Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek the advice of your own physician or other qualified health care professional regarding any medical questions or conditions. The use of this website is governed by the UpToDate Terms of Use 2014 UpToDate, Inc.
Patient information: Endometriosis (Beyond the Basics) Section Editor Deputy Editor Disclosures
All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Dec 2013. | This topic last updated: May 7, 2013. INTRODUCTION — Endometriosis is a condition where tissue, similar to the tissue that normally grows inside the uterus, also grows outside of the uterus. The tissue inside the uterus is called "endometrium" and the tissue outside of the uterus is called "endometriosis". The most common places where endometriosis occurs are the ovaries, the fallopian tubes, the bowel, and the areas in front, in back, and to the sides of the uterus.
Some women with endometriosis have few or no symptoms while others have pain or difficulty becoming pregnant. There is no cure for endometriosis, but there are several treatment options. The best treatment depends on your individual situation.
More detailed information about endometriosis is available by subscription. (See "Overview of the treatment of endometriosis".)
ENDOMETRIOSIS CAUSES — The cause of endometriosis is not known. A common theory is that some menstrual blood and endometrium flows backwards from the uterus through the fal opian tubes and into the pelvis during a menstrual period (figure 1). This tissue then grows where it lands in the pelvis. This is called the retrograde menstruation theory. There are several other theories. ENDOMETRIOSIS SYMPTOMS — Some women with endometriosis have no symptoms. The most common symptom is pain in the pelvic area, especial y with periods. Pain — Pelvic pain caused by endometriosis can occur:
■ Just before or during the menstrual period. In some women, painful periods get worse over time.
(See "Patient information: Painful menstrual periods (dysmenorrhea) (Beyond the Basics)".)
■ Between menstrual periods, with worsened pain during the period
■ With bowel movements or while urinating, especially during the period
Pelvic pain can also be caused by many other conditions, such as pelvic infections and irritable bowel syndrome. A doctor or nurse can help to figure out if endometriosis may be the cause of your pain.
http://www.uptodate.com/contents/endometriosis-beyond-the-basics?topicKey=PI%2F217. Difficulty getting pregnant — Endometriosis can make it more difficult to become pregnant. This might occur because endometriosis may cause scar tissue to develop, which can damage the ovaries or fallopian tubes. Even women with endometriosis who do not have scar tissue can have difficulty becoming pregnant.
In women who become pregnant, endometriosis does not harm the pregnancy. Symptoms of endometriosis often improve after pregnancy. Endometriomas (chocolate cysts) — Women with endometriosis can develop ovarian cysts containing endometriosis; this is called an endometrioma. Endometriomas are usually fil ed with old blood that resembles chocolate syrup; thus, they are sometimes called chocolate cysts. Endometriomas are sometimes seen during a pelvic ultrasound or felt during a pelvic exam. ENDOMETRIOSIS DIAGNOSIS — Your doctor or nurse might suspect that you have endometriosis based on your symptoms of pelvic pain or painful menstrual periods. However, the only way to know for sure if you have endometriosis is to have surgery.
Endometriosis is considered mild, moderate, or severe depending on what is found during surgery. Women with mild disease can have severe symptoms, and women with severe disease can have mild symptoms.
In some cases, your doctor wil recommend a medicine as the first treatment for symptoms that make her suspect endometriosis. This might include a nonsteroidal antiinflammatory medicine (ibuprofen/Advil) or hormonal birth control. (See 'Endometriosis treatment' below.)
If treatment does not improve your pain within three to six months, surgery is a reasonable next step. (See 'Surgery' below.)
In other cases, surgery is performed to diagnose endometriosis and remove it before you take any medicine. Talk to your doctor or nurse about which treatment is right for your situation. ENDOMETRIOSIS TREATMENT — There are several treatment options for women with endometriosis:
■ Nonsteroidal antiinflammatory drugs■ Hormonal birth control■ Other forms of hormone treatment (gonadotropin releasing hormone agonists)■ Surgery
The best treatment depends on your future plans to become pregnant and what symptoms are most bothersome. Nonsteroidal antiinflammatory drugs — Nonsteroidal antiinflammatory drugs (NSAIDs) are a type of pain medicine that can help to relieve the pain caused by endometriosis. The medicine works by stopping the release of prostaglandins, one of the main chemicals responsible for painful menstrual periods. NSAIDs do not shrink or prevent the growth of endometriosis.
Most NSAIDs are available without a prescription, including:
■ Ibuprofen (sold as Advil, Motrin, and store brands). Follow the package instructions. In general, two
tablets are taken for the first dose and one tablet every four to six hours, as needed, thereafter. These should be taken with food and may be most effective if started one to two days before the onset of pain. Physicians may prescribe higher doses.
http://www.uptodate.com/contents/endometriosis-beyond-the-basics?topicKey=PI%2F217.
■ Naproxen sodium (sold as Aleve, Anaprox, Naprosyn, and store brands). Follow the package
instructions, as the dose and frequency differ depending on the formulation. In general, two tablets are taken for the first dose, and one tablet is taken every 8 to 12 hours, as needed, thereafter, depending on the formulation. All tablets should be taken with food and a full glass of water. Like ibuprofen, naproxen may be more effective if begun a day or two prior to the onset of typical menstrual pain. Physicians may prescribe higher doses.
■ The disadvantage of NSAIDs is that they do not always relieve endometriosis-related pain. NSAIDs
probably work better when combined with another treatment, like hormonal birth control. Serious side effects from NSAIDs, although uncommon, include stomach upset, kidney problems, and worsened high blood pressure. Hormonal birth control treatments — Hormonal birth control, including the pill, patch, and the vaginal ring are often helpful in treating pain because they reduce heavy bleeding. Injectable and implantable long -acting progestins may be very effective in managing endometriosis-related pain. A progestin-containing intrauterine device can also be very effective in treating pain. Hormonal birth control works best in women who do not have severe pain unrelated to the period.
Women with endometriosis are often advised to take hormonal birth control continuously (skipping the placebo pills) for three or more months. This allows you to have fewer periods and have less pain and bleeding during each period. This is explained in detail separately. (See "Patient information: Hormonal methods of birth control (Beyond the Basics)", section on 'Continuous dosing'.)
The most common side effects of estrogen-containing hormonal birth control are:
■ Nausea■ Breast tenderness■ Irregular vaginal bleeding or spotting
These side effects usually improve after using the treatment for several months. Serious side effects (eg, blood clots, stroke, heart attack) are rare in women who do not smoke. (See "Patient information: Hormonal methods of birth control (Beyond the Basics)".)
Progestins — Progestins are a synthetic form of a natural hormone called progesterone. This treatment might be recommended for women who do not get pain relief from or who cannot take hormonal birth control that contains estrogen (such as smokers). Progestins are available by prescription and usually given as a pil or injection. Progestins are not used if you are trying to become pregnant. A progestin- containing intrauterine device delivers very low levels of progestin directly to the uterus and results in markedly lighter and less painful bleeding episodes with fewer systemic side effects.
Side effects of progestins can be bothersome for some women. The most common side effects include: bloating, weight gain, irregular vaginal bleeding, and rarely, worsened depression. Gonadotropin releasing hormone agonists — Gonadotropin releasing hormone (GnRH) agonists are medicines that work by causing a temporary menopause. The treatment causes the ovaries to stop producing estrogen, which causes the endometriosis implants to shrink.
This treatment reduces pain in over 80 percent of women, including women with severe pain. GnRH agonists are not used if you are trying to become pregnant.
■ Nafarelin (Synarel) - Nasal spray taken twice per day
http://www.uptodate.com/contents/endometriosis-beyond-the-basics?topicKey=PI%2F217.
■ Leuprolide (Lupron) - Shot taken once every one or three months■ Goserelin (Zoladex) - Shot taken once every 28 days
Adult women can take the full dose of a GnRH agonist for up to 12 months. There are concerns about using GnRH agonists at full strength for more than 12 months. Women who use GnRH agonists lose bone density, and this can become serious over time. One way to minimize bone loss is to take hormonal "add-back" treatment (adding very small amounts of either estrogen or a synthetic progestin) in addition to the GnRH agonist.
Taking hormonal add-back can also help to treat the most common side effects of GnRH agonists, which are menopausal symptoms (hot flashes, vaginal dryness, decreased libido, insomnia). (See "Gonadotropin releasing hormone agonists for long-term treatment of endometriosis".)
Surgery — Surgery might be an option to treat endometriosis if you:
■ Have tried medicines but still have bothersome pain (attributable to endometriosis)
■ Have a growth or mass in the pelvic area. Surgery may be necessary to remove the mass and
figure out if endometriosis, or another problem, is the cause.
■ Are having trouble getting pregnant and endometriosis might be the cause.
The goal of surgery is to remove endometriosis implants and scar tissue. More than 80 percent of women who have surgery have less pain for several months after surgery. However, there is a good chance that the pain wil come back unless you take some form of treatment after surgery (like hormonal birth control). Laparoscopy — Laparoscopy is one way to perform surgery, and is commonly used to diagnose and
treat endometriosis. During laparoscopy, a doctor makes several small cuts to place instruments inside the abdomen and pelvis. One of these instruments has a light and camera, which allows the doctor to see the organs on a screen. Treatment of an endometrioma — Medicines are unlikely to make an endometrioma go away.
Surgery to remove the endometrioma if it is larger than 4 to 5 cm, symptomatic or enlarging, is usually recommended because surgery can confirm the diagnosis, prevent complications (such as rupture of the endometrioma), and treat any symptoms, such as pain. (See "Diagnosis and management of ovarian endometriomas".)
Removal of the uterus or ovaries — Your doctor might recommend surgery to remove your uterus or
■ You have tried other treatments but continue to have severe symptoms
■ You do not want to become pregnant in the future
■ Surgery to remove the uterus is called hysterectomy. (See "Patient information: Abdominal
■ Surgery to remove the ovaries and fal opian tubes is called salpingo-oophorectomy. It is not always
necessary to remove the ovaries to treat endometriosis; this decision will depend on your age and your preferences.
http://www.uptodate.com/contents/endometriosis-beyond-the-basics?topicKey=PI%2F217. Hormone therapy after surgery — If your ovaries are removed, your doctor or nurse might
recommend hormone therapy (estrogen) after surgery. This is especially true for women under age 50 who are not yet menopausal. Estrogen can help to minimize menopausal symptoms like hot flashes, night sweats, vaginal dryness, and bone loss. (See "Patient information: Postmenopausal hormone therapy (Beyond the Basics)".)
INFERTILITY TREATMENT — There are several options for treating infertility in women with endometriosis. The best treatment depends on individual factors, including your age, if there are other fertility issues, and how severe your endometriosis is. Treatment options include:
■ A fertility medicine (such as clomiphene/Clomid). (See "Patient information: Ovulation induction
with clomiphene (Beyond the Basics)".)
■ Fertility medicines with intrauterine insemination. (See "Patient information: Infertility treatment with
■ Surgery to remove endometriosis (see 'Surgery' above)
■ In vitro fertilization (IVF). (See "Patient information: In vitro fertilization (IVF) (Beyond the Basics)".)
More detailed information about endometriosis and infertility is available. (See "Pathogenesis and treatment of infertility in women with endometriosis".)
WHERE TO GET MORE INFORMATION — Your healthcare provider is the best source of information for questions and concerns related to your medical problem.
This article will be updated as needed on our web site (www.uptodate.com/patients). Related topics for patients, as well as selected articles written for healthcare professionals, are also available. Some of the most relevant are listed below. Patient level information — UpToDate offers two types of patient education materials. The Basics — The Basics patient education pieces answer the four or five key questions a patient
might have about a given condition. These articles are best for patients who want a general overview and who prefer short, easy-to-read materials.
Patient information: Endometriosis (The Basics) Patient information: Painful periods (The Basics) Patient information: Infertility in women (The Basics) Patient information: Ovarian cysts (The Basics) Patient information: Uterine adenomyosis (The Basics)
Beyond the Basics — Beyond the Basics patient education pieces are longer, more sophisticated,
and more detailed. These articles are best for patients who want in-depth information and are comfortable with some medical jargon.
Patient information: Painful menstrual periods (dysmenorrhea) (Beyond the Basics) Patient information: Hormonal methods of birth control (Beyond the Basics) Patient information: Abdominal hysterectomy (Beyond the Basics) Patient information: Postmenopausal hormone therapy (Beyond the Basics) Patient information: Ovulation induction with clomiphene (Beyond the Basics) Patient information: Infertility treatment with gonadotropins (Beyond the Basics) Patient information: In vitro fertilization (IVF) (Beyond the Basics)
http://www.uptodate.com/contents/endometriosis-beyond-the-basics?topicKey=PI%2F217. Professional level information — Professional level articles are designed to keep doctors and other health professionals up-to-date on the latest medical findings. These articles are thorough, long, and complex, and they contain multiple references to the research on which they are based. Professional level articles are best for people who are comfortable with a lot of medical terminology and who want to read the same materials their doctors are reading.
Diagnosis and management of ovarian endometriomas Diagnosis and treatment of endometriosis in adolescents Gonadotropin releasing hormone agonists for long-term treatment of endometriosis Reproductive surgery for female infertility Overview of the treatment of endometriosis Pathogenesis and treatment of infertility in women with endometriosis Pathogenesis, clinical features, and diagnosis of endometriosis Thoracic endometriosis The following organizations also provide reliable health information.
(www.nlm.nih.gov/medlineplus/endometriosis.html)
■ The American Congress of Obstetricians and Gynecologists
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Hughes E, Fedorkow D, Collins J, Vandekerckhove P. Ovulation suppression for endometriosis.
Cochrane Database Syst Rev 2000; :CD000155.
2. ACOG Committee on Practice Bulletins--Gynecology. ACOG practice bulletin. Medical management
of endometriosis. Number 11, December 1999 (replaces Technical Bulletin Number 184, September 1993). Clinical management guidelines for obstetrician-gynecologists. Int J Gynaecol Obstet 2000; 71:183.
3. Kennedy S, Bergqvist A, Chapron C, et al. ESHRE guideline for the diagnosis and treatment of
endometriosis. Hum Reprod 2005; 20:2698.
4. Allen C, Hopewell S, Prentice A, Gregory D. Nonsteroidal anti-inflammatory drugs for pain in women
with endometriosis. Cochrane Database Syst Rev 2009; :CD004753.
5. Davis L, Kennedy SS, Moore J, Prentice A. Modern combined oral contraceptives for pain
associated with endometriosis. Cochrane Database Syst Rev 2007; :CD001019.
http://www.uptodate.com/contents/endometriosis-beyond-the-basics?topicKey=PI%2F217. GRAPHICS Areas where endometriosis can be found
This figure shows some of the areas in the body (purple spots) where endometriosis can be found. Common areas affected by endometriosis include the ovaries, the tubes connecting the ovaries to the uterus (fallopian tubes), and the bowel. Endometriosis can also grow in front, in back, and to the sides of the uterus. Sometimes the doctor can feel the tissue when doing a pelvic exam.
http://www.uptodate.com/contents/endometriosis-beyond-the-basics?topicKey=PI%2F217.
PROHIBITED LIST INTERNATIONAL STANDARD The official text of the Prohibited List shall be maintained by WADA and shall be published in English and French. In the event of any conflict between the English and French versions, the English version shall prevail. This List shall come into effect on 1 January 2012 THE 2012 PROHIBITED LIST WORLD ANTI-DOPING CODE Valid 1 Janua
SAFETY INFORMATION - LITHIUM-IONS BATTERY PACK Batterypack 1. Product- and Company Name Tradename Manufactrurer/Distributor 2. Compsition/Information on ingredients Characterisation Registered Office: Stuttgart, Registration Court: Amtsgericht Stuttgart HRB 14000 Chairman of the Supervisory Board: Hermann Scholl; Managing Directors: Franz Fehrenbach, Siegfried Dai


 The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek the advice of your own physician or other qualified health care professional regarding any medical questions or conditions. The use of this website is governed by the UpToDate Terms of Use 2014 UpToDate, Inc.
Patient information: Endometriosis (Beyond the Basics)
The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek the advice of your own physician or other qualified health care professional regarding any medical questions or conditions. The use of this website is governed by the UpToDate Terms of Use 2014 UpToDate, Inc.
Patient information: Endometriosis (Beyond the Basics)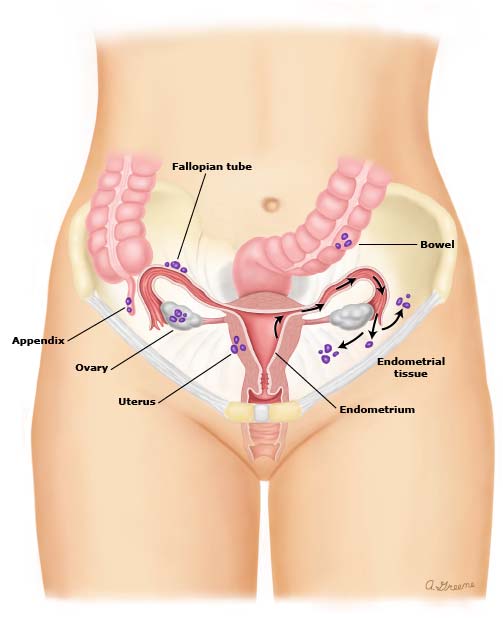 GRAPHICS
GRAPHICS