Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Combination of r,r-glycopyrrolate, rolipram and budesonide for the treatment of inflammatory diseases - european patent office ep1971369 b
EP 1 971 369 B1 EUROPEAN PATENT SPECIFICATION A61K 31/40 (2006.01) A61K 31/58 (2006.01) 19.08.2009 Bulletin 2009/34 A61K 31/4015 (2006.01) A61P 11/00 (2006.01) A61P 29/00 (2006.01) A61P 1/04 (2006.01)
(21) Application number: 06829226.7 A61P 11/06 (2006.01) A61P 13/12 (2006.01) A61P 17/06 (2006.01) A61P 19/02 (2006.01) A61P 25/28 (2006.01) A61P 37/00 (2006.01)
Date of filing: 01.12.2006 A61P 37/08 (2006.01) PCT/EP2006/011536 WO 2007/071313 (28.06.2007 Gazette 2007/26)
(54) COMBINATION OF R,R-GLYCOPYRROLATE, ROLIPRAM AND BUDESONIDE FOR THE TREATMENT OF INFLAMMATORY DISEASES
KOMBINATION VON R,R-GLYCOPYRROLAT, ROLIPRAM UND BUDESONID ZUR BEHANDLUNG VON ENTZÜNDUNGSKRANKHEITEN
COMBINAISON DE GLYCOPYRROLATE, DE ROLIPRAM ET DE BUDESONIDE POUR LE TRAITEMENT DE MALADIES INFLAMMATOIRES
• KASTRUP, Horst AT BE BG CH CY CZ DE DK EE ES FI FR GB GR 48161 Münster (DE) HU IE IS IT LI LT LU LV MC NL PL PT RO SE SI • BAUHOFER, Artur 35039 Marburg (DE) • CNOTA, Peter 61348 Bad Homburg (DE) • SZELENYI, Istvan
(30) Priority: 21.12.2005 US 752058 P 90571 Schwaig (DE)
(43) Date of publication of application:
24.09.2008 Bulletin 2008/39 WO-A-01/76575 WO-A-20/05074918 WO-A-20/05074983 WO-A-20/05082413 WO-A-20/05115462 US-A1- 2005 107 420 09006788.5 US-A1- 2005 148 562
(73) Proprietor: MEDA Pharma GmbH & Co. KG • PAHL ET AL: "Synergistic effects of the anti- 61352 Bad Homburg (DE) cholinergic R,R-glycopyrrolate with anti- inflammatory drugs" BIOCHEMICAL PHARMACOLOGY, vol. 72, no. 12, 21 November • MAUS, Joachim 2006 (2006-11-21), pages 1690-1696, 63165 Mühlheim (DE) XP005774405 ISSN: 0006-2952
Note: Within nine months of the publication of the mention of the grant of the European patent in the European PatentBulletin, any person may give notice to the European Patent Office of opposition to that patent, in accordance with the
Implementing Regulations. Notice of opposition shall not be deemed to have been filed until the opposition fee has beenpaid. (Art. 99(1) European Patent Convention). EP 1 971 369 B1 Description
dominantly characterized by eosinophils and CD4+ lym-phocytes, neutrophil granulocytes, CD8+ lymphocytes
The invention relates to novel combination of
and macrophages appear to play a major role in the
R,R-glycopyrrolate, rolipram and budesonide process for
pathogenesis of COPD (Saetta et al. Am J Respir Crit
its production and its use for the treatment of inflamma-
Care Med 1999; 160:711-7, Shapiro Am J Respir Crit
tory diseases, preferably respiratory diseases as bron-
chial asthma and chronic obstructive pulmonary diseas-
There is now strong evidence that airway in-
es (COPD) or rheumatic or autoimmune diseases.
flammation is a predominant underlying problem in pa-
Asthma bronchiale, affecting as many as 10%
of individuals in industrialized nations, is characterized
The pathophysiology of asthma involves an in-
by bronchoconstriction, chronic airway inflammation, air-
teractive network of molecular and cellular interactions,
way hyperreactivity, and mucosal oedema. Airway re-
although the contribution of each individual factor is prob-
modelling and altered noncholinergic, nonadrenergic
ably different from patient to patient depending on the
neurotransmission may contribute to irreversible airway
setting and stimulus. Major participants in the develop-
obstruction and reduction of pulmonary function. Asthma
ment of an asthma phenotype include the triggering stim-
is characterized by recurrent episodes of breathless-
uli such as the allergens themselves, cells such as T
ness, wheezing, coughing, and chest tightness, termed
cells, epithelial cells and mast cells that produce a variety
exacerbations. The severity of exacerbations can range
of cytokines including tumor necrosis factor-alpha (TN-
from mild to life threatening. The exacerbations can be
Fα), interleukin(IL)-5, granuloyte-macrophage colony-
a result of exposure to e.g. respiratory infections, dust,
stimulating-factor (GM-CSF), IL-3, IL-4 and IL-13 and
mould, pollen, cold air, exercise, stress, tobacco smoke,
chemokines such as eotaxin, adhesion molecules, etc.
and air pollutants. Bronchial asthma has emerged as a
Unfortunately, much less is known about the
major public health problem worldwide over the past 20
pathogenesis of COPD than that of asthma. Recent stud-
years. Although data indicate that current asthma thera-
ies have greatly expanded the understanding of patho-
pies led to limited decreases in death rates, it continues
genetic mechanisms underlying COPD. Thus, there is
to be a significant health care problem. It still is one of
consent that COPD is also an inflammatory disease.
the leading causes of preventable hospitalization world-
From the present pathogenetical point of view, COPD is
wide and accounts for several million lost workdays.
defined as a progressive and not fully reversible airway
Along with the increase in asthma prevalence, the costs
obstruction with predominantly neutrophilic airway in-
associated with this disease have also risen dramatically.
flammation. In COPD, the predominant inflammatory cell
types are CD8+ T lymphocytes, macrophages, and neu-
(COPD) is very common world-wide. It is primarily asso-
trophils. Neutrophils and neutrophilic inflammatory mark-
ciated with past and present cigarette smoking but the
ers including IL-8, TNFα and LTB4 are increased in the
fact that the society gets older also plays an even con-
airways of COPD patients (Yamamoto et al. Chest 1997;
tinuously increasing role. The prevalence of COPD varies
112:505-10, Keatings et al. Am J Respir Crit Care Med
between 3% and 10% with a steadily increasing trend.
Although COPD is a leading cause of illness and death,
The current management of asthma and COPD
its recognition as a public health problem has been slow
is focussed on the improvement of the lung function of
to evolve despite the rising mortality rate for COPD and
patients. In both diseases but especially in COPD, the
the decline in death rates for most of the cardiovascular
first step is smoking cessation. There is evidence that
diseases (Hurd Chest 2000; 117(2 Suppl):1S-4S). Addi-
smoking reduction or cessation may result in improve-
tionally, COPD imparts substantial economic burden on
ment of some respiratory parameters.
individuals and society. COPD is a disease characterised
Bronchoconstriction occurs due to bronchial
by chronic inflammation and irreversible airflow obstruc-
smooth muscle spasm and airway inflammation with
tion with a decline in the lung function parameter FEV1
oedema. Whilst it is known that β2-adrenoceptor agonists
that is more rapid than normal. The disease has two major
provide symptomatic relief of patients suffering from asth-
aspects of pathology, namely chronic bronchitis, charac-
ma or COPD, another component of these airway disor-
terised by mucus hypersecretion from the conducting air-
ders, i.e. inflammation often requires separate treatment.
ways, and emphysema, characterised by destructive
Typically this may involve treatment with a glucocorticoid,
or a PDE4 inhibitor, respectively. Currently available glu-
cocorticoids include beclomethasone, triamcinolone,
problems characterised by a chronic inflammatory disor-
budesonide, fluticasone, mometasone, ciclesonide,
der of the airways. Airflow obstruction and airway inflam-
loteprednol, etiprednol, flunisolide. PDE4 inhibitors are
mation are features of asthma as well as COPD. Although
now under clinical development. Some of them are short-
the airway inflammation in asthma and COPD, respec-
ly before approval, e.g. roflumilast, AWD-12 281.
tively, involve different cell types, both diseases are of
Bronchoconstriction and inflammation are also
chronic inflammatory nature associated with cellular in-
associated with increased bronchial mucus production
filtration and activation. While bronchial asthma is pre-
and possible bronchial plugging, which can be treated
EP 1 971 369 B1
with anticholinergics, such as ipratropium, oxitropium, ti-
NM. Clin Immunol Immunopathol 1997;84:223-43).
otropium, glycopyrrolate and in particular the RR enan-
Autoimmune diseases are disorders in which
the immune system produces antibodies against the
Bronchodilators (ß2-adrenoceptor agonists and
body’s own cells, destroying healthy tissue. These mis-
anticholinergics) are now the mainstay of symptomatic
directed immune responses are referred to as autoim-
therapy. Short- and long-acting β2-adrenoceptor ago-
munity, which can be demonstrated by the presence of
nists such as salbutamol, fenoterol, salmeterol, formot-
autoantibodies or T lymphocytes reactive with host anti-
erol are established therapeutics in the symptomatic
gens. Human autoimmune diseases can be divided into
COPD management. Of the short-acting antimuscarinic
two categories: organ-specific and systemic. In organ-
drugs, ipratropium is widely used although antimuscarin-
specific autoimmune disease (e.g. Graves’ disease,
ic drugs are rather less efficacious in the relief of an asth-
Hashimoto’s thyroiditis, type 1 diabetes mellitus), auto-
ma attack than the β2-adrenoceptor agonists (Rodrigo
reactivity is directed to antigens unique to a single organ.
and Rodrigo, Chest 2003; 123:1908-15). Recently, tio-
In systemic autoimmune disease (e.g. RA, MS, SLE),
tropium, a long-acting anticholinergic with a certain pref-
autoreactivity is largely directed toward a broad range of
erence to M3-muscarinic receptors has now been intro-
antigens and involves a number of tissues.
duced world-wide (Hansel and Bames, Drugs Today
Systemic lupus erythematosus (SLE) is a
(Barc) 2002; 38:585-600, Koumis and Samuel, Clin Ther
chronic, usually life-long, potentially fatal autoimmune
2005; 27:377-92). Relatively sufficient anti-inflammatory
disease. SLE is notable for unpredictable exacerbations
therapy with glucocorticoids are available for asthma.
and remissions and a predilection for clinical involvement
However, they are less effective in COPD. Additionally,
of the joints, skin, kidney, brain, lung, heart, and gastroin-
tiotropium reduces COPD exacerbations and related
hospitalisations compared to placebo and ipratropium
Rheumatoid arthritis (RA), juvenile idiopathic
(Barr et al. Cochrane Database Syst Rev 2005; (2):
arthritis, the seronegative spondylo-arthropathies includ-
CD002876). Further long-acting anticholinergics are now
ing psoriatic arthritis, and systemic lupus erythematosus
under development. They are more convenient to use
are all examples of rheumatic diseases in which inflam-
for patients with advanced disease who require mainte-
mation is associated with skeletal pathology. RA is the
nance therapy with bronchodilators, and have been
most common inflammatory joint disease and a major
shown to provide superior efficacy compared with short-
cause of functional disability, morbidity, and premature
mortality. Inflammation of the synovial membrane sur-
The basic tenet of asthma therapy has centred
rounding a joint leads to swollen, tender, and stiff joints.
on optimal management of the underlying inflammatory
This may be accompanied by fatigue, weight loss, anxi-
process. The most recent expert recommendations
strongly support the use of inhaled glucocorticoids. Bron-
Rheumatoid arthritis (RA) usually requires life-
chodilators are used for transient relief of symptoms in
long treatment. Nonsteroidal anti-inflammatory drugs
these patients and for additional symptomatic control in
(NSAIDs) have been the cornerstone of therapy for RA.
patients who have persistent symptoms despite inhaled
NSAIDs reduce pain and inflammation and allow for im-
glucocorticoid therapy (http://www.ginasthma.com/). In
provements in mobility and function. Aspirin and other
well-defined COPD, therapeutic alternatives vary. Be-
NSAIDs, such as ibuprofen, diclofenac, fenoprofen, in-
cause there is no currently accepted pharmacologic ther-
domethacin, naproxen are strongly anti-flammatoric and
apy that alters the natural history of the disease, thera-
analgetic. Their strong gastrointestinal side effects often
peutic emphasis is placed on symptom relief. Unlike in
limit their use. Cyclooxygenase-2 (COX-2) inhibitors
asthma therapy, bronchodilators play a prominent role in
were initially believed to cause fewer stomach problems
the initial therapy for symptomatic COPD patients. In this
than classical NSAIDs. However, the use of COX-2 in-
regard, long-acting ß2-adrenoceptor agonists and the
hibitors is considerable limited due their cardiovascular
new long-acting anticholinergic agent (tiotropium) offer
undesired effects. Corticosteroids, used alone or in con-
distinct advantages. In contrast, inhaled glucocorticoids
junction with other medications, may reduce the symp-
appear to have a more limited role in COPD. On the other
tomatology associated with RA. In fact, corticosteroids
hand, inhaled glucocorticoids have been shown to have
reduce inflammation in RA. However, because of poten-
beneficial effects on health status and to decrease exac-
tial long-term side effects (e.g. gastrointestinal ulcera-
tion, osteoporosis, cataract development, glaucoma,
Autoimmune diseases (e.g. rheumatoid arthri-
etc.), corticosteroid use is usually limited to short courses
tis [RA], systemic lupus erythematosus [SLE], multiple
and low doses where possible. Drugs like anticholiner-
sclerosis [MS], glomerulonephritis, inflammatory bowel
gics are frequently used in combination with GCs to re-
diseases [Morbus Cohn, colitis ulcerosa], psoriasis) be-
duce ulcer development induced by GCs.
long to the major health problems worldwide. Autoim-
The current standard of care is aggressive ther-
mune diseases are among the ten leading causes of
apy with anti-inflammatory drugs and disease-modifying
death. Most of autoimmune diseases require lifelong
treatment (Jacobson DL, Grange SJ, Rose NR, Graham
DMARDs most frequently are used in various
EP 1 971 369 B1
Tumor necrosis factor (TNF) inhibitors are a rel-
The pharmacodynamic properties of all these
atively new class of medications used to treat autoim-
drug classes, anticholinergics (especially R,R-glycopyr-
mune disease. They include etanercept (soluble TNF re-
rolate), PDE4 inhibitors, and/or inhaled GCs complement
ceptor), infliximab (monoclonal antibody against TNF),
one another and result in more efficacious treatment of
adalimumab (human TNF antiobody) and anakinra (re-
the mentioned diseases, which is surprisingly over-addi-
combinant human interleukin-1 receptor antagonist).
tive even compared to the dual combinations. Further-
The term inflammatory bowel disease (IBD)
more, since the doses of monocompounds are in the
describes a group of chronic inflammatory disorders of
combination lower, the incidence of adverse effects can
unknown causes involving the gastrointestinal tract
be reduced by using the combination. Additionally, the
(GIT). Patients with IBD can be divided into two major
patients’ compliance is also increased.
groups, those with ulcerative colitis (UC) and those with
Antimuscarinic treatment of asthma and
Crohn’s disease (CD). In patients with UC, there is an
COPD has a relatively long history leading to its present
inflammatory reaction primarily involving the colonic mu-
day use as an effective bronchodilating drug for obstruc-
cosa. The inflammation is typically uniform and continu-
tive pulmonary diseases. Anticholinergic agents are ex-
ous with no intervening areas of normal mucosa. CD dif-
emplified by the belladonna alkaloids atropine and sco-
fers from UC in that the inflammation extends through all
polamine, which inhibit the muscarinic action of acetyl-
layers of the intestinal wall and involves mesentery as
choline on structure innervated by postganglionic cholin-
well as lymph nodes. CD can occur anywhere along the
ergic nerves. These agents typically inhibit bronchocon-
striction by relaxing of smooth muscles and cause con-
Current therapies comprise aminosalicylates,
siderable bronchodilation. Anticholinergic agents also
drugs that contain 5-aminosalicyclic acid (5-ASA), which
are known to exert central effects which include pupil
help to control inflammation. Sulfasalazine is mainly use-
dilatation and stimulation and/or depression of the central
ful in colonic disease because the active compound, 5-
nervous system. Novel anticholinergic pharmaceuticals
aminosalicylic acid (5-ASA), is released in the large bow-
have been developed which have a limited capacity to
el by bacterial degradation of the parent compound.
pass across the blood-brain barrier, and therefore have
Products such as mesalamine that release 5-ASA in the
a limited capacity to produce central effects. Examples
distal small bowel secondary to pH changes are more
of these agents are the quaternary ammonium com-
useful in patients with small intestinal Crohn disease.
pounds methscopolamine, ipratropium, oxitropium, tio-
Other 5-ASA agents, such as olsalazine, mesalamine,
tropium and the enantiomers of glycopyrrolate. Some ex-
and balsalazide, have a different carrier, fewer side ef-
perts recommend ipratropium as the first choice. It has
fects, and may be used by people who cannot take sul-
a very slow onset and can be used as maintenance ther-
fasalazine. Immunomodulators such as azathioprine and
apy for people with emphysema and chronic bronchitis
6-mercapto-purine reduce inflammation by affecting the
with few severe side effects. However, a patient should
not take more than 12 inhalations per day. The recently
Since TNF is a key inflammatory cytokine and
introduced tiotropium has a long duration of action and
mediator of intestinal inflammation, compounds directed
against this cytokine such as infliximab are promising in
Anticholinergic medications have been accept-
IBD. In certain cases, immunosuppressive agents: cy-
ed as an important treatment modality in COPD and
closporine A, tacrolimus, mycophenolate mofetil may be
chronic asthma. The anticholinergic bronchodilator, the
muscarinic receptor antagonist, used in this invention will
Glycopyrrolate belongs to the so-called anti-
be a long-acting compound. Any compound of this type
cholinergic drugs and antagonizes the neurotransmitter
can be used in this combination therapy approach. By
acetylcholine at its receptor site. This effect leads to a
long-lasting it is meant that the drug will have an effect
considerable bronchodilatation and a reduced mucus se-
on the bronchi that lasts around 12 hours or more, up to
cretion. To date, one of the most effective medications
24 hours. The recently approved long acting inhaled an-
for airway inflammation is inhaled glucocorticoids
ticholinergic drug, tiotropium, produces sustained bron-
(GCs). These compounds practically inhibit all important
chodilation throughout the 24 hour day (Calverley et al.
inflammatory processes involved in asthma and partly in
Thorax 2003a; 58:855-60). In fact, bronchodilators im-
COPD, at least, to a considerable extent. Inhibitors of
prove symptoms and quality of life, in COPD patients,
the isoenzyme PDE4 reduce the inflammatory process-
but, with the exception of tiotropium, they do not signifi-
cantly influence the natural course of the disease (Car-
A cornerstone in the management of asthma
amori and Adcock, Pulm Pharmacol Ther 2003; 16:
and COPD is the control of airway inflammation. All drug
classes mentioned above are able to reduce airway in-
Glycopyrrolate, a quaternary ammonium anti-
flammation to various extents. Therefore, our intention
cholinergic compound, consists of four stereoisomers. It
was to combine these drug classes with the aim to im-
is poorly absorbed from mucus membranes, thus reduc-
prove the bronchodilatory effect and to enhance the anti-
ing anticholinergic side effects (Ali-Melkkila et al. Acta
EP 1 971 369 B1
Anaesthesiol Scand 1993; 37:633-42). Glycopyrrolate
prove the health status of these patients (Nishimura et
possesses no selectivity in its binding to the M1-M3 re-
al. Chest 1999; 115:31-7, Selroos, Curr Med Res Opin
ceptors. Kinetics studies, however, showed that glycop-
2004; 20:1579-93). But it has to be admitted that current
yrrolate dissociates slowly from M3 muscarinic receptors
pharmacological treatment of COPD is unsatisfactory,
(Haddad et al. Br J Pharmacol 1999; 127:413-20). Sim-
as it does not significantly influence the severity of the
ilarly to tiotropium, this behavior explains glycopyrrolate’s
disease or its natural course. In general, inhaled gluco-
relative receptor selectivity and its long duration of action.
corticoids have relatively little impact on the inflammatory
Indeed, there is evidence that racemic glycopyrrolate
processes that characterize COPD (Adcock and Chung,
produces considerable and long-lasting bronchodilatory
Curr Opin Investig Drugs 2002; 3:58-60) and are not suit-
effects both in asthmatic and in COPD patients (Walker
able for monotherapy in COPD but can be helpfully com-
et al. Chest 1987; 91:49-51, Schroeckenstein et al. J Al-
bined with an inhaled bronchodilator (Calverley et al. Eur
lergy Clin Immunol 1988; 82:115-9, Gilman et al. Chest
Respir J 2003b; 22:912-9, Calverley Semin Respir Crit
1990; 98:1095-8, Cydulka and Emerman, Ann Emerg
Care Med 2005; 26:235-45). They have, however, been
Med 1995; 25:470-3, Hansel et al. Chest 2005; 128:
shown to decrease the frequency of exacerbations and
1974-9). As asthma and COPD are characterized by in-
improve quality of life in patients with COPD (Calverley
creased mucus secretions, the antisecretory effect of an-
Semin Respir Crit Care Med 2005; 26235-45).
ticholinergics such glycopyrrolate is an additional advan-
The administration of inhaled glucocorticoids or
tage for their use in the therapy of these diseases.
anticholinergics (e.g. ipratropium) reduced the risk of
A cornerstone in the management of asthma
hospitalization of COPD patients (Rascati et al. Clin Ther
and COPD is the control of airway inflammation.
2005; 27:346-54). The combination of long-acting mus-
Inhaled glucocorticoids (GCs) are the most
carinic antagonists and inhaled glucocorticoids is more
effective long-term therapy in controlling chronic asthma
efficacious in asthma and COPD than either alone. In-
symptoms (Barnes Ernst Sobering Res Found Work-
deed, there is evidence that corticosteroid/muscarinic
shop. 2002; 40:1-23). Randomized, controlled clinical
antagonist combination therapy has complementary, ad-
studies confirm the efficacy of early intervention with in-
ditive, or synergistic inhibitory effects on proinflammatory
haled glucocorticoids in patients with mild persistent
signalling pathways, inflammatory mediator release, and
asthma (Sheffer et al. Ann Allergy Asthma Immunol 2005;
recruitment and survival of inflammatory cells. In the pa-
94:48-54). Inhaled glucocorticoids suppress eosinophilic
tient with an airway inflammatory disease such as asthma
inflammation in the airways and are a corner-stone in
or COPD, this is reflected in enhanced anti-inflammatory
asthma treatment (van Rensen et al. Thorax 1999;54:
activity with combination therapy beyond that which can
403-8, Barnes Ernst Schering Res Found Workshop.
be achieved by either drug alone, or the potential for an-
2002; 40:1-23). However, patients show a variable re-
timuscarinic drugs to provide a steroid-sparing effect.
sponse to inhaled glucocorticoids and some exhibit glu-
Cyclic adenosine monophosphate (adenosine
3’,5’-cyclic monophosphate, [cAMP]) is known as a sec-
In COPD the airway inflammation is quite dif-
ond messenger that mediates cellular responses to sev-
ferent from asthma, so inflammation and anti-inflamma-
eral compounds e.g. hormones, mediators, etc. Phos-
tory treatment in COPD is relatively a new focus of inter-
phodiesterases (PDEs) are a family of enzymes that
est. In contrast to asthma, the practice of using inhaled
metabolize 3’,5’ cyclic nucleotides to 5’ nucleoside mono-
glucocorticoids in COPD is common but controversial
phosphates, thereby terminating cAMP and cGMP sec-
(Crapo et al. Eur Respir J Suppl 2003; 41:19s-28s, O’Ri-
ond messenger activity. A particular PDE, PDE4, which
ordan, J Aerosol Med 2003; 16:1-8). It is likely that inhaled
is a high affinity, cAMP specific, type 4 PDE, has gener-
GCs have little effect on the progression of COPD (Vonk
ated interest as potential targets for the development of
et al. Thorax 2003; 58,322-327), glucocorticoids are
novel anti-inflammatory compounds. In fact, PDE4 reg-
probably scarcely effective in COPD patients without
ulate intracellular levels of cAMP and are the predomi-
overlapping concomitant asthma. The use of inhaled glu-
nant PDE expressed in inflammatory cells. Inhibitors of
cocorticoids in patients with moderately severe disease
PDE4 act by increasing intracellular concentrations of
(FEV1 < 50% predicted) may produce clinical benefit as
cyclic AMP, which has a broad range of anti-inflammatory
measured by an increase in FEV1, reduced symptoms
effects on various key effector cells involved in asthma
and fewer exacerbations (O’Riordan, J Aerosol Med
and COPD (Barnette et al. J Pharmacol Exp Ther 1998;
2003; 16:1-8). However, there is also clinical evidence
284:420-6, Hatzelmann and Schudt, J Pharmacol Exp
that the neutrophil inflammation may be decreased by
Ther 2001; 297:267-79, Marx et al. Pulm Pharmacol Ther
inhaled glucocorticoids in clinically stable COPD patients
2002; 15:7-15, Kuss et al. J Pharmacol Exp Ther 2003;
(Yildiz et al. Respiration 2000; 67:71-6). Consequently,
307:373-85). They show a broad spectrum of activity in
in a recently published guideline on COPD treatment,
animal models of asthma COPD (Howell et al. 1995,
adding on inhaled glucocorticoid is recommended in
Bundschuh et al. 2002, Billah et al. 2002, Kuss et al. J
moderate to severe disease (Pauwels et al. Am J Respir
Pharmacol Exp Ther 2003; 307:373-85). In addition, ac-
Crit Care Med 2001; 163:1256-76). glucocorticoids
tivation of the cAMP signalling pathway in airway smooth
should mainly be used to reduce exacerbations and im-
muscle cells promotes relaxation and blocks smooth
EP 1 971 369 B1
muscle cell replication (Tomlinson et al. Biochem Phar-
of drugs, among which can be mentioned for example
macol 1995; 49: 1809-19), thus preventing the airway
triamcinolone, beclomethasone; mometasone, flutica-
remodelling observed in the chronic stage of the diseas-
sone, budesonide, etc., elicits remarkable pharmacody-
es. Studies on cilomilast, roflumilast and other PDE4 in-
namics effects on the respiratory tract. Additionally, they
hibitors in asthma and COPD have shown a broad range
also elicit undesired effects on different organs, and for
of anti-inflammatory activity, and the available evidence
this reason both their clinical use and its interruption
on clinical outcomes (Compton et al. Lancet 2001; 358:
cause a series of side effects, some of which very serious.
265-7, Dyke and Montana, Expert Opin Investig Drugs
Among said toxic effects can be mentioned
2002; 11:1-13, Grootendorst et al. Pulm Pharmacol Ther
those affecting the bone tissue leading to an altered cel-
2003; 16:341-7, Spina Curr Drug Targets Inflamm Allergy
lular metabolism and a high osteoporosis incidence. Sev-
2004; 3:231-6, Lipworth Lancet 2005; 365:167-75,
eral studies showed that inhaled glucocorticoids cause
Bäumer et al. Exp Rev 2005; 1:134-45, Rabe et al. Lancet
a reduction in bone mineral density leading to an increase
2005; 366:563-71). Efforts to minimize or eliminate the
in fractures in people taking an inhaled glucocorticoid
above-mentioned adverse events sometimes associated
compared with controls (Ip et al. Chest 1994; 1051722-7,
with PDE4 inhibitors have included creating inhibitors
Mortimer et al. Ann Allergy Asthma Immunol 2005; 94:
which do not penetrate the central nervous system, and
15-21). Strategies are needed to reduce the systemic
administering PDE4 inhibitors by inhalation rather than
effects of inhaled glucocorticoids. Inhibition of PDE4 ac-
orally. It is likely that these class-associated side effects,
tivity is believed effective for the treatment of osteoporo-
mainly nausea and emesis, could be at least partially
sis by reducing bone loss. There is evidence that the
overcome by the so-called "second-generation" PDE4
PDE4 isoenzyme may play an important role in bone turn-
inhibitors that can be applied by inhalation.
over through cAMP and that its inhibitors are candidates
Inhibition of PDE4 results in an elevation of
for therapeutic drugs for the bone loss diseases (Miya-
cAMP in the inflammatory cells, which in tum downreg-
moto et al. Biochem Pharmacol 1997; 54:613-7). Indeed,
ulates the inflammatory response. For example, rol-
rolipram can enhance physiological bone formation and
ipram, a PDE4 inhibitor, reduced the clinical and histo-
thereby increase bone mass in mice (Kinoshita et al.
logical severity of collagen-induced arthritis in rats (Ny-
Bone 2000; 27:811-7). PDE4 inhibitors are apparently
man U, Mussener A, Larsson E, Lorentzen J, KJareskog
able to counteract the bone-demineralising effect of glu-
L: Amelioration of collage II-induced arthritis in rats by
cocorticoids. Therefore, it would be desirable to provide
the type IV phosphodiesterase inhibitor rolipram.). It has
novel compositions that contain besides glucocorticoids
also been demonstrated that selective PDE4 inhibition
suppresses the clinical manifestations of EAE (Sommer
Current treatments for asthma and COPD are
N, Martin R, McFarland HF, Quigley L, Cannella B, Raine
not satisfactory. Given the high prevalence of these dis-
CS, Scott DE, Loschmann PA, Racke MK. Therapeutic
eases, improved, more effective and more convenient
potential of phosphodiesterase type 4 inhibition in chronic
therapeutic interventions are highly desirable.
autoimmune demyelinating disease. J Neuroimmunol
Therefore the problem underlying the invention
1997;79:54-61). PDE4 inhibitors might also have thera-
was to present a pharmaceutical, which is improved for
peutic benefit both in IBD (Banner KH, Trevethick MA.
the treatment of inflammatory diseases especially respi-
PDE4 inhibition; a novel approach for the treatment of
ratory diseases as asthma or COPD, but also for rheu-
inflammatory bowel disease. Trends Pharmacol Sci
2004;25:430-6), and in psoriasis (Houslay MD, Schafer
This problem is solved by a combination of the
P, Zhang KY. Keynote review: phosphodiesterase-4 as
anticholinergic R,R-glycopyrrolate, the PDE4 inhibitor
a therapeutic target. Drug Discov Today 2005;10:
rolipram and the glucocorticoid budesonide, which show
higher efficiency and reduced side effects compared to
One of the possible side effects induced by
the single substances or double combinations which
PDE4 inhibitors may be a certain sedation, decrease in
could not be expected from prior art.
locomotor activity. In animal experiments, it has convinc-
The combination may be administered as fixed
ingly been demonstrated that rolipram, a specific PDE4
of free combinations, which may be administered simul-
inhibitor induces sedative effects such as hypoactivity,
decreased locomotion that were completely reversed by
The combination may be administered orally,
adding scopolamine, an anticholinergic compound (Sil-
topically, preferably inhalative. In free combination the
vestre et al. Pharmacol Biochem Behav 1999; 64:1-5).
single active substances may be presented in the same
Consequently, an antimuscarinic agents may compen-
or different administration forms, chosen from the possi-
sate the possible sedation induced by a PDE4 inhibitor
bilities of oral, topical, and inhalative application.
and thus improve the therapeutic value of the combina-
It is well known that inhaled glucocorticoids rep-
resent a first choice pharmacological intervention in the
The influence of monocompounds and its com-
therapy of inflammatory respiratory diseases. This class
bination, also in three-in-one on TNF secretion was in-
EP 1 971 369 B1
vestigated by using human monocytes. The study was
The PDE4 inhibitor rolipram dose dependently
approved by our institutional Ethics Committee according
inhibited the TNFα release. Maximum inhibition was
to the International Declarations of Helsinki and Tokyo.
around 70%. Consequently, instead of IC50, the IC35-val-
Peripheral blood mononuclear cells (PBMCs)
ue was determined. The IC35 for rolipram amounted to
were isolated from heparinized blood samples of healthy
donors by density gradient centrifugation. An equal vol-
The corticosteroid budesonide also inhibited
ume of Hanks buffer (Invitrogen, Heidelberg, Germany)
the TNFα release in a dose-dependent manner. The IC50
was added to heparinized whole blood samples. 15ml
Histopaque-1077 (Sigma, Deisenhofen, Germany) were
overlayed with a maximum of 40ml of blood/Hanks mix-
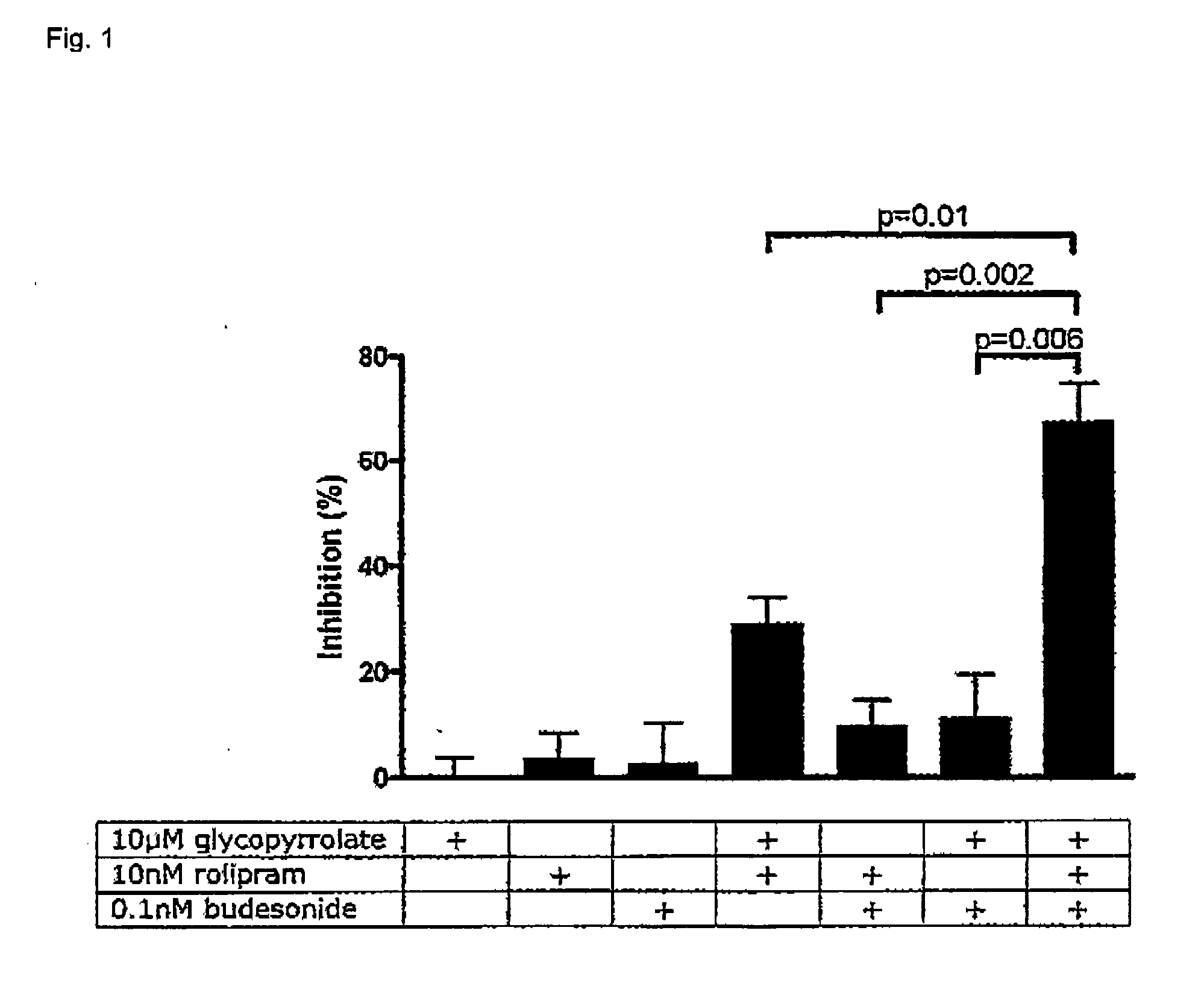
substances , in a first experiment the effect of the PDE4
ture and were centrifuged for 30 min at room temperature
inhibitor rolipram (10 nM) and the corticosteroid budes-
(2000 rpm). A visible band containing PBMCs was trans-
onide (0.1 nM) alone and in combination, and in combi-
ferred to a fresh tube and washed twice with Hanks-buff-
nation with R,R-glycopyrrolate (10 PM) on the LPS-in-
er. Finally cells are seeded in RPMI 1640 Medium (Life
duced TNFα release from human PBMCs was investi-
Technologies, Heidelberg, Germany) with Glutamax I
gated. The concentrations chosen for rolipram and
(Gibco BRL, Eggenstein) and 10% FCS (Boehringer
budesonide were considerably below their IC35 and IC50,
Mannheim, Penzberg, Germany). After isolated, PBMCs
respectively. The results are summarized in Fig. 1.
were seeded in RPMI 1640 medium (Invitrogen, Heidel-
ThePDE4 inhibitor rolipram dose dependently
berg, Germnay) with Glutamax I (Invitrogen, Heidelberg,
inhibited the TNFα release. Maximum inhibition was
Germany). PBMCs were cultured in RPMI 1640 medium
around 70%. Consequently, instead of IC50, the IC35-val-
at 37 °C 5% CO2 overnight. Monocytes were isolated
ue was determined. The IC35 for rolipram amounted to
from other cells by adherence method, non-adherent
cells were removed by changing the medium.
The corticosteroid budesonide also inhibited
Cells were re-suspended at 106 cells/ml and
the TNFα release in a dose-dependent manner. The IC50
incubated in 500Pl volumes in 24-well tissue culture
plates (Falcon Becton Dickinson Labware, Heidelberg,
Based on the results from the single substanc-
Germany) at 37°C, 5%CO2. After pre-incubation with test
es, the effect of the PDE4 inhibitor rolipram (10 nM) and
substances (0.5 Pl / 500Pl medium) for 30min, cells were
the corticosteroid budesonide (0.1 nM) alone and in com-
stimulated with lipopolysaccharide (LPS) (Sigma, De-
bination, and in combination with R,R-glycopyrrolate (10
isenhofen, Germany) (1 Pg/ml). After 24 h of incubation,
PM) on the LPS-induced TNFα release from human PB-
cells were sedimented by centrifugation. The superna-
MCs was investigated. The concentrations chosen for
tants were harvested and kept frozen at -80°C until pro-
rolipram and budesonide were considerably below their
IC35 and IC50, respectively. The results are summarized
Cytokine measurements in culture superna-
tants were done by sandwich ELISA using matched an-
As can be seen from Fig. 1, each drug alone
tibody pairs (BD Pharmingen, Heidelberg, Germany).
hardly affected LPS-induced TNFα release. At the inten-
ELISA plates (Maxisorb, Nunc, Wiesbaden, Germany)
tionally low concentrations, each double combination
were coated overnight with anti-cytokine monoclonal an-
caused only a minor inhibition of TNFα secretion from
tibody (mAb) in 0.1 M carbonate buffer, pH 9.5. After
PBMCs. In contrast, the three-in-one combination
being washed, plates were blocked with Assay Diluent
(budesonide, rolipram and R,R-glycopyrrolate) resulted
(BD Pharmingen, Heidelberg, Germany) for 1h and
in statistically significant over-additive inhibition of the
washed again. Appropriately diluted supernatant sam-
ples and standards were distributed in duplicates and the
The medications can be administered in differ-
plates were incubated for 2h at room temperature. Plates
ent ways, such as metered-dosage inhalers (MDls), in
were washed, incubated for 1h with working detector (bi-
dry powder inhalers (DPls), and in another liquid formu-
otinylated anti-cytokine antibody and Avidin-horseradish
lation suitable for inhalation. They can also be adminis-
peroxidase conjugate) (BD Pharmingen, Heidelberg,
tered together in a single dosage form. Or they may be
Germany). After washing, substrate (TMB and hydrogen
administered in different dosage forms. They may be ad-
peroxide) was added. The reaction was stopped by add-
ministered at the same time. Or they may be administered
ing of 1 M H3PO4- Plates were read at 450nm (reference
either close in time or remotely, such as where one is
570nm) in a microplate reader (Dynatech, Alexandria,
administered in the morning and the second is adminis-
USA). The results were expressed as a percentage of
tered in the evening. The combination may be used pro-
the control level of cytokines production by cells stimu-
phylactically or after the onset of symptoms has occurred.
lated in the absence of the compound.
In some instances the combination(s) may be used to
Upon LPS-stimulation, basal TNFα release
prevent the progression of a pulmonary disease or to
from monocytes increased from 328 pg/ml up to 7,258
arrest the decline of a function such as lung function.
pg/ml. R,R-glycopyrrolate alone did not influence the
These drugs are usually administered as an
LPS-induced TNFα release up to 10 Pmol/l.
aerosol, or as an inhaled powder. This invention contem-
EP 1 971 369 B1
plates either co-administering all drugs in one delivery
substance optionally together with a finely divided phar-
form such as an inhaler that is putting all drugs in the
maceutically acceptable carrier, which is preferably
present and may be chosen from materials known as
As inhalable compositions pressurized me-
carriers in dry powder inhalation compositions, for exam-
tered dose inhalers, dry powders or inhalation solutions
ple saccharides, including monosaccharides, disaccha-
without propellant can be considered. Among the latter
rides, polysaccharides and sugar alcohols such as ara-
are even sterile, ready for use or just before use manu-
binose, fructose, ribose, mannose, sucrose, trehalose,
factured inhalation solutions, suspensions or concen-
lactose, starches, dextran or mannitol. An especially pre-
trates as a nebulizable composition in an aqueous and/
ferred carrier is lactose. The dry powder may be in cap-
or organic medium. These dosage forms are part of the
sules of gelatin or plastic, or in blisters, for in a dry powder
inhalation device. Alternatively, the dry powder may be
Pressurized metered dose inhalers with propel-
contained as a reservoir in a dose dry powder inhalation
lants may contain the active substances in solution or in
dispersion in a propellant. The propellants which can be
The inhalation powders according to this inven-
used for inhalation aerosols in this invention are well
tion can be administered by the help of state of the art
known: mainly halogenated hydrocarbon derivatives,
dry powder inhalation devices for instance the Novoliz-
TG134a and TG227, or their mixtures are applied. Fur-
er®. The inhalation powder can be pre-metered in cap-
thermore detergents (eg. oleic acid), stabilizers (eg. so-
sules (eg. gelatine) or blisters (aluminium pouches) or
dium edetate), co-solvents (eg. propyleneglycol, polyeth-
metered just before use from a bulk reservoir. The active
yleneglycol, glycerol), antioxidants (eg. ascorbic acid),
substances of the inventive combination can be there in
lubricants (eg. polyoxyethylene-glyceryl-trioleate) or
a fixed combination or both actives are in separate pack-
buffer systems or other excipients for pH adjustment (eg.
aging units, that they can be administered independent
hydrochloric acid) are normally added. The active ingre-
of each other from one device or a pack from two or more
dient may have an average particle diameter of up to 5
different devices or simultaneously.
In the finely divided particulate form of the med-
A combination of ethyl alcohol and poly-oxyeth-
icament, and in the aerosol composition where the active
ylene-25-glyceryl-trioleate (trade name: Tagat TO) can
ingredient is present in particulate form, the active ingre-
be suitable used as a detergent/stabilizer/co-solvent/lu-
dient may have an average particle diameter of up to 4
bricant complex in a concentration between 0.5 and 1.5
Pm. The finely divided carrier, where present, generally
has a maximum diameter up to approximately 500 Pm
The above mentioned aerosols containing a
and conveniently has a mean particle diameter of 10 to
propellant, solutions or suspensions according to the in-
350 Pm, preferably approx. 110 to 290 Pm. The particle
vention are administered by state of the art inhalers, so-
size of the active ingredient, and that of the carrier where
called pressurized metered dose inhalers (=pMDI). They
present in dry powder compositions, can be reduced to
can be equipped with different-sized metal or plastic
the desired level by conventional methods, for example
stems, responsible for metering and release of the ac-
by grinding in an air-jet mill, ball mill or vibrator mill, mi-
croprecipitation, spray-drying, lyophilisation or recrystal-
Administration of the medicament or pharma-
ceutical composition is preferably by inhalation. The in-
The active ingredients may be given from 1 to
halable form of the medicament may be, for example, an
8 times a day, sufficient to exhibit the desired activity.
atomizable composition such as an aerosol comprising
Preferably, the active components are given about once
the active ingredients, separately or in admixture, in so-
or four times a day, more preferably once or twice a day.
lution or dispersion in a propellant, or a nebulizable com-
The inhaled anticholinergic drug, R,R-glycop-
position comprising a dispersion of the active ingredient
yrrolate can be administered in an amount of between 5
in an aqueous/organic or medium. For example, the in-
and 500 Pg/day adult human with the preference of 15
halable form of the medicament may be an aerosol com-
prising a mixture of any composition according to the
The PDE4 inhibitor rolipram can be adminis-
invention in solution or dispersion in a propellant, or a
tered in an amount between 10 and 5000 Pg/day adult
combination of an aerosol containing each single active
human with the preference of 50 to 2000 Pg/day in de-
substance in solution or dispersion in a propellant. In an-
pendence of the intensity of the airway inflammation.
other example, the inhalable form is a nebulized compo-
The glucocorticoid budesonide can be admin-
sition comprising a dispersion of the substances accord-
istered in an amount of between 50 and 2000 Pg/day
ing to the inventive combination in an aqueous or organic
adult human with the preference of 100 to 1000 mg/day
medium, or a combination of dispersions of each sub-
in dependence of the intensity of the airway inflammation.
The active ingredients in all above aerosol for-
In another embodiment of the invention, the in-
mulations are preferably in the concentration of 0.01 wt%
halable form is a dry powder, i.e. the substances are
present in a dry powder comprising finely divided each
The anticholinergic drug, R,R-glycopyrrolate
EP 1 971 369 B1
can be administered in an amount between 1 and 199
ment of inflammatory diseases selected form the
mg/day for adult patients with the preference of 5 to 50
group comprising respiratory diseases, rheumatism
10. Use according to claim 9, characterized in that the
It is contemplated that all active agents would
respiratory disease is asthma or COPD.
be administered at the same time, or very close in time. Alternatively, one drug could be taken in the morning and
11. Use according to claim 9, characterized in that the
others later in the day. Or in another scenario, one drug
auto-immune disease is rheumatoid arthritis,
could be taken twice daily and the others once daily, ei-
glomerulonephritis, multiple sclerosis, Crohn’s dis-
ther at the same time as one of the twice-a-day dosing
ease, ulcerative colitis, systemic lupus erythemato-
occurred, or separately. Preferably all drugs would be
Patentansprüche
Kombination von R,R-Glykopyrrolat, Rolipram und
Combination of R,R-glycopyrrolate, rolipram and
Budesonid oder ihren physiologisch unbedenklichen
budesonide or their physiologically acceptable salts
Salzen zur Verwendung bei der Behandlung von ent-
for use in the treatment of inflammatory diseases.
Combination according to claim 1, characterized in
Kombination nach Anspruch 1, dadurch gekenn- that the inflammatory disease is a respiratory dis- zeichnet, daß es sich bei der entzündlichen Erkran-
ease, rheumatism or an auto-immune disease.
kung um eine Atemwegserkrankung, Rheumatis-
mus oder eine Autoimmunkrankheit handelt.
Combination according to claim 2, characterized in that the respiratory disease is asthma or COPD.
Kombination nach Anspruch 2, dadurch gekenn- zeichnet, daß es sich bei der Atemwegserkrankung
Combination according to claim 2, characterized in that the auto-immune disease is rheumatoid arthri- tis, glomerulonephritis, multiple sclerosis, Crohn’s
Kombination nach Anspruch 2, dadurch gekenn-
disease, ulcerative colitis, systemic lupus erythema-
zeichnet, daß es sich bei der Autoimmunkrankheit
um rheumatoide Arthritis, Glomerulonephritis, mul-tiple Sklerose, Morbus Crohn, Colitis ulcerosa, sy-
Pharmaceutical for use in the treatment of inflamma-
stemischen Lupus erythematodes oder Psoriasis
tory diseases containing R,R-glycopyrrolate, rol-
ipram and budesonide or their physiologically ac-ceptable salts
Pharmazeutikum zur Verwendung bei der Behand-lung von entzündlichen Erkrankungen, enthaltend R,
Pharmaceutical according to claim 5, characterized
R-Glykopyrrolat, Rolipram und Budesonid oder ihre
in that it is an inhalable dry powder, an inhalable
aerosol with or without propellant, or an inhalablesuspension or solution.
Pharmazeutikum nach Anspruch 5, dadurch ge- kennzeichnet, daß es sich um ein inhalierbares
Pharmaceutical according to claim 6, presented in
Trockenpulver, ein inhalierbares Aerosol mit oder
ohne Treibmittel oder eine inhalierbare Suspensionoder Lösung handelt.
Pharmaceutical according to any one of claims 5 to 7, characterized in that the active substances are
Pharmazeutikum nach Anspruch 6, das in einem In-
presented in fixed or free combination for simultane-
ous, sequential or separate administration togetherwith the usual excipients, adjuncts, and additives in
Pharmazeutikum nach einem der Ansprüche 5 bis
a pharmaceutical form suitable for inhalative appli-
7, dadurch gekennzeichnet, daß die Wirkstoffe in
fester oder freier Kombination für die gleichzeitige,
aufeinanderfolgende oder getrennte Verabreichung
Use of a combination of R,R-glycopyrrolate, rolipram
zusammen mit herkömmlichen Exzipienten, Adju-
and budesonide or their physiologically acceptable
vantien und Zusatzstoffen in einer für die inhalative
salts for the production of a medicament for the treat-
Anwendung geeigneten pharmazeutischen Form
EP 1 971 369 B1
Produit pharmaceutique selon l’une quelconque des revendications 5 à 7, caractérisé en ce que les
Verwendung einer Kombination von R,R-Glykopyr-
substances actives sont présentées dans une com-
rolat, Rolipram und Budesonid oder ihren physiolo-
binaison fixe ou libre pour une administration simul-
gisch unbedenklichen Salzen zur Herstellung eines
tanée, séquentielle ou séparée conjointement avec
Medikaments zur Behandlung von entzündlichen Er-
les excipients, les adjuvants et les additifs habituels
krankungen, ausgewählt aus der Atemwegserkran-
sous une forme pharmaceutique appropriée pour
kungen, Rheumatismus oder Autoimmunkrankhei-
Utilisation d’une combinaison de R,R-glycopyrrola-
10. Verwendung nach Anspruch 9, dadurch gekenn-
te, de rolipram et de budésonide ou de leurs sels
zeichnet, daß es sich bei der Atemwegserkrankung
physiologiquement acceptables pour la production
d’un médicament pour le traitement de maladies in-flammatoires choisies parmi le groupe constitué de
11. Verwendung nach Anspruch 9, dadurch gekenn-
maladies respiratoires, de rhumatismes ou de ma-
zeichnet, daß es sich bei der Autoimmunkrankheit
um rheumatoide Arthritis, Glomerulonephritis, mul-tiple Sklerose, Morbus Crohn, Colitis ulcerosa, sy-
10. Utilisation selon la revendication 9, caractérisée en
stemischen Lupus erythematodes oder Psoriasis
ce que la maladie respiratoire est l’asthme ou la 11. Utilisation selon la revendication 9, caractérisée en Revendications ce que la maladie auto-immune est la polyarthrite rhumatoïde, la sclérose en plaques, la maladie de
Combinaison de R,R-glycopyrrolate, de rolipram et
Crohn, la colite ulcéreuse, le lupus érythémateux dis-
de budésonide ou de leurs sels physiologiquement
acceptables pour utilisation dans le traitement demaladies inflammatoires.
Combinaison selon la revendication 1, caractérisée en ce que la maladie inflammatoire est une maladie respiratoire, un rhumatisme ou une maladie auto- immune.
Combinaison selon la revendication 2, caractérisée en ce que la maladie respiratoire est l’asthme ou la MPOC.
Combinaison selon la revendication 2, caractérisée en ce que la maladie auto-immune est la polyarthrite rhumatoïde, la sclérose en plaques, la maladie de Crohn, la colite ulcéreuse, le lupus érythémateux dis- séminé ou le psoriasis.
Produit pharmaceutique pour utilisation dans le trai-tement de maladies inflammatoires, qui contient duR,R-glycopyrrolate, du rolipram et du budésonide ouleurs sels physiologiquement acceptables.
Produit pharmaceutique selon la revendication 5, caractérisé en ce qu’il s’agit d’une poudre sèche inhalable, d’un aérosol inhalable avec ou sans pro- pulseur, ou une suspension ou une solution inhala- ble.
Produit pharmaceutique selon la revendication 6,présenté sous la forme d’un inhalateur. EP 1 971 369 B1 EP 1 971 369 B1 REFERENCES CITED IN THE DESCRIPTION
This list of references cited by the applicant is for the reader’s convenience only. It does not form part of the Europeanpatent document. Even though great care has been taken in compiling the references, errors or omissions cannot beexcluded and the EPO disclaims all liability in this regard. Non-patent literature cited in the description Saetta et al. Am J Respir Crit Care Med, 1999, vol. Nishimura et al. Chest, 1999, vol. 115, 31-7 [0032]
160, 711-7 [0004] Selroos. Curr Med Res Opin, 2004, vol. 20, 1579-93 Shapiro. Am J Respir Crit Care Med, 1999, vol. 160,
S29-S32 [0004] Adcock ;Chung. Curr Opin Investig Drugs, 2002, Yamamoto et al. Chest, 1997, vol. 112, 505-10
vol. 3, 58-60 [0032] Calverley et al. Eur Respir J, 2003, vol. 22, 912-9 Keatings et al. Am J Respir Crit Care Med, 1996,
vol. 153, 530-4 [0007] Calverley. Semin Respir Crit Care Med, 2005, vol. Rodrigo ;Rodrigo. Chest, 2003, vol. 123, 1908-15
26, 235-45 [0032] Calverley. Semin Respir Crit Care Med, 2005, Hansel ;Bames. Drugs Today, 2002, vol. 38,
26235-45 [0032]
585-600 [0011] Rascati et al. Clin Ther, 2005, vol. 27, 346-54 [0033] Koumis ;Samuel. Clin Ther, 2005, vol. 27, 377-92 Barnette et al. J Pharmacol Exp Ther, 1998, vol.
284, 420-6 [0034] Barr et al. Cochrane Database Syst Rev, 2005, Hatzelmann ;Schudt. J Pharmacol Exp Ther, 2001,
CD002876 [0011]
vol. 297, 267-79 [0034] Jacobson DL ;Grange SJ ;Rose NR ;Graham Marx et al. Pulm Pharmacol Ther, 2002, vol. 15, 7-15 NM. Clin Immunol Immunopathol, 1997, vol. 84,
223-43 [0013] Kuss et al. J Pharmacol Exp Ther, 2003, vol. 307, Calverley et al. Thorax, 2003, vol. 58, 855-60 [0028]
373-85 [0034] [0034] Caramori ;Adcock. Pulm Pharmacol Ther, 2003, Tomlinson et al. Biochem Pharmacol, 1995, vol. 49,
vol. 16, 247-77 [0028]
1809-19 [0034] Ali-Melkkila et al. Acta Anaesthesiol Scand, 1993, Compton et al. Lancet, 2001, vol. 358, 265-7 [0034]
vol. 37, 633-42 [0029] Dyke ;Montana. Expert Opin Investig Drugs, 2002, Haddad et al. Br J Pharmacol, 1999, vol. 127, 413-20
vol. 11, 1-13 [0034] Grootendorst et al. Pulm Pharmacol Ther, 2003, Walker et al. Chest, 1987, vol. 91, 49-51 [0029]
vol. 16, 341-7 [0034] Schroeckenstein et al. J Allergy Clin Immunol, Spina. Curr Drug Targets Inflamm Allergy, 2004, vol.
1988, vol. 82, 115-9 [0029]
3, 231-6 [0034] Gilman et al. Chest, 1990, vol. 98, 1095-8 [0029] Lipworth. Lancet, 2005, vol. 365, 167-75 [0034] Cydulka ;Emerman. Ann Emerg Med, 1995, vol. Bäumer et al. Exp Rev, 2005, vol. 1, 134-45 [0034]
25, 470-3 [0029] Rabe et al. Lancet, 2005, vol. 366, 563-71 [0034] Hansel et al. Chest, 2005, vol. 128, 1974-9 [0029] Sommer N ;Martin R ;McFarland HF ;Quigley L ;
Barnes Ernst Sobering Res Found Workshop, 2002,
Cannella B ;Raine CS ;Scott DE ;Loschmann
vol. 40, 1-23 [0031] PA ;Racke MK. Therapeutic potential of phosphodi- Sheffer et al. Ann Allergy Asthma Immunol, 2005,
esterase type 4 inhibition in chronic autoimmune de-
vol. 94, 48-54 [0031]
myelinating disease. J Neuroimmunol, 1997, vol. 79,
van Rensen et al. Thorax, 1999, vol. 54, 403-8
54-61 [0035] Banner KH ;Trevethick MA. PDE4 inhibition; a nov-
Barnes Ernst Schering Res Found Workshop, 2002,
el approach for the treatment of inflammatory bowel
vol. 40, 1-23 [0031]
disease. Trends Pharmacol Sci, 2004, vol. 25, 430-6
Crapo et al. Eur Respir J Suppl, 2003, vol. 41,
19s-28s [0032] Houslay MD ;Schafer P ;Zhang KY. Keynote re- O’Riordan. J Aerosol Med, 2003, vol. 16, 1-8 [0032]
view: phosphodiesterase-4 as a therapeutic target.
Drug Discov Today, 2005, vol. 10, 1503-19 [0035] Vonk et al. Thorax, 2003, vol. 58, 322-327 [0032] Silvestre et al. Pharmacol Biochem Behav, 1999, Yildiz et al. Respiration, 2000, vol. 67, 71-6 [0032]
vol. 64, 1-5 [0036] Pauwels et al. Am J Respir Crit Care Med, 2001, Ip et al. Chest, 1994, 1051722-7 [0038]
vol. 163, 1256-76 [0032] EP 1 971 369 B1 Mortimer et al. Ann Allergy Asthma Immunol, 2005, Miyamoto et al. Biochem Pharmacol, 1997, vol. 54,
vol. 94, 15-21 [0038]
613-7 [0038] Kinoshita et al. Bone, 2000, vol. 27, 811-7 [0038]
RANIDE FORTE ® FICHA TÉCNICA USO VETERINARIO 1.- GENERALIDADES: : RANIDE FORTE 2.- PROPIEDADES FÍSICO-QUÍMICAS: : Estable durante 2 años a partir de la fecha de elaboración en condiciones normales de almacenamiento. 3.-DESCRIPCIÓN: Antiparasitario interno en suspensión oral de 4.- INDICACIONES: RANIDE FORTE está indicado para el control y tr
Reversal of Polarity, Cyclizations, Summary of Strategies B. Important Reactions used in WW Chapter 7: Model: Synthesis of 1,2-DiX electrophiles meta -chloroperbenzoic acid (MCPBA) meta -chloroperbenzoic acid (MCPBA) Exploration: The products in reactions a-e are starting materials revealed in the 2-Group Di-X activity. Now we are exploring how they can be synthesized and the natu
 EP 1 971 369 B1
EP 1 971 369 B1