
ductions in plasma interleukin-6 concentrations mayalso reflect a reduced systemic inflammatory response
to lung injury, which could contribute to the higher
number of days without organ or system failure and
the lower mortality in the group treated with lower
Several factors could explain the difference in re-
sults between our trial and other trials of ventilation
using lower tidal volumes in patients with acute lung
injury and the acute respiratory distress syndrome.22-24
(ml/cm of water/kg of predicted body weight)
First, our study had a greater difference in tidal vol-umes between groups. In one earlier trial, the tradi-
Figure 2. Mean (+SE) Mortality Rate among 257 Patients with Acute Lung Injury and the Acute Respiratory Distress Syndrome
tional tidal volume was equivalent to approximately
Who Were Assigned to Receive Traditional Tidal Volumes and
12.2 ml per kilogram of predicted body weight and
260 Such Patients Who Were Assigned to Receive Lower Tidal
the lower tidal volume was equivalent to approximate-
Volumes, According to the Quartile of Static Compliance of the
ly 8.1 ml per kilogram of predicted body weight.23
Respiratory System before Randomization.
In a second study, the traditional and lower tidal vol-
The interaction between the study group and the quartile ofstatic compliance at base line was not significant (P=0.49).
umes were approximately 10.3 and 7.1 ml per kilo-gram of dry body weight (calculated as the measuredweight minus the estimated weight gain from fluidretention), respectively.22 In the present trial, meas-ured weight exceeded predicted body weight by ap-
with traditional tidal volumes. These results are con-
proximately 20 percent. Assuming a similar difference,
sistent with the results of experiments in animals9-14
and assuming that half the difference was dry weight
and observational studies in humans.16,17
in excess of predicted body weight, tidal volumes in
These benefits occurred despite the higher require-
the second trial would have been approximately 11.3
ments for positive end-expiratory pressure and frac-
and 7.8 ml per kilogram of predicted body weight.
tion of inspired oxygen and the lower ratio of partial
Therefore, the traditional tidal volume of 11.8 ml
pressure of arterial oxygen to fraction of inspired ox-
per kilogram of predicted body weight in our study
ygen in the group treated with lower tidal volumes
was similar to the values in the previous two trials. V E N T I L AT I O N W I T H L OW E R T I DA L VO LU M E S I N PAT I E N T S W I T H T H E AC U T E R E S P I R ATO RY D I ST R E S S SY N D R O M E
However, the tidal volume of 6.2 ml per kilogram of
utes to compliance of the respiratory system and is
predicted body weight in the group receiving lower
reduced in many patients with acute lung injury and
tidal volumes was lower than the values in the pre-
the acute respiratory distress syndrome,39 may have
obscured a true interaction between tidal volume and
If one assumes that measured weights also exceed-
ed predicted body weights by 20 percent in the ear-
Barotrauma occurred with similar frequency in
lier trials, the tidal volumes in the traditional groups
the two study groups, a finding consistent with the
were approximately 10.2 and 9.4 ml per kilogram of
results of other studies in which the incidence of baro-
measured weight, respectively, as compared with 9.9
trauma was independent of airway pressures.22-24,40,41
ml per kilogram of measured weight in our study.
The most common manifestation of barotrauma was
Therefore, the tidal volumes in the traditional groups
pneumothorax, which could have been the result of
in each of the three trials were consistent with tradi-
invasive procedures. Pneumothorax is not a sensitive
or specific marker of stretch-induced injury with the
A second possible explanation for the different re-
sults is that the previous trials were designed to detect
The similarity in the number of days of ventilator
larger differences in mortality between groups.22-24
use among the survivors in both groups suggests that
Hence, they lacked the statistical power to demon-
the higher number of ventilator-free days in the group
strate the moderate effects of lower tidal volumes that
treated with lower tidal volumes resulted from re-
duced mortality rather than from a reduced number
A third difference in the trials was in the treat-
of days of ventilation among the survivors. However,
ment of acidosis. Increases in the ventilator rate were
the comparison of the number of days of ventilator
required and bicarbonate infusions were allowed to
use among the survivors could be misleading.42 Some
correct mild-to-moderate acidosis in our study, which
patients who would have survived in the group treat-
resulted in smaller differences in the partial pressure
ed with traditional tidal volumes might have needed
of arterial carbon dioxide and pH between the study
the ventilator on fewer days had they been in the
groups than in the previous trials.22-24 The deleteri-
group treated with lower tidal volumes. This bene-
ous effects of acidosis in the previous studies may
ficial effect would have been obscured if prolonged
have counteracted a protective effect of the lower
ventilation was required before recovery among pa-
tients who otherwise would have died in the group
In addition to being caused by excessive stretch,
treated with traditional tidal volumes. For similar
lung injury may also result from repeated opening
reasons, it is also difficult to compare the number of
and closing of small airways or from excessive stress
days with organ or system failure among the survi-
at margins between aerated and atelectatic regions of
the lungs.37 These types of lung injury may be pre-
We found that treatment with a ventilation ap-
vented by the use of a higher positive end-expiratory
proach designed to protect the lungs from excessive
pressure.10,13,37,38 A slightly higher positive end-expir-
stretch resulted in improvements in several impor-
atory pressure was necessary in the group treated with
tant clinical outcomes in patients with acute lung in-
lower tidal volumes during the first few days to main-
jury and the acute respiratory distress syndrome. On
tain arterial oxygenation at a level similar to that in
the basis of these results, high priority should be
the group treated with traditional tidal volumes, but
given to preventing excessive lung stretch during ad-
positive end-expiratory pressure was not increased as
justments to mechanical ventilation, and this lower-
tidal-volume protocol should be used in patients with
In a recent trial in 53 patients with acute respira-
acute lung injury and the acute respiratory distress
tory distress syndrome, 28-day mortality was signif-
icantly lower with a ventilation strategy that useda higher positive end-expiratory pressure combined
Supported by contracts (NO1-HR 46054, 46055, 46056, 46057,
with limited peak inspiratory pressure than with a
46058, 46059, 46060, 46061, 46062, 46063, and 46064) with the Na-
strategy of traditional ventilation.21 These results sug-
tional Heart, Lung, and Blood Institute.
Presented in part at the International Conference of the American Lung
gest that both increased positive end-expiratory pres-
Association and the American Thoracic Society, San Diego, Calif., April
sure and reduced inspiratory stretch could have ben-
We are indebted to the intensive care unit nurses, respiratory ther-
Stretch-induced lung injury may not occur if lung
apists, and physicians, as well as our patients and their families, who
compliance is not greatly reduced. However, the ben-
efit of ventilation with a lower tidal volume was in-dependent of the static compliance of the respiratory
APPENDIX
system at base line, suggesting that the lower tidal vol-
In addition to the members of the Writing Committee, the members of
ume was advantageous regardless of lung compliance.
the National Heart, Lung, and Blood Institute ARDS Network were as fol- lows: Network Participants: Cleveland Clinic Foundation — H.P. Wiede-
Variations in chest-wall compliance, which contrib-
mann, A.C. Arroliga, C.J. Fisher, Jr., J.J. Komara, Jr., P. Perez-Trepichio;
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Denver Health Medical Center — P.E. Parsons, R. Wolkin; Denver Veterans
tilation with permissive hypercapnia: a prospective study. Crit Care Med
Affairs Medical Center — C. Welsh; Duke University Medical Center — W.J.
Fulkerson, Jr., N. MacIntyre, L. Mallatratt, M. Sebastian, R. McConnell,
17. Hickling KG, Henderson SJ, Jackson R. Low mortality associated with
C. Wilcox, J. Govert; Johns Hopkins University — D. Thompson; LDS Hos-
low volume pressure limited ventilation with permissive hypercapnia in se-
pital — T. Clemmer, R. Davis, J. Orme, Jr., L. Weaver, C. Grissom, M.
vere adult respiratory distress syndrome. Intensive Care Med 1990;16:372-
Eskelson; McKay–Dee Hospital — M. Young, V. Gooder, K. McBride, C.
Lawton, J. d’Hulst; MetroHealth Medical Center of Cleveland — J.R. Peer-
18. Slutsky AS. Mechanical ventilation: American College of Chest Physi-
less, C. Smith, J. Brownlee; Rose Medical Center — W. Pluss; San Francisco
cians’ Consensus Conference. Chest 1993;104:1833-59. [Erratum, Chest
General Hospital Medical Center — R. Kallet, J.M. Luce; Jefferson MedicalCollege — J. Gottlieb, M. Elmer, A. Girod, P. Park; University of California,19. Blanch L, Fernandez R , Valles J, Sole J, Roussos C, Artigas A. Effect San Francisco — B. Daniel, M. Gropper; University of Colorado Health Sci-
of two tidal volumes on oxygenation and respiratory system mechanics dur-
ences Center — E. Abraham, F. Piedalue, J. Glodowski, J. Lockrem, R.
ing the early stage of adult respiratory distress syndrome. J Crit Care 1994;
McIntyre, K. Reid, C. Stevens, D. Kalous; University of Maryland — H.J.
Silverman, C. Shanholtz, W. Corral; University of Michigan — G.B. Toews,
20. Hedley-Whyte J, Pontoppidan H, Morris MJ. The response of patients
D. Arnoldi, R.H. Bartlett, R. Dechert, C. Watts; University of Pennsylvania
with respiratory failure and cardiopulmonary disease to different levels of
— P.N. Lanken, H. Anderson III, B. Finkel, C.W. Hanson; University of
constant volume ventilation. J Clin Invest 1966;45:1543-54. Utah Hospital — R. Barton, M. Mone; University of Washington–Harbor-21. Amato MBP, Barbas CSV, Medeiros DM, et al. Effect of a protective- view Medical Center — L.D. Hudson, C. Lee, G. Carter, R.V. Maier, K.P.
ventilation strategy on mortality in the acute respiratory distress syndrome.
Steinberg; Vanderbilt University — G. Bernard, M. Stroud, B. Swindell, L.
Stone, L. Collins, S. Mogan; Clinical Coordinating Center:Massachusetts 22. Brochard L, Roudot-Thoraval F, Roupie E, et al. Tidal volume reduc- General Hospital and Harvard Medical School — M. Ancukiewicz, D. Hay-
tion for prevention of ventilator-induced lung injury in acute respiratory
den, F. Molay, N. Ringwood, G. Wenzlow, A.S. Kazeroonian; National
distress syndrome. Am J Respir Crit Care Med 1998;158:1831-8. Heart, Lung, and Blood Institute Staff: D.B. Gail, C.H. Bosken, P. 23. Stewart TE, Meade MO, Cook DJ, et al. Evaluation of a ventilation
Randall, M. Waclawiw; Data and Safety Monitoring Board: R.G.
strategy to prevent barotrauma in patients at high risk for acute respiratory
Spragg, J. Boyett, J. Kelley, K. Leeper, M. Gray Secundy, A. Slutsky; Pro-
distress syndrome. N Engl J Med 1998;338:355-61. tocol Review Committee:T.M. Hyers, S.S. Emerson, J.G.N. Garcia, J.J. 24. Brower RG, Shanholtz CB, Fessler HE, et al. Prospective, random-
Marini, S.K. Pingleton, M.D. Shasby, W.J. Sibbald.
ized, controlled clinical trial comparing traditional versus reduced tidal vol-ume ventilation in acute respiratory distress syndrome patients. Crit Care
REFERENCES
Med 1999;27:1492-8. 25. Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. 1. Bernard GR , Artigas A, Brigham KL, et al. The American-European
Transection of the oesophagus for bleeding oesophageal varices. Br J Surg
Consensus Conference on ARDS: definitions, mechanism, relevant out-
comes, and clinical trial coordination. Am J Respir Crit Care Med 1994;
26. Crapo RO, Morris AH, Gardner RM. Reference spirometric values us-
ing techniques and equipment that meet ATS recommendations. Am Rev
2. Sloane PJ, Gee MH, Gottlieb JE, et al. A multicenter registry of pa-
tients with acute respiratory distress syndrome: physiology and outcome.
27. Crapo RO, Morris AH, Clayton PD, Nixon CR. Lung volumes in
healthy nonsmoking adults. Bull Eur Physiopathol Respir 1982;18:419-25. 3. Doyle RL, Szaflarski N, Modin GW, Wiener-Kronish JP, Matthay MA. 28. Knoben JE, Anderson PO, eds. Handbook of clinical drug data. 7th
Identification of patients with acute lung injury: predictors of mortality.
ed. Hamilton, Ill.: Drug Intelligence, 1993.
Am J Respir Crit Care Med 1995;152:1818-24. 29. Bernard GR , Wheeler AP, Arons MM, et al. A trial of antioxidants 4. Zilberberg MD, Epstein SK. Acute lung injury in the medical ICU: co-
N-acetylcysteine and procysteine in ARDS. Chest 1997;112:164-72.
morbid conditions, age, etiology, and hospital outcome. Am J Respir Crit
30. Arons MM, Wheeler AP, Bernard GR , et al. Effects of ibuprofen on
the physiology and survival of hypothermic sepsis. Crit Care Med 1999;27:
5. Pittet JF, Mackersie RC, Martin TR , Matthay MA. Biological markers
of acute lung injury: prognostic and pathogenic significance. Am J Respir
31. O’Brien PC, Fleming TR. A multiple testing procedure for clinical tri- 6. Marini JJ. Evolving concepts in the ventilatory management of acute 32. DeMets DL, Ware JH. Group sequential methods for clinical trials
respiratory distress syndrome. Clin Chest Med 1996;17:555-75.
with a one-sided hypothesis. Biometrika 1980;67:651-60. 7. Gattinoni L, Presenti A, Torresin A, et al. Adult respiratory distress 33. Kalbfleisch JD, Prentice RL. The statistical analysis of failure time
syndrome profiles by computed tomography. J Thorac Imaging 1986;
34. Knaus WA, Wagner DP, Draper EA, et al. The APACHE III prognos- 8. Maunder RJ, Shuman WP, McHugh JW, Marglin SI, Butler J. Preser-
tic system: risk prediction of hospital mortality for critically ill hospitalized
vation of normal lung regions in the adult respiratory distress syndrome:
analysis by computed tomography. JAMA 1986;255:2463-5. 35. Ranieri VM, Suter PM, Tortorella C, et al. Effect of mechanical ven- 9. Tsuno K, Miura K, Takeya M, Kolobow T, Morioka T. Histopathologic
tilation on inflammatory mediators in patients with acute respiratory dis-
pulmonary changes from mechanical ventilation at high peak airway pres-
tress syndrome: a randomized controlled trial. JAMA 1999;282:54-61.
sures. Am Rev Respir Dis 1991;143:1115-20. 36. Carmichael LC, Dorinsky PM, Higgins SB, et al. Diagnosis and ther- 10. Tremblay L, Valenza F, Ribeiro SP, Li J, Slutsky AS. Injurious ventila-
apy of acute respiratory distress syndrome in adults: an international survey.
tory strategies increase cytokines and c-fos m-RNA expression in an isolat-
ed rat lung model. J Clin Invest 1997;99:944-52. 37. Muscedere JG, Mullen JB, Gan K, Slutsky AS. Tidal ventilation at low 11. Parker JC, Hernandez LA, Peevy KJ. Mechanisms of ventilator-induced
airway pressures can augment lung injury. Am J Respir Crit Care Med
lung injury. Crit Care Med 1993;21:131-43. 12. Dreyfuss D, Basset G, Soler P, Saumon G. Intermittent positive-pres- 38. Corbridge TC, Wood LD, Crawford GP, Chudoba MJ, Yanos J, Sznaj-
sure hyperventilation with high inflation pressures produces pulmonary mi-
der JI. Adverse effects of large tidal volume and low PEEP in canine acid
crovascular injury in rats. Am Rev Respir Dis 1985;132:880-4.
aspiration. Am Rev Respir Dis 1990;142:311-5. 13. Webb HH, Tierney DF. Experimental pulmonary edema due to inter- 39. Mergoni M, Martelli A, Volpi A, Primavera S, Zuccoli P, Rossi A. Im-
mittent positive pressure ventilation with high inflation pressures: protec-
pact of positive end-expiratory pressure on chest wall and lung pressure-
tion by positive end-expiratory pressure. Am Rev Respir Dis 1974;110:
volume curve in acute respiratory failure. Am J Respir Crit Care Med 1997;
14. Kolobow T, Moretti MP, Fumagalli R , et al. Severe impairment in lung 40. Schnapp LM, Chin DP, Szaflarski N, Matthay MA. Frequency and im-
function induced by high peak airway pressure during mechanical ventila-
portance of barotrauma in 100 patients with acute lung injury. Crit Care
tion: an experimental study. Am Rev Respir Dis 1987;135:312-5. 15. Slutsky AS, Tremblay LN. Multiple system organ failure: is mechanical 41. Weg JG, Anzueto A, Balk RA, et al. The relation of pneumothorax
ventilation a contributing factor? Am J Respir Crit Care Med 1998;157:
and other air leaks to mortality in the acute respiratory distress syndrome.
16. Hickling KG, Walsh J, Henderson S, Jackson R. Low mortality rate in 42. Heitjan DF. Causal inference in a clinical trial: a comparative example.
adult respiratory distress syndrome using low-volume, pressure-limited ven-
Schroder USA Fondo Común de Inversión Estados Contables correspondientes al período de nueve meses finalizado el 30 de septiembre de 2009 presentados en forma comparativa. Schroder USA Fondo Común de Inversión Estados Contables correspondientes al período de nueve meses finalizado el 30 de septiembre de 2009 presentados en forma comparativa. Indice Balance Genera
1. PRODUCT AND COMPANY IDENTIFICATION Formulator: Emergency Phone: For 24-Hour Emergency Assistance (Spill, Leak, Fire, or Exposure), Call CHEMTREC®: Inside the U.S.: (800) 424-9300 Outside the U.S.: (703) 527-3887 For Medical Emergency: Product: EPTAM® 20-G EPA Signal Word: EPA Registration No.: Active Ingredient: Chemical Name:
 The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
TABLE 4. MAIN OUTCOME VARIABLES.*
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
TABLE 4. MAIN OUTCOME VARIABLES.*