Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
Williams & Wilkins 1997. All Rights Reserved.
Ciprofloxacin in pediatrics: worldwide clinical
experience based on compassionate use-safety
[Proceedings of a Symposium: Ciprofloxacin Use in Pediatric
HAMPEL, BARBARA MD; HULLMANN, RAINER MS; SCHMIDT,
From Bayer AG, Wuppertal, Germany. Address for reprints: Dr. Barbara Hampel, Medical Department Germany,
D-51368 Leverkusen, Germany. Fax 49-214-3051469.
Background. Quinolone-induced cartilage toxicity has been observed in experimental juvenile
animal studies and is species- and dose-specific. Accordingly these findings have led to thecontraindication of fluoroquinolones in children. Previous data in 634 adolescents and childrentreated with compassionate use ciprofloxacin demonstrated low rates of reversible arthralgia and asafety profile similar to that for adult patients.
Objective. This report describes the safety findings in 1795 children who received 2030
treatment courses of intravenous or oral ciprofloxacin.
Results. The average doses of intravenous and oral ciprofloxacin in the study population were 8
and 25 mg/kg/day, respectively. Treatment-associated events were reported in 10.9% of childrenreceiving oral ciprofloxacin compared with 18.9% among intravenous recipients. Overall arthralgiaoccurred during 31 ciprofloxacin treatment courses (1.5%) and the majority of events were of mildto moderate severity and resolved without intervention. More than 60% of arthralgia episodeswere in children with cystic fibrosis.
Conclusion. The adverse event pattern in children receiving ciprofloxacin in this analysis was
similar to that observed in adults. Rates of reversible arthralgia were low and unchanged frompreviously published surveillance data in children.
Quinolone cartilage toxicity was initially observed in experimental investigations in juvenile
animals. The first histopathologic findings of articular cartilage damage in immature dogs induced
by nalidixic, oxolinic and pipemidic acids were reported by Ingham et al.1 in 1977. Specifically the
cartilage showed characteristic lesions including blisters and erosions.2 Furthermore the role of
mechanical pressure, determined by the fact that clinical arthropathy and blister formations appear
only in weight-bearing joints, was confirmed by several investigators.3, 4
Since these first reports articular cartilage toxicity has been observed in juvenile animals with
all fluoroquinolones tested. In addition arthrotoxic manifestations were found to be species- and
Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
dosage-dependent. For example cartilage damage have been observed with ciprofloxacin, but at
larger dosages compared with nalidixic acid. The hips, knees and shoulder joints are mainly
affected which signifies that clinical arthropathy occurs only in weight-bearing joints. Although the
mechanism of arthrotoxicity is still unknown, this potential risk led to important restrictions in the
use of quinolones. However, the experimentally induced cartilage damage has not been confirmed
Nalidixic acid has been used in children for more than two decades, often for prolonged
periods. Follow-up studies have failed to detect any joint pathology.5 After the initiation of
ciprofloxacin clinical trials in the early 1980s, ciprofloxacin has been administered to children
despite restrictions. The first report from a child treated with ciprofloxacin was in May, 1983.6
Since that time ciprofloxacin has been continuously used in children and adolescents when
conventional therapy failed or was not available.
This report summarizes the safety data available from patients, in the international Bayer
clinical data pool, who received ciprofloxacin on a compassionate use basis.
Safety data were accrued from two sources involving pediatric patients. Ciprofloxacin tablets
and/or intravenous solution were provided to physicians on request for use in pediatric patients
who had failed conventional therapy or for whom no other therapeutic alternative was appropriate.
Secondly safety reports were obtained from physicians who chose to use ciprofloxacin in pediatric
The first part of these data (634 cases) has been published by Chysky et al.7 Continuing
collection of these compassionate use data has resulted in a total of 2030 treatment courses.
Documentation of these cases included case report forms used for Phase IV trials as well as case
report forms used for postapproval surveillance studies.
Physicians, who requested ciprofloxacin on compassionate use basis, were asked to carefully
document the safety of the drug with special emphasis on joint evaluation. They were also
requested to provide the following information: patients' demographic data; the general status of
health; infection diagnosis; causative organisms; accompanying diseases; concomitant medication;
ciprofloxacin dosage regimen and route of administration; duration of therapy; and laboratory
safety data including hematology, blood chemistry and urinalysis. Because these patients were not
part of a study, information is occasionally incomplete.
Demographic data. By December 31, 1994, a total of 2030 treatment courses with
ciprofloxacin in 1795 children and adolescents (up to 17 years) were completed. Of these 1767
received oral treatment, 159 iv treatment and 98 patients sequential iv/oral therapy. Eighty-two
patients received more than 1 treatment course. One patient received 14 treatment courses. There
was a slight female predominance (54%).
The majority of the children treated with ciprofloxacin were between 13 and 17 years old: 1447
Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
or 71.3%. There were 517 treated children (25.5%) between 5 and 12 years and 66 children were
The respiratory tract was considered the infection site in >65% of the children (1316 cases),
followed by skin and skin structure in 155 patients and urinary tract in 153 patients. All other
infection sites were of minor importance. In cases with a specific diagnosis, cystic fibrosis followed
by pneumonia and bronchitis were the most frequently reported respiratory tract pathologies. The
severity of the infection clearly reflected the compassionate use of ciprofloxacin: 36.6% of the
infections were considered to be severe; 49.2% were considered moderate; and the infection was
A causative organism was documented in approximately one-third of the patients with
respiratory tract infection. The most frequently documented organism from these patients was 358
(54%) isolates of Pseudomonas aeruginosa. In addition 111 (17%) Pseudomonas sp. were
cultured. Clearly more than two-thirds of pathogens from the respiratory tract were Pseudomonas
sp. This pathogen distribution clearly reflects the predominance of cystic fibrosis patients. The next
most frequently isolated pathogen was Staphylococcus sp. which was documented in 93 (14%)
cases in the respiratory tract. All other organisms were infrequently documented.
The largest group of orally treated patients (n = 649, 36.7%) received 21 to 40 mg/kg body
weight per day; 150 patients received 41 to 50 mg/kg/day and 171 patients were treated with 15
to 20 mg/kg/day. The median oral daily dosage was 25 mg/kg. The duration of oral treatment
ranged from 1 to 303 days. Thirteen patients received oral ciprofloxacin from 151 to 300 days, but
most patients were treated for 15 to 30 days (n = 555, 32.9%). The most often administered iv
dosage in mg/kg body weight was 6 to 10 mg/kg/day. The latter iv dosage was also documented
for most of the patients receiving sequential iv/oral treatment. Duration of iv treatment ranged
from 1 to 72 days. Five patients received iv treatment for 31 to 72 days.
Safety. Adverse events (drug-related and non-drug-related), according to the Costart system,
were reported in 192 (10.9%) of 1767 patients treated with ciprofloxacin (Fig. 1). The total number
of individual adverse events was 270. After iv ciprofloxacin administration 47 adverse events
occurred in 30 of 159 patients (18.9%; Fig. 1). The digestive system was the site of most adverse
effects, including diarrhea, with nausea and vomiting. In addition headache and abdominal pain
were frequently reported. Hypersensitivity, injection site reactions, musculoskeletal system
adverse events, psychiatric disorders and thromboembolism were infrequently reported.
Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
Fig. 1. International clinical data pool. Incidence of adverse events during the use of ciprofloxacinin pediatric patients. Number of patients with adverse events: oral, 192 (10.9%); iv, 30 (18.9%).
Arthralgia. Arthralgia denotes the clinical entity of joint pain and may be associated with signs
of inflammation. Arthralgia occurred in 31 of 2030 patients (1.5%). Nineteen patients had
documented cystic fibrosis and 9 additional patients' underlying condition was cystic fibrosis.
The intensity of the arthralgia was documented in 29 cases and was considered mild in 9
patients, moderate in 16 patients and severe in 4 patients. The total daily dose of oral ciprofloxacin
in these patients was 200 to 1500 mg. The median duration of therapy was 23 days. Therapy was
permanently discontinued in 9 patients, discontinued temporarily in 5 cases and was not
discontinued in 14 patients. In one patient the dosage was reduced and another received remedial
Arthralgia was reported to resolve in 25 patients, including the severely affected patients, 1
patient improved and 1 remained unchanged. In the remaining 4 patients, information regarding
The data from the international clinical data pool reflect the spectrum of ciprofloxacin
compassionate use in children wherein it was administered most frequently to children with acute
pulmonary exacerbation caused by cystic fibrosis. Ciprofloxacin was found to be advantageous
when compared with conventional intravenous therapy because of its availability in an oral
formulation and its excellent activity against pseudomonal organisms. Of most importance this
report emphasized the safety of ciprofloxacin in pediatric patients and confirms the results reported
previously in 634 cases.7 Except for arthralgia the adverse event pattern in children was similar
compared to that observed in adults.8 The incidence of reversible arthralgia has remained
unchanged from a previous report with 1.3%7 and 1.5% from the current report.
Arthralgia occurred in 31 patients in this report, including 28 cases among cystic fibrosis
patients. Arthropathy has been estimated to occur in 4 to 7% of the cystic fibrosis population.9
Therefore definite diagnosis of quinolone-associated arthropathy in this patient population is often
Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
In a recent literature review of ciprofloxacin use in pediatric patients, there were 36 cases of
arthralgia among 1113 children (3.2%) from 12 studies.10 The great majority of patients with joint
symptoms were adolescents with cystic fibrosis, which concurs with the current report. In 3 of the
12 studies, where magnetic resonance imaging or plane radiographs were obtained, no cartilage
The compassionate data presented herein, as well as data from published trials, indicate that
acute courses of ciprofloxacin therapy appear to be safe in children. The incidence of arthropathy is
consistent among all available reports, and to date no cases of cartilage damage have been
reported. Continued surveillance of ciprofloxacin safety in children will be necessary to confirm
these findings, especially if ciprofloxacin is prescribed more widely in the pediatric population.
1. Ingham B, Brentnall DW, Dale EA, McFadzean JA. Arthropathy induced by antibacterial fusedN-alkyl-4-pyridone 3-carboxylic acids. Toxicol Lett 1977;1:21-6. Bibliographic Links [Context Link]
2. Gough A, Barsoum NY, Mitchell L, McGuire EJ, De La Iglesia FA. Juvenile canine drug-induced arthropathy:clinicopathological studies on articular lesions caused by oxolinic and pipemidic acids. Toxicol Appl Pharmacol1979;51:177-87. [Context Link]
3. Simon C. Im Tierexperiment beobachtete Knorpelsch, digung duch Chinolone. Fortschr AntimikrobAntineoplast Chemother 1984;3:785-8. [Context Link]
4. Stahlmann R, Merker HJ, Hinz N, Chahoud J, Heger W, Neubert D. Ofloxacin in juvenile non-humanprimates and rats: arthropathia and drug plasma concentrations. Arch Toxicol 1990;64:193-204.
5. Schaad UB, Wedgwood-Krucho J. Nalidixic acid in children: retrospective matched controlled study forcartilage toxicity. Infection 1987;15:165-8. Bibliographic Links [Context Link]
6. Data on file. Bayer AG, Wuppertal, Germany. [Context Link]
7. Chysky V, Kapila K, Hullmann R, Arcieri G, Schacht P, Echols R. Quinolones in clinical use: safety ofciprofloxacin in children: worldwide clinical experience based on compassionate use-emphasis on jointevaluation. Infection 1991;19:289-96. Bibliographic Links [Context Link]
8. Schacht P, Arcieri G, Branolte J, et al. Worldwide clinical data on efficacy and safety of ciprofloxacin. Infection 1988;16(Suppl. 1):29-43. [Context Link]
9. Phillips BM, David TJ. Pathogenesis and management of arthropathy in cystic fibrosis. J R Soc Med1986;79(Suppl. 12):44-50. [Context Link]
10. Kubin R. Safety and efficacy of ciprofloxacin in paediatric patients: review. Infection 1993;21:413-21.
Key words: Ciprofloxacin; pediatrics; safety; arthropathy; arthralgia
Proceedings of a symposium; July 28 to 29, 1995; Nantucket, MA
Accession Number: 00006454-199701000-00036
Copyright (c) 2000-2005 Ovid Technologies, Inc. Version: rel10.2.0, SourceID 1.11354.1.65
Access-produkter v9 släpps onsdag 12 Mars Version 9 (på svenska) av Supernova, Hal, Lunar och LunarPlus släpps den 12 mars 2008. Omskriven kod för Internet Explorers Document Object Model (DOM) Våra utvecklare har skrivit om koden för Internet Explorers DOM från grunden. Detta innebär bland annat mer konsekvent och tillförlitlig navigering när du läser Internetsidor med hjä
Dr. Petheő Gábor OTKA pályázatokhoz csatolandó közleményjegyzéke, Created on 2/24/2011 12:00 PM Eredeti közlemények (cikkek): 1 : Petheő GL , Orient A, Baráth M, Kovács I, Réthi B, Lányi A, Rajki A, Rajnavölgyi E, Geiszt M. Molecular and functional characterization of Hv1 proton channel in human granulocytes. PLoS One. 2010 Nov 23;5(11):e14081. IF: 4.351 (2010-ben), Cit
 Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
Williams & Wilkins 1997. All Rights Reserved.
Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
Williams & Wilkins 1997. All Rights Reserved.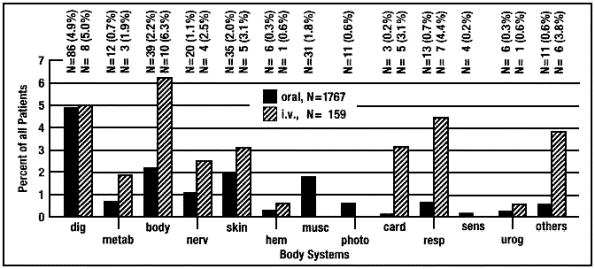 Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
Fig. 1. International clinical data pool. Incidence of adverse events during the use of ciprofloxacinin pediatric patients. Number of patients with adverse events: oral, 192 (10.9%); iv, 30 (18.9%).
Ovid: HAMPEL: Pediatr Infect Dis J, Volume 16(1).January 1997.127-129
http://gateway.ut.ovid.com/gw1/ovidweb.cgi
Fig. 1. International clinical data pool. Incidence of adverse events during the use of ciprofloxacinin pediatric patients. Number of patients with adverse events: oral, 192 (10.9%); iv, 30 (18.9%).