Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Plasma amitriptyline level after acute administration, and driving performance in healthy volunteers
Psychiatry and Clinical Neurosciences 2008; 62: 610–616 Regular Article
Plasma amitriptyline level after acute administration, anddriving performance in healthy volunteers
Kunihiro Iwamoto, MD,1 Yukiko Kawamura, MS,2 Masahiro Takahashi, MD,1Yuji Uchiyama, PhD,3 Kazutoshi Ebe, ME,3 Keizo Yoshida, MD, PhD,1*Tetsuya Iidaka, MD, PhD,1 Yukihiro Noda, PhD2 and Norio Ozaki, MD, PhD11Department of Psychiatry, Nagoya University, Graduate School of Medicine, 2Meijyo University, Graduate School ofPharmacy, Division of Clinical Science and Neuropsychopharmacology and 3Toyota Central R&D Labs., Aichi, JapanAims: Amitriptyline triggers the impairment of cog-
plasma amitriptyline concentrations were measured
nitive and motor functions and has been confirmed
on high-performance liquid chromatography.
to have harmful effects on driving performance. Results: A significant positive correlation was ob-
Although interindividual differences in plasma
served between the plasma amitriptyline concen-
concentration may cause variations in driving
tration and road-tracking performance (r = 0.543,
P < 0.05). There was no significant correlation
amitriptyline concentration and its effect on driving
between the plasma amitriptyline concentration and
performance has not been completely elucidated.
other driving performance, cognitive functions, and
Thus, the aim of the present study was to assess
the influence of individual pharmacokinetic dif-ferences on driving performance and cognitive
Conclusions: Amitriptyline produces a concentration-
related impairment on road-tracking performance. Therapeutic monitoring of amitriptyline would be
Methods: In this double-blinded study, 17 healthy
useful for predicting the difficulties involved while
male volunteers were given an acute, single, 25-mg
dose of amitriptyline. The subjects were assignedthree driving simulator tasks, three cognitive tasks,
Key words: amitriptyline, antidepressants, automo-
and the questionnaire of the Stanford Sleepiness
bile driving, cognition, drug monitoring.
Scale at the baseline and at 4 h after dosing. The
INTERINDIVIDUAL DIFFERENCES IN drug re- case of antidepressants, tricyclic antidepressants
sponses occur even when the same dosage of a drug
(TCA) are repeatedly recommended to be monitored
is prescribed to different individuals. Therapeutic
for blood concentration1–5 because these drugs have
drug monitoring (TDM) is one of the most valid tools
shown a fairly large interindividual variance in clini-
utilized to minimize interindividual differences in
cal response. The relationship between the blood
drug responses. TDM enables a clinician to adjust the
TCA concentration and adverse effects, such as
drug dosage and enhance efficacy and safety.1 In the
dropout rate, central nervous system toxicity, and car-diovascular toxicity has been reported.4,6
Among TCA, there is no consensus regarding the
*Correspondence: Keizo Yoshida, MD, PhD, Department of
relationship between plasma amitriptyline concen-
Psychiatry, Nagoya University, Graduate School of Medicine, 65
tration and therapeutic response, in contrast to that
Tsurumai, Showa, Nagoya, Aichi 466-8550, Japan. Email:
for imipramine, desipramine, and nortriptyline.2,3
Previous studies reported different results regard-
Received 14 April 2008; revised 11 June 2008; accepted 25 June2008.
ing the relationship between plasma amitriptyline
Journal compilation 2008 Japanese Society of Psychiatry and Neurology
Psychiatry and Clinical Neurosciences 2008; 62: 610–616
concentration and common adverse effects such as
cal Interview for DSM-IV, the subjects were found to
drowsiness and dry mouth. For example, although
be free from any physical or psychiatric disorders and
these adverse events were attributed to high plasma
were not taking medication. All subjects had been in
concentration of amitriptyline, correlation for low–
possession of a driving license for at least 10 years
moderate concentrations of amitriptyline was not
and had been driving a car daily (minimum,
5000 km/year). The study was approved by the ethics
Epidemiological data indicate that TCA users are
committee of the Nagoya University School of Medi-
twice as likely to be involved in traffic accidents as
cine, and written informed consent was obtained
compared to non-users.8,9 Various studies have dem-
from each subject prior to participation.
onstrated the harmful effects of TCA on driving per-formance.10 As for amitriptyline, impairment of road
Procedure
tracking performance and increase in brake reactiontime have been reported.11,12 Amitriptyline also has
All subjects were tested at approximately 09.30 hours
been linked to impairment of cognitive functions as
using the Stanford Sleepiness Scale (SSS),21 driving
well as driving performance. A single low dose of
tests, and cognitive tests. The entire testing lasted
amitriptyline impaired cognitive functions as mea-
approximately 1 h for each person. Following base-
sured on cognitive tests such as auditory vigilance
line assessment, the subjects were given capsules
test, tapping test, arithmetic test, digit symbol substi-
containing 25 mg amitriptyline in a double-blind
tution test, short term memory test, flicker-fusion
manner. The dose of 25 mg was selected because it
test, and choice reaction time test.13–19
is a recommended starting dose in Japan, and also
In our recent study we used simulator scenarios to
because the higher dose of amitriptyline might cause
examine car-following performance in the context
severe side-effects, possibly interrupting the experi-
of crowded urban roads and driving at relatively low
ments. Blood samples (10 mL) were collected 4 h
speeds as well as other driving tasks routinely inves-
after administration, because that is when maximum
tigated in other previous studies. Furthermore, cog-
plasma drug concentration occurs.22 The patients
nitive function was evaluated using the Wisconsin
were subjected to all the aforementioned tests
Card-Sorting Test (WCST), Continuous Performance
again after blood drawing. The blood samples were
Test (CPT), and N-back test. At 4 h after amitrip-
immediately centrifuged at 1700 g. for 10 min, and
the plasma was frozen at -30°C. Plasma ami-
following performance was significantly impaired,
triptyline concentrations were determined on high-
vigilance was reduced, and subjective somnolence
performance liquid chromatography, as described
previously.23 Five-point calibration curves were set up
Although the adverse effects of amitriptyline on
for the range 2–200 ng/mL. A linear response func-
driving performance and cognitive functions differ
tion was obtained, and the limit of quantification
across individuals, to the best of our knowledge there
was 2 ng/mL. The interday coefficient of variation
have been no studies reported on the relationship
for 4 days for plasma amitriptyline at 20 ng/mL
between plasma amitriptyline concentration on the
was 11.2%. The intraday coefficients of variation
one hand, and driving performance and cogni-
were 1.1–1.2% (n = 2). Amitriptyline has an active
tive functions on the other. Considering the afore-
metabolite, nortriptyline. Both amitriptyline and
mentioned factors, we examined the influence of
nortriptyline undergo benzylic hydroxylation, and
individual pharmacokinetic differences on driving
the hydroxylated nortriptyline metabolites are still
performance and cognitive functions using the same
active.24 Jiang et al. reported that the plasma concen-
tration of nortriptyline was considerably lower thanthat of amitriptyline after a single dose of amitrip-tyline.22 The plasma concentrations of nortriptyline
and its metabolites were not analyzed because thepresent study used only single low dosing and a short
Subjects
sampling interval after administration.
The sample consisted of 17 healthy male volunteers
The subjects received substantial training in driving
aged 30–42 years (mean Ϯ SD, 35.8 Ϯ 3.3 years).
and cognitive tests 1 or 2 weeks prior to the first
Based on health interviews and the Structured Clini-
testing; and in order to minimize the learning effects
Journal compilation 2008 Japanese Society of Psychiatry and Neurology
Psychiatry and Clinical Neurosciences 2008; 62: 610–616
the subjects were trained until they reached the
tion was used, and the performance was measured
plateau level. Furthermore, the subjects were prohib-
as the percentage of correct responses (accuracy,
ited from consuming alcohol or beverages contain-
ing caffeine for 12 h before taking the tests andwere requested to sleep adequately on the previousevening. On the test days the subjects were also pro-
Statistical analysis
hibited from ingesting substances that may induce
None of the outcome variables of the driving tests,
wakefulness, such as caffeine, supplement drinks,
cognitive tests, and subjective scales, except BRT
chewing gum, or candies because these substances
(harsh-braking test) and d’ (CPT), had a normal dis-
could exert a stimulating effect on their performance.
tribution. To clarify the correlations between plasma
During the intervals between the test series, the sub-
amitriptyline concentration and percent change in
jects were assigned certain light tasks to prevent them
performance, the Spearman rank-order correlation
coefficients (non-parametric) were calculated. PENand DMS were analyzed as difference not percent
Driving and cognitive tests
change, because their baseline values could be 0and percent change could not be calculated. BRT
We used a driving simulator (Toyota Central R&D
and d’ were analyzed using the Pearson product-
Labs, Nagakute, Japan) to examine three driving skills
moment correlation. In order to analyze the drug
that appeared to be associated with the recent traffic
effect, the baseline values were compared to that
accidents. The road-tracking test in the present study
obtained at 4 h after dosing using the Wilcoxon
was based on a road-tracking test that was developed
signed-rank test. A paired t test was used to analyze
previously.25,26 The subjects were instructed to drive at
the BRT and d’ data. All statistical tests were con-
a constant speed of 100 km/h and stabilize their
ducted using SPSS version 11 for Windows (SPSS
vehicles at the center of a gently winding road. The
Japan, Tokyo, Japan). Significance levels were set at
standard deviation of the lateral position (SDLP; cm),
which indicates weaving, was considered a perfor-mance measure. The car-following test required thesubjects to maintain a constant distance between
the cars (targeted distance of 5 m) in the contextof crowded urban roads driving at a speed of
Correlations between plasma amitriptyline
40–60 km/h. The coefficient of variation (CV) was
concentration and driving performance,
obtained by dividing the standard deviation of the
cognitive function, and
car-following distance (m) between the cars by the
subjective assessments
mean value, and it was considered a performancemeasure.27 Therefore, a smaller value of distance
The mean Ϯ SD plasma amitriptyline concentration
CV (DCV) would indicate a better performance. The
was 15.3 Ϯ 6.4 ng/mL (range, 8.5–32.9 ng/mL). The
harsh-braking test required the subjects to avoid
relationships between the plasma amitriptyline con-
crashing into the humanoid models that randomly
centration and driving performance, cognitive func-
ran on the road by harsh braking. The brake reaction
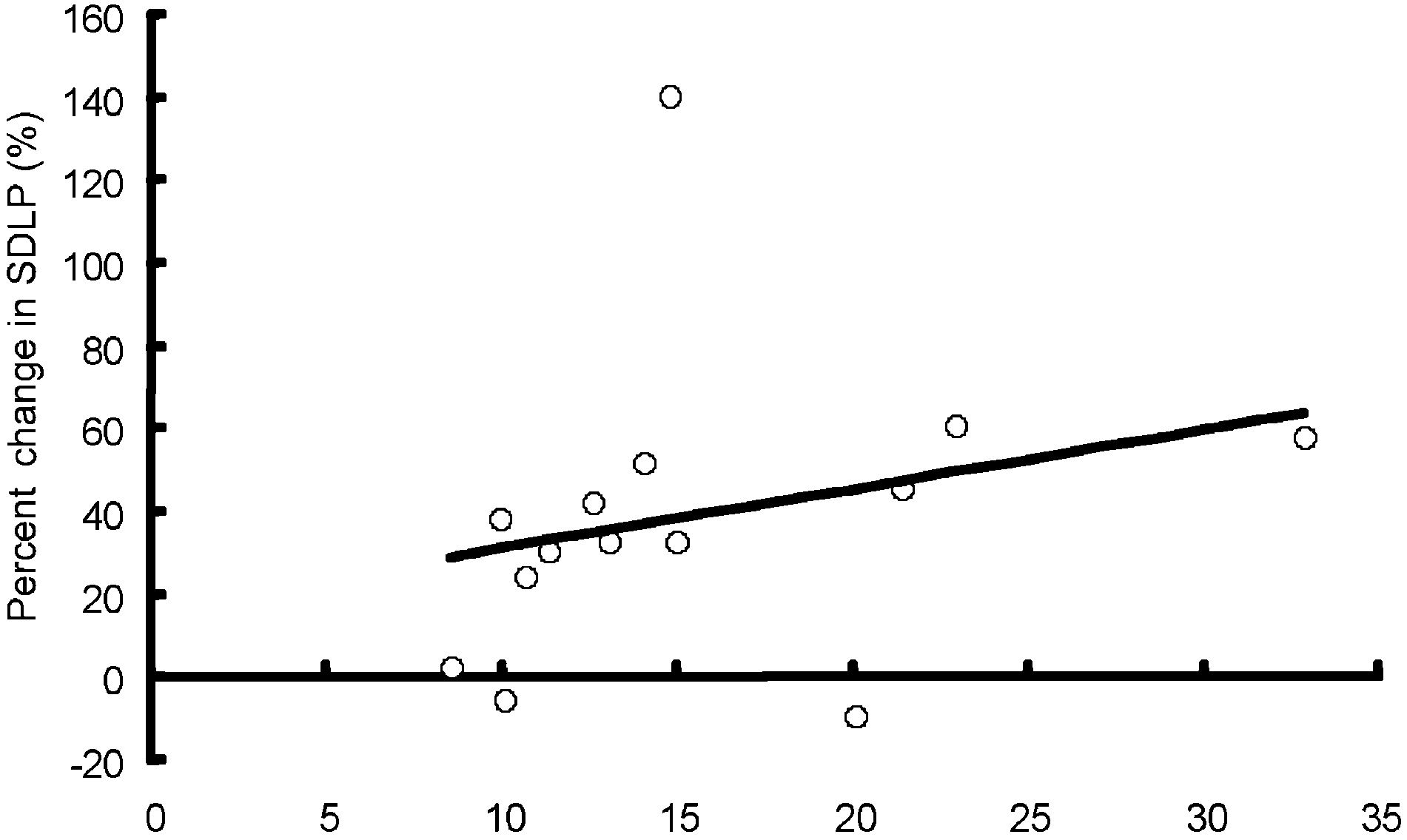
tion, and subjective assessments are shown in Fig. 1.
time (BRT; ms) was considered a performance
Data that indicate the coefficient of correlation of
measure. Each test lasted for 5 min and the details
-0.1 < r < 0.1 are not shown. A significant correlation
was observed between plasma amitriptyline con-
The three cognitive tests were examined using a
centration and percent change in SDLP (Fig. 1a).
computer. In the WCST the performance was mea-
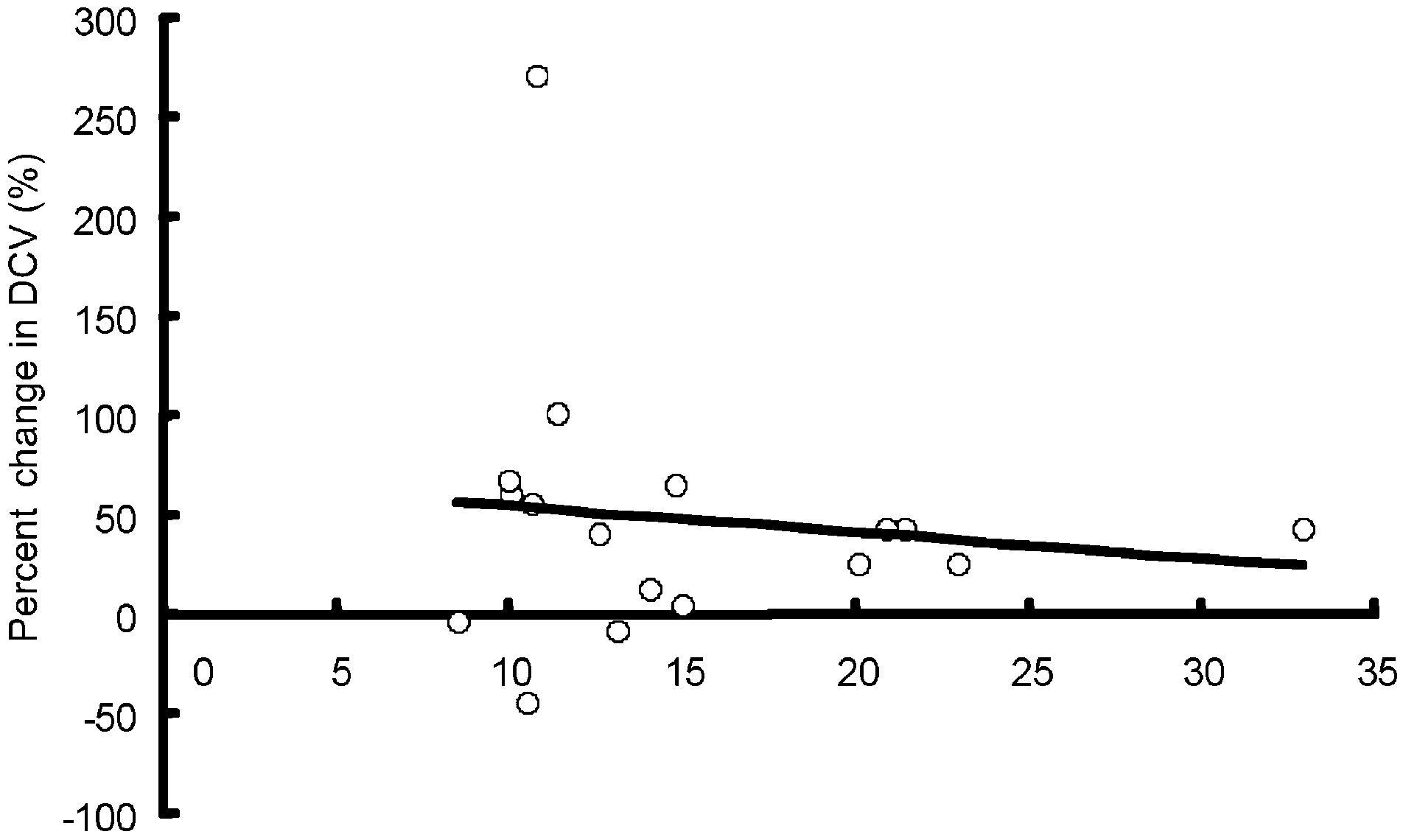
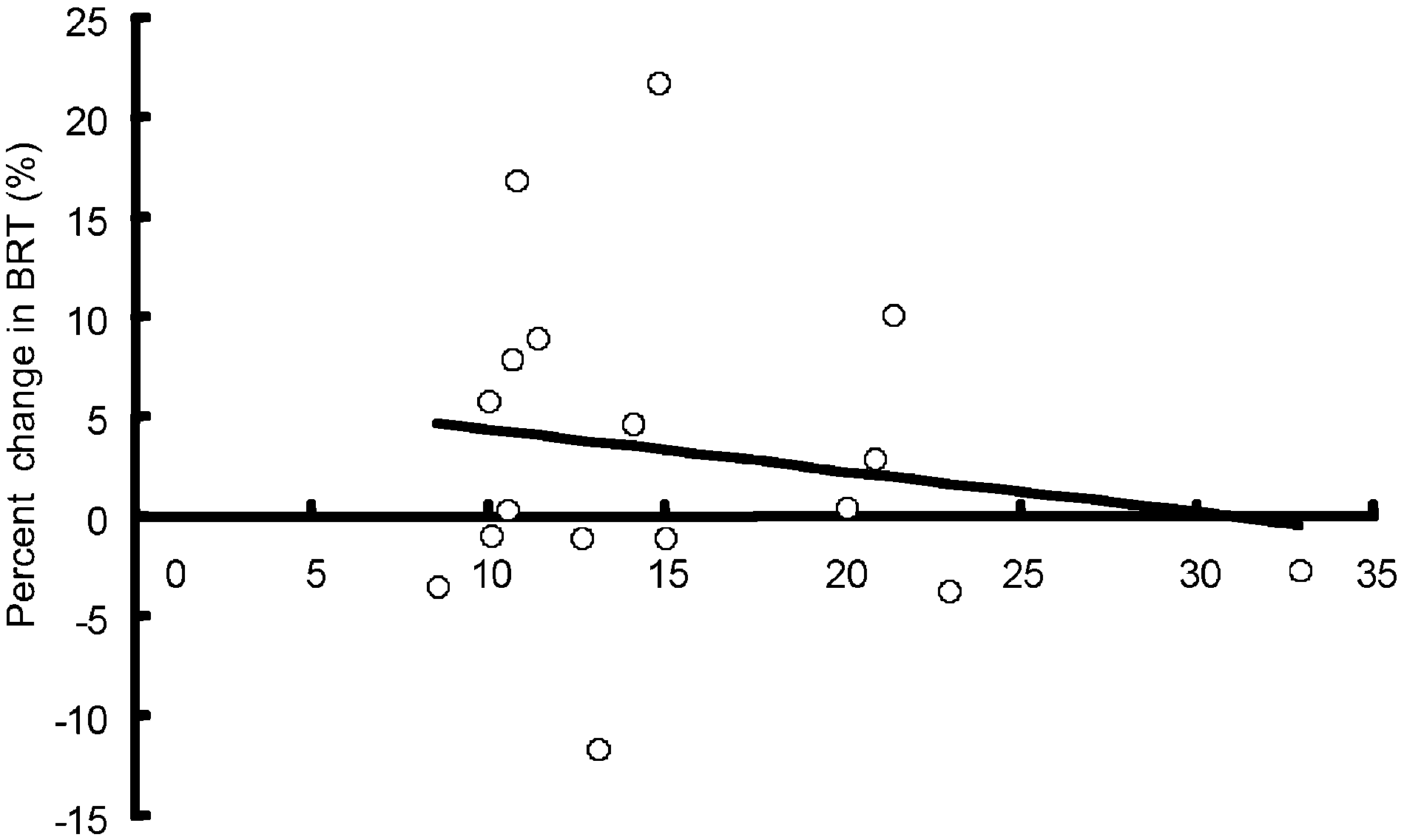
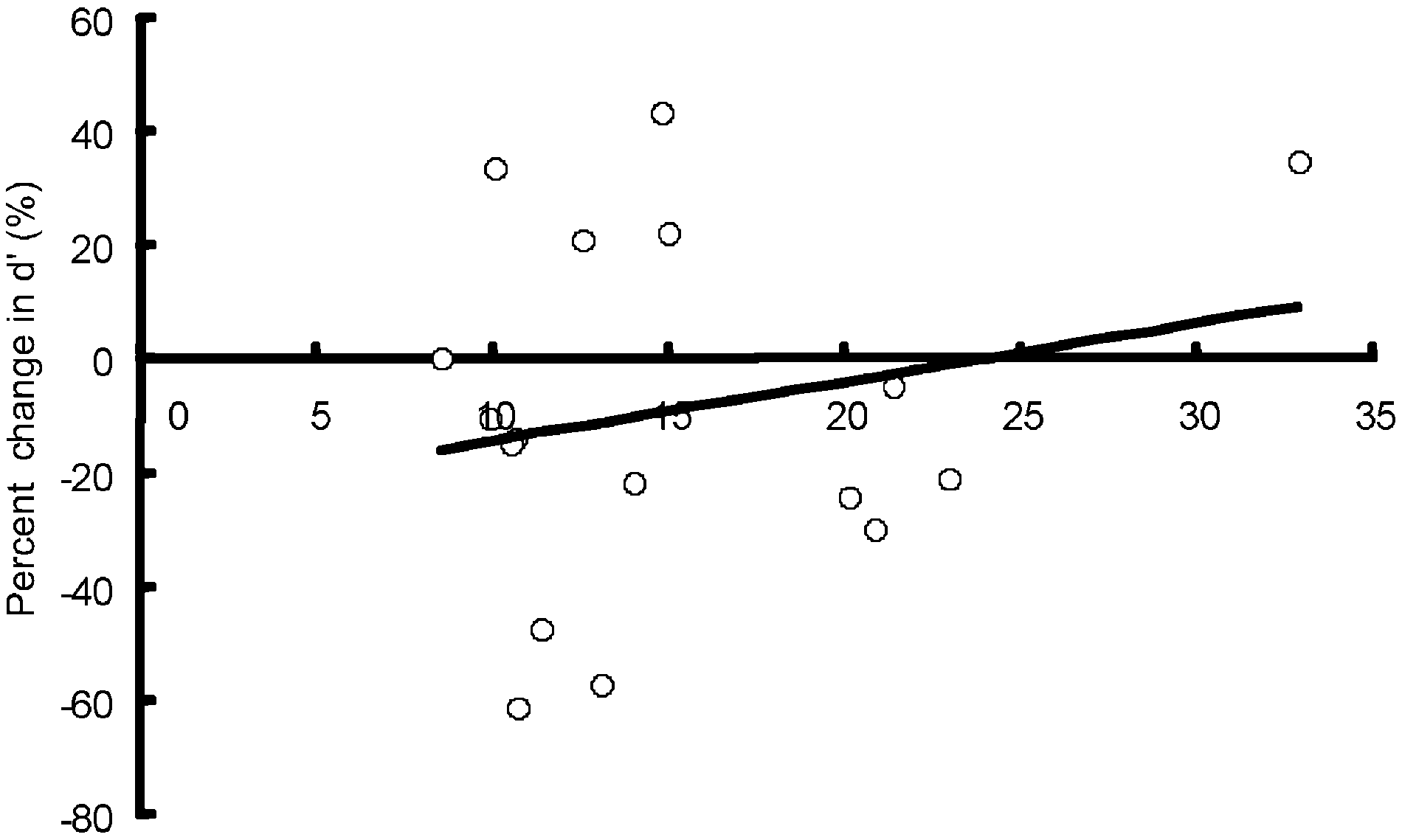
No significant correlations were detected between
sured using the following indices: category achieve-
plasma amitriptyline concentration and the remain-
ment (CA), perseverative errors of Nelson (PEN),
ing driving, cognitive, and subjective variables
and difficulty of maintaining set (DMS).28,29 In
(Fig. 1b–f). Percent change in CA, difference of PEN
the CPT the performance was measured using the
and percent change in SSS showed no significant cor-
signal detection index d-prime (d’), which is a
relations as follows: r = -0.070, P = 0.789 for CA,
measure of discriminability computed from hits and
r = 0.048, P = 0.855 for PEN and r = 0.035, P = 0.893
false alarms.30 In the N-back test a two-back condi-
2008 The AuthorsJournal compilation 2008 Japanese Society of Psychiatry and Neurology
Psychiatry and Clinical Neurosciences 2008; 62: 610–616
Plasma Amitriptyline Concentration (ng/mL)
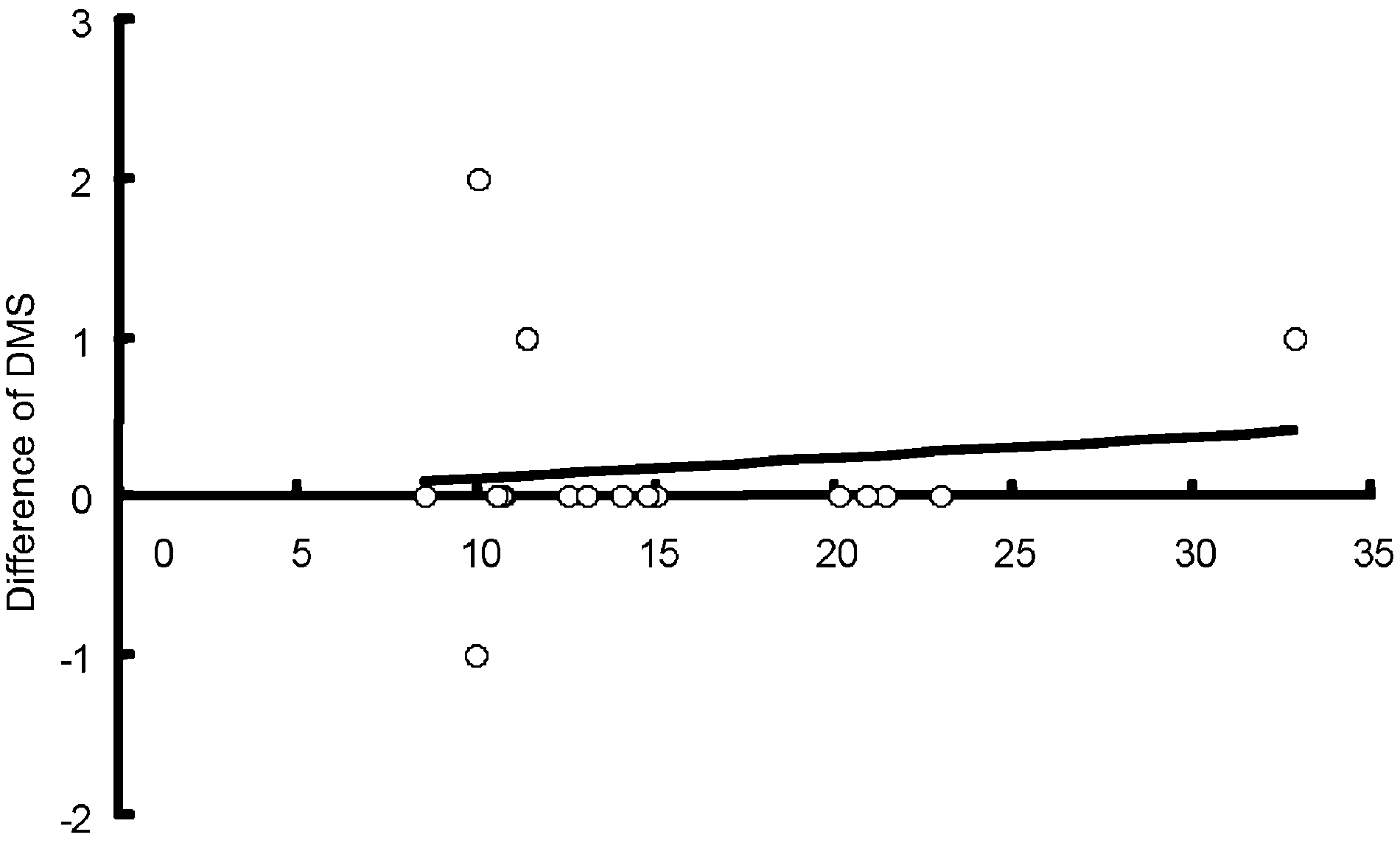
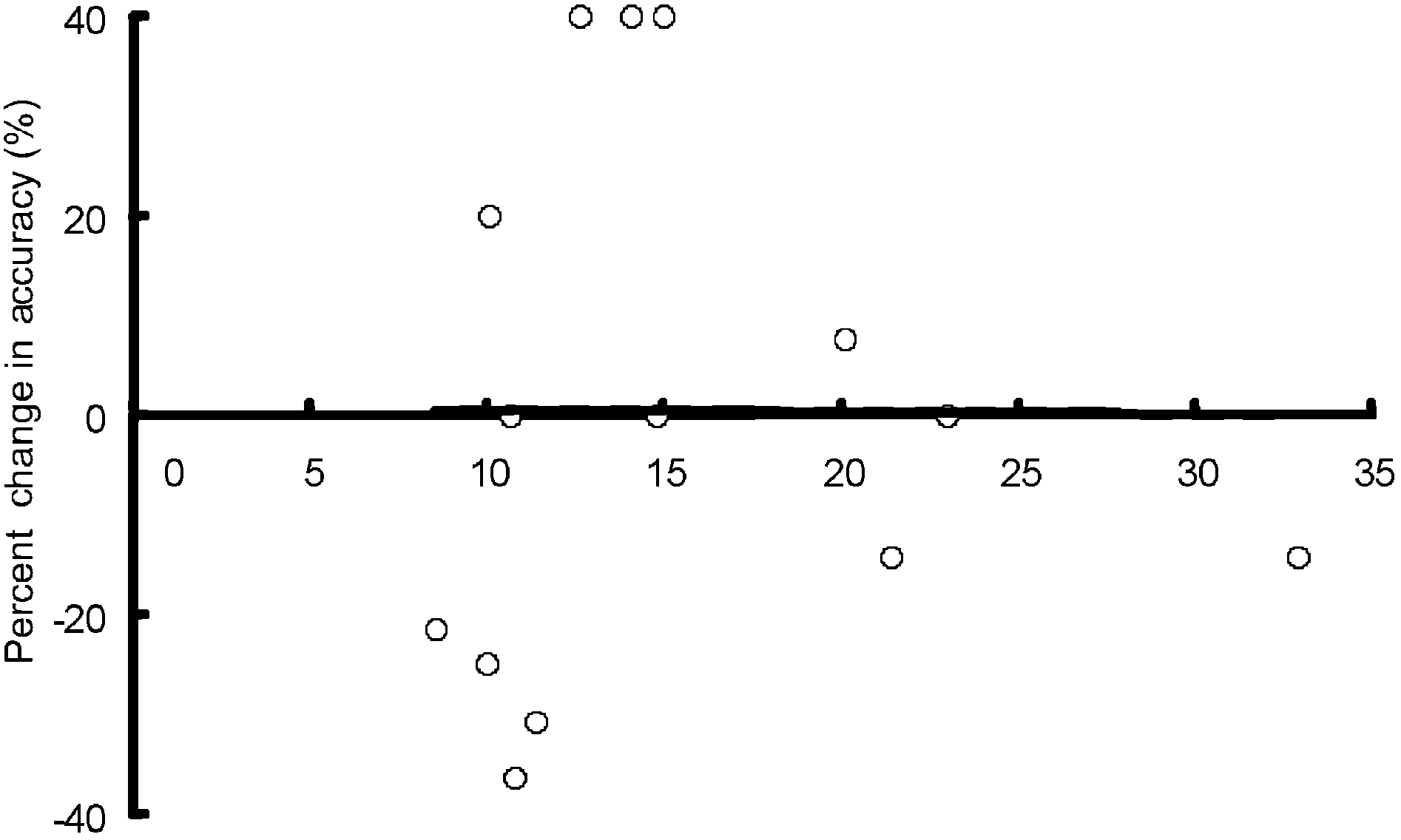
Figure 1. Relationship between plasma amitriptyline concentration and percent changes in the variables of driving performance, cognitive functions, and subjective somnolence. (Difference rather than percent change was used for (e) difficulty of maintaining set [DMS], because the baseline values of DMS can be 0 and hence, percent changes cannot be calculated.) (a) Percent change in standard deviation of the lateral position (SDLP; r = 0.543, P = 0.045); (b) percent change in distance coefficient of variation (DCV; r = -0.110, P = 0.673); (c) percent change in brake reaction time (BRT; r = -0.163, P = 0.532); (d) percent change in signal detection index d-prime (d’) in the Continuous Performance Test (r = 0.209, P = 0.420); (e) difference of DMS in the Wisconsin Card-Sorting Test (r = 0.132, P = 0.614); (f) percent change in accuracy in the N-back test (r = 0.260, P = 0.370). Due to non-completion of the assigned task and technical malfunctions, three subjects were excluded from statistical analyses for SDLP and N-back test.
Journal compilation 2008 Japanese Society of Psychiatry and Neurology
Psychiatry and Clinical Neurosciences 2008; 62: 610–616
significant correlation was observed between plasma
Effects of amitriptyline on driving
amitriptyline concentration and percent change in
performance, cognitive function, and
SSS scores. These values might be influenced by
subjective assessments
individual pharmacodynamic differences rather than
At 4 h after receiving the single dose of 25 mg ami-
individual pharmacokinetic differences. The same
triptyline, SDLP (P = 0.003), DCV (P = 0.006), CA
logic may be applied to the absence of correlations
(P = 0.035), and SSS score (P = 0.0002) were signifi-
between plasma amitriptyline concentration and
cantly impaired. The effect of amitriptyline on the
DCV and CA (WCST); therefore, further investiga-
remaining variables was not statistically significant.
tions should be conducted in this regard.
These data have been reported in our previous study.20
Several studies indicate cognitive impairments
in major depression patients.34–36 Richardson et al. reported that amitriptyline and fluoxetine showed
DISCUSSION
equal clinical improvement but patients receiving
The present results demonstrated a significant linear
amitriptyline did not perform as well on the verbal
correlation between plasma amitriptyline concentra-
learning task.37 The present results indicate that TCA
tion and percent change in SDLP. Baseline SDLP
including amitriptyline might affect recovered cogni-
was 38.9 Ϯ 10.8 cm, and at 4 h it increased to
tive function, even though clinical depressive symp-
51.3 Ϯ 12.7 cm. This increase of lateral swerving
might lead to traffic accidents. The plasma amitrip-
The present study has several limitations. First, it
tyline concentration, however, did not show a signifi-
used a single, low dose of amitriptyline. Therefore, we
cant relationship with (i) other driving performance
could not investigate the steady state condition, in
parameters of DCV and BRT; (ii) cognitive functions
which amitriptyline and its active metabolites exert
measured using the WCST, CPT, and N-back test; or
their influence. Second, the participants were limited
(iii) subjective somnolence, determined using the SSS.
to healthy adult male volunteers; therefore, women
In a previous study imipramine had a detrimental
who are prone to develop depression and the elderly
effect on driving performance measured as SDLP and
should be included in future studies. Third, the valid-
caused slight cognitive impairment as assessed on a
ity and sensitivity of the driving simulator used in the
memory scanning test.33 This memory test indicated
present study should be considered. Finally, we found
that the plasma drug concentration significantly cor-
a significant linear correlation between plasma ami-
related with reaction time change but not with SDLP
triptyline concentration and percent change in SDLP,
change. The present study found a significant corre-
but it is necessary to investigate this relationship under
lation between plasma concentration of amitriptyline
clinical therapeutic dose and steady-state conditions.
after a single dose and driving performance measuredas SDLP. Amitriptyline may have a concentration-dependent
ACKNOWLEDGMENTS
ability. Therapeutic monitoring of amitriptyline
This work was supported in part by research grants
would be useful for predicting the difficulties
from the Ministry of Education, Culture, Sports,
encountered while driving. The present results and
Science and Technology of Japan, the Ministry of
those of the van Laar et al. study33 do not agree,
Health of Japan, Labor and Welfare, Grant-in-Aid for
although both these studies used TCA. The method-
Scientific Research on Pathomechanisms of Brain
ological differences between the two studies might
Disorders from the Ministry of Education, Culture,
Sports, Science and Technology of Japan, MEXT
A previous review demonstrated that somnolence
Academic Frontier and the Japan Health Sciences
or sedation is the most important cause of driving
Foundation (Research on Health Sciences focusing
impairment in patients treated with antidepres-
sants.10 In our previous simulator study we also con-firmed a weak but significant association between thedetrimental effects of antidepressants on driving per-
REFERENCES
formance and increased subjective somnolence.20 In
1 Baumann P, Hiemke C, Ulrich S et al. The AGNP-TDM
the present study an acute dose of 25 mg amitrip-
expert group consensus guidelines: Therapeutic drug moni-
tyline strongly increased the SSS scores, but no
toring in psychiatry. Pharmacopsychiatry 2004; 37: 243–265.
2008 The AuthorsJournal compilation 2008 Japanese Society of Psychiatry and Neurology
Psychiatry and Clinical Neurosciences 2008; 62: 610–616
2 Task Force on the Use of Laboratory Tests in Psychiatry.
18 Kinirons MT, Jackson SH, Kalra L, Trevit RT, Swift CG. Com-
Tricyclic antidepressants: Blood level measurements and
puterised psychomotor performance testing: A comparative
clinical outcome: An APA Task Force report. Am. J. Psychiatry
study of the single dose pharmacodynamics of minaprine
1985; 142: 155–162.
and amitriptyline in young and elderly subjects. Br. J. Clin.
3 Orsulak PJ. Therapeutic monitoring of antidepressant drugs:
Pharmacol. 1993; 36: 376–379.
Guidelines updated. Ther. Drug Monit. 1989; 11: 497–507.
19 Nathan PJ, Sitaram G, Stough C, Silberstein RB, Sali A.
4 Preskorn SH, Fast GA. Therapeutic drug monitoring for anti-
Serotonin, noradrenaline and cognitive function: A prelimi-
depressants: Efficacy, safety, and cost effectiveness. J. Clin.
nary investigation of the acute pharmacodynamic effects of
Psychiatry 1991; 52 (Suppl.): 23–33.
a serotonin versus a serotonin and noradrenaline reuptake
5 Perry PJ, Zeilmann C, Arndt S. Tricyclic antidepressant con-
inhibitor. Behav. Pharmacol. 2000; 11: 639–642.
centrations in plasma: An estimate of their sensitivity and
20 Iwamoto K, Takahashi M, Nakamura Y et al. The effects of
specificity as a predictor of response. J. Clin. Psychopharma-
acute treatment with paroxetine, amitriptyline, and placebo
col. 1994; 14: 230–240.
on driving performance and cognitive function in healthy
6 Rodriguez de la Torre B, Dreher J, Malevany I et al. Serum
Japanese subjects: A double-blind crossover trial. Hum. Psy-
levels and cardiovascular effects of tricyclic antidepressants
chopharmacol. 2008; 23: 399–407.
and selective serotonin reuptake inhibitors in depressed
21 Hoddes E, Zarcone V, Smythe H, Phillips R, Dement WC.
patients. Ther. Drug Monit. 2001; 23: 435–440.
Quantification of sleepiness: A new approach. Psychophysiol-
7 Ulrich S, Lauter J. Comprehensive survey of the relationship
ogy 1973; 10: 431–436.
between serum concentration and therapeutic effect of ami-
22 Jiang ZP, Shu Y, Chen XP et al. The role of CYP2C19 in
triptyline in depression. Clin. Pharmacokinet. 2002; 41: 853–
amitriptyline N-demethylation in Chinese subjects. Eur. J.Clin. Pharmacol. 2002; 58: 109–113.
8 Ray WA, Fought RL, Decker MD. Psychoactive drugs and the
23 Duverneuil C, de la Grandmaison GL, de Mazancourt P,
risk of injurious motor vehicle crashes in elderly drivers. Am.
Alvarez JC. A high-performance liquid chromatography
J. Epidemiol. 1992; 136: 873–883.
method with photodiode-array UV detection for therapeutic
9 Leveille SG, Buchner DM, Koepsell TD, McCloskey LW, Wolf
drug monitoring of the nontricyclic antidepressant drugs.
ME, Wagner EH. Psychoactive medications and injurious
Ther. Drug Monit. 2003; 25: 565–573.
motor vehicle collisions involving older drivers. Epidemiol-
24 Halling J, Weihe P, Brosen K. The CYP2D6 polymorphism
ogy 1994; 5: 591–598.
in relation to the metabolism of amitriptyline and nortrip-
10 Ramaekers JG. Antidepressants and driver impairment:
tyline in the Faroese population. Br. J. Clin. Pharmacol.
Empirical evidence from a standard on-the-road test. J. Clin.
2008; 65: 134–138. Psychiatry 2003; 64: 20–29.
25 O’Hanlon JF, Haak TW, Blaauw GJ, Riemersma JB. Diaz-
11 Robbe HW, O’Hanlon JF. Acute and subchronic effects of
epam impairs lateral position control in highway driving.
paroxetine 20 and 40 mg on actual driving, psychomotor
Science 1982; 217: 79–81.
performance and subjective assessments in healthy volun-
26 O’Hanlon JF. Driving performance under the influence of
teers. Eur. Neuropsychopharmacol. 1995; 5: 35–42.
drugs: Rationale for, and application of, a new test. Br. J.
12 Hindmarch I, Subhan Z, Stoker MJ. The effects of zimeldine
Clin. Pharmacol. 1984; 18 (Suppl. 1): 121S–129S.
and amitriptyline on car driving and psychomotor perfor-
27 Uchiyama Y, Ebe K, Kozato A, Okada T, Sadato N. The
mance. Acta Psychiatr. Scand. Suppl.1983; 308: 141–146.
neural substrates of driving at a safe distance: A functional
13 Bye C, Clubley M, Peck AW. Drowsiness, impaired perfor-
MRI study. Neurosci. Lett. 2003; 352: 199–202.
mance and tricyclic antidepressants drugs. Br. J. Clin. Phar-
28 Heaton RK. The Wisconsin Card Sorting Test (Manual). Psy-
macol. 1978; 6: 155–162.
chological Assessment Resources, Odessa, FL, 1981.
14 Crome P, Newman B. A comparison of the effects of single
29 Kashima H, Honda T, Kato M et al. Neuropsychological
doses of mianserin and amitriptyline on psychomotor tests
investigation on chronic schizophrenia-aspect of its frontal
in normal volunteers. J. Int. Med. Res. 1978; 6: 430–434.
functions. In: Takahashi R, Flor-Henry P, Gruzelier J, Niwa
15 Peck AW, Bye CE, Clubley M, Henson T, Riddington C. A
S (eds). Cerebral Dynamics, Laterality and Psychopathology.
comparison of bupropion hydrochloride with dexamphet-
Elsevier, Amsterdam, 1987; 337–345.
amine and amitriptyline in healthy subjects. Br. J. Clin.
30 Cornblatt BA, Risch NJ, Faris G, Friedman D, Erlenmeyer-
Pharmacol. 1979; 7: 469–478.
Kimling L. The continuous performance test, identical pairs
16 Ogura C, Kishimoto A, Mizukawa R et al. Influence of single
version (CPT-IP): I. New findings about sustained attention
doses of dothiepin and amitriptyline on physiological mea-
in normal families. Psychiatry Res. 1988; 26: 223–238.
sures and psychomotor performance in normal young
31 Callicott JH, Bertolino A, Mattay VS et al. Physiological dys-
and elderly volunteers. Neuropsychobiology 1983; 10: 103–
function of the dorsolateral prefrontal cortex in schizophre-
nia revisited. Cereb. Cortex 2000; 10: 1078–1092.
17 Tiller JW. Antidepressants, alcohol and psychomotor perfor-
32 Callicott JH, Egan MF, Mattay VS et al. Abnormal fMRI
mance. Acta Psychiatr. Scand. Suppl. 1990; 360: 13–17.
response of the dorsolateral prefrontal cortex in cognitively
Journal compilation 2008 Japanese Society of Psychiatry and Neurology
Psychiatry and Clinical Neurosciences 2008; 62: 610–616
intact siblings of patients with schizophrenia. Am. J. Psychia-
35 Porter RJ, Gallagher P, Thompson JM, Young AH. Neuro-
try 2003; 160: 709–719.
cognitive impairment in drug-free patients with major
33 van Laar MW, van Willigenburg AP, Volkerts ER. Acute and
depressive disorder. Br. J. Psychiatry 2003; 182: 214–
subchronic effects of nefazodone and imipramine on
highway driving, cognitive functions, and daytime sleepi-
36 Airaksinen E, Larsson M, Lundberg I, Forsell Y. Cognitive
ness in healthy adult and elderly subjects. J. Clin. Psychop-
functions in depressive disorders: Evidence from a
harmacol. 1995; 15: 30–40.
population-based study. Psychol. Med. 2004; 34: 83–91.
34 Murphy FC, Michael A, Robbins TW, Sahakian BJ. Neurop-
37 Richardson JS, Keegan DL, Bowen RC et al. Verbal learning
sychological impairment in patients with major depressive
by major depressive disorder patients during treatment with
disorder: The effects of feedback on task performance.
fluoxetine or amitriptyline. Int. Clin. Psychopharmacol. 1994;
Psychol. Med. 2003; 33: 455–467. 9: 35–40.
2008 The AuthorsJournal compilation 2008 Japanese Society of Psychiatry and Neurology
Moral thinking: foundations, approaches and applications Henry Haslam www.moralmind.co.uk Introduction: free thinking Good morning. It is a great privilege to be invited to speak here, in the Conway Hall, home of the South Place Ethical Society, with its fine tradition of promoting moral discourse and free thinking. To me, as a Christian, the Christian faith makes an excelle
MIR Guidelines Regarding Pre-Treatment of Patients Undergoing Contrast-Enhanced MRI 1. At the time of scheduling, it should be determined if the patient has had a prior reaction to either gadolinium-based (MR) or iodinated contrast agents. a. If there is no history of a prior reaction , then no pre-treatment is needed. b. If the patient has had a prior reaction to an MR contrast agen
 Psychiatry and Clinical Neurosciences 2008; 62: 610–616
Psychiatry and Clinical Neurosciences 2008; 62: 610–616