Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Hrup643 201.215
Human Reproduction Update, Vol.8, No.3 pp. 201±215, 2002
Hormone replacement therapy and the prevention of
Helena J.TeedeAddress for correspondence: Monash University Department of Medicine, Vascular Medicine and Sciences Unit, Dandenong
Hospital, David St, Dandenong 3175, Victoria, Australia. E-mail: [email protected]
Cardiovascular disease (CVD) is the primary killer of both men and women in Western societies. The
implementation of preventive strategies has led to a fall in the rate of CVD, but there is still much to be
achieved. Proven interventional strategies are largely under-utilized, and the search continues for further promising
interventions. HRT appears to reduce CVD in post-menopausal women, based on observational data supported by
plethora of evidence for the bene®cial cardiovascular effects of estrogen. However, a recent controlled trial in post-
menopausal women with established CVD has shown that a speci®c combined oral HRT regimen did not reduce, and
may even contribute to, an early increase in cardiovascular events, suggesting that HRT is inappropriate in
secondary prevention. HRT may be useful in the primary prevention of CVD, yet observational data that suggested
cardiovascular bene®t with HRT also suggests that 80% of CVD in women could be eliminated by lifestyle
modi®cation, without the attendant risks of HRT including thrombosis and (potentially) breast cancer. At present, it
is arguable that the evidence is inadequate to recommend HRT solely for the purpose of CVD prevention, and that
the challenge for the health professional should be appropriate utilization of established preventative therapies, with
further research into the potential role of HRT and estrogen-receptor modulators.
Key words: cardiovascular disease/health management/hormone replacement therapy/lifestyle modi®cation/preventative therapy
Lifestyle modi®cations are well known to reduce CVD with
few side effects and many other health bene®ts. Many
pharmacological interventions including anti-platelet, anti-hyper-
Cardiovascular disease in women, and established risk factors
tensive and lipid-lowering therapies also reduce cardiovascular
morbidity and mortality (Yusef, 1998). Increasing evidence
suggests that the targets for cardiovascular risk factor reduction
should be more aggressive. Yet it appears that even existing
Randomized controlled human interventional data
targets are not being met (Mosca et al., 1999; Wood, and the Joint
European Task Force, 2001). The recent American Heart
Association guidelines on preventive cardiology noted that
clinicians are missing opportunities for prevention, and that this
is especially the case in women (Mosca et al., 1999).
Women spend on average 35 years of their lives in a post-
menopausal, low-estrogen state. It is during these years that the
majority of CVD burden is noted. In this setting, hormone
Cardiovascular disease (CVD) is the number one killer in both
replacement therapy (HRT) may have a role to play in the
men and women in Western society. The disease process is
prevention of CVD. There is overwhelming observational data to
largely attributed to age and lifestyle factors (Stampfer et al.,
support a bene®cial effect of HRT on the cardiovascular system.
2000). Effective health management strategies, if appropriately
There are, however, limitations in the application of observational
implemented, have the potential for signi®cant impact on both
data to the clinical setting. A wealth of animal and human
mortality and morbidity. With the emphasis on evidence-based
interventional data, focusing on isolated mechanisms of estrogen
medicine, the ef®cacy of preventive measures has been proven in
action, has suggested largely bene®cial cardiovascular effects.
numerous well-designed trials (Yusef, 1998). As a result, the
Yet, the translation of animal data to the post-menopausal woman
implementation of these preventive measures has resulted in a
may not be valid. Furthermore, the in-vivo effects of estrogen are
recent fall in the incidence of CVD (Hu et al., 2000).
ubiquitous and complex. In this setting it is the net effects of
Ó European Society of Human Reproduction and Embryology
estrogen rather than isolated estrogenic mechanisms that are most
progression to diabetes, in those with impaired glucose tolerance
relevant clinically (Teede and McGrath, 1999). This can only be
(Hu et al., 2000, 2001; Tuomilehto et al., 2001). Unfortunately,
assessed in controlled human trials focusing on de®nitive clinical
obesity is increasing in Western societies, and may be slowing the
end-points. In limited controlled data completed to date, the
decline in CVD (Hu et al., 2000). This is likely to be contributed
effects of HRT appear to be neutral or even deleterious (Hulley et
to by the sedentary nature of Western lifestyle. Although evidence
al., 1998). Estrogen actions depend on dose, type, route of
is largely observational, the role of exercise in the prevention of
administration and on the co-administered progestin. Therefore,
CVD is also well accepted. The National Heart Foundation of
even the results of controlled trials should be interpreted only for
Australia and the American Heart Association recognize physical
the speci®c HRT preparations used and the populations studied.
inactivity as an independent risk factor, and recommend 30
In considering the potential role for HRT in CVD prevention,
minutes of moderate intensity exercise ®ve times per week. Few
clinicians need to appreciate the dif®culties in translating existing
people achieve these targets, however (Glassberg and Balady,
data on the vascular effects of HRT into clinical practice. There is
also a need to interpret all results in the era of evidence-based
Improving lipid pro®les in those with established CVD has
medicine and in the setting of inadequate utilization of existing
been shown to lead to regression of atherosclerosis and markedly
proven preventive therapies (Burger and Teede 2001; Mosca et
to reduce cardiovascular events (Ades, 2001). In women, low
al., 2001a; Wood, and the Joint European Task Force, 2001).
serum high-density lipoprotein (HDL) and raised triglycerides
Future research is essential to resolve many important issues prior
appear more important than low-density lipoprotein (LDL) levels
to establishing de®nitively the role of HRT and other estrogenic
alone. However, lipid-lowering trials have demonstrated that
high-risk women bene®t from LDL lowering with statins, for both
primary and secondary prevention, as much as men (Heart
Cardiovascular disease in women, and established risk
Protection Study Collaboration Group, 2001). Improvement in
lipid pro®les is achievable through dietary modi®cation, exercise
and drug therapy; the latter approach has been proven to be
Coronary heart disease is the leading cause of mortality, and
especially effective. In the secondary prevention `4S' trial
contributes to signi®cant morbidity among women in western
(Scandinavian Simvastatin Survival Study Group, 1994), cardio-
society (Mosca et al., 1999; Tsang et al., 2000). In fact, in women
vascular events were reduced with statins by 30%. In the
it causes more deaths than the next 14 most common fatal
conditions combined (Tsang et al., 2000). It has been estimated
secondary prevention `CARE' trial, even those with lower LDL
from the prospective Nurses Health Study that the majority of
serum levels had a 24% reduction in coronary events (Sacks et al.,
CVD is preventable by modi®cation in lifestyle (Stampfer et al.,
1996). In those with low HDL levels, treatment with ®brates
2000), and comprehensive risk reduction is a well-established
resulted in a 22% reduction in relative risk of non-fatal
approach to prevent the condition. Proven preventive strategies
myocardial infarction (Rubins et al., 1999). Despite the ef®cacy
encompass exercise, nutritional modi®cation, weight loss and
of these intervention strategies, recent data have suggested that
cessation of smoking, all of which carry no health risks (Ades,
the ideal cholesterol targets are reached in only one-third of
2001). Additional bene®cial strategies include targeted therapy to
patients with coronary disease (Ades, 2001).
reduce blood pressure, improve lipid pro®les, control diabetes,
Intensive blood pressure control is well established for the
reduce platelet adhesion and modulate the neurohumoral system
primary and secondary prevention of cardiovascular disease. The
(Scandanavian Simvastatin Survival Study Group, 1994;
`HOT' study noted that the lower the blood pressure, the lower the
Hennekens et al., 1997; Anonymous, 1998; Hansson et al.,
risk of vascular events (Hansson et al., 1998). The targets for
1998; Progress Collaborative Group, 2001).
optimal blood pressure control are being lowered progressively.
Cessation of smoking is associated with a reduction in coronary
Currently, blood pressures of <140/90 mmHg are being
events. In subjects who have suffered a myocardial infarction, a
recommended, with <130/85 mmHg in high-risk groups (World
50% reduction in mortality and reinfarction rate has been noted
Health Organization, 1999). However, despite the overwhelming
one year after cessation (Wilson et al., 2000). Public health
evidence for blood pressure lowering, the accepted targets are not
campaigns aimed at smoking cessation have been successful; for
being met in the majority of subjects (Wood, and the European
example, in Australia intensive public health measures have led to
a decline in smoking rates down to 20% of the population, though
Diabetes is an important risk factor in women, with the risk of
further effort is still required to minimize the impact of smoking
CVD increased 3- to 7-fold compared with 2- to 3-fold in men.
The Nurses Health Study suggested that diabetic women have a 5-
Adherence to a healthy diet, weight loss and dietary change
fold increase in coronary heart disease compared with non-
including modi®cation in dietary fat intake appear to have
diabetic women (Manson et al., 1991). Diabetic women have
substantial bene®ts in CVD prevention (Stampfer et al., 2000;
more severe CVD, higher CVD-related mortality and poorer
Hooper et al., 2001; Tuomilehto et al., 2001). In a recent
prognosis overall compared with non-diabetic women (Lowel et
Cochrane Database Systematic Review focusing on the cardio-
al., 2000; Friday, 2001). Although blood glucose control may play
vascular effects of dietary fat modi®cation, it was noted that
a role in the prevention of CVD (Anonymous, 1998), it is
dietary intervention for more than 2 years showed signi®cant
accepted that, in diabetic subjects, it is the other risk factors which
reductions in the rate of cardiovascular events (Hooper et al.,
largely contribute to the burden of macrovascular disease (Friday,
2001). Dietary intervention appears to improve lipid pro®les,
2001). Thus, the presence of diabetes should target this high-risk
lower blood pressure, reduce insulin resistance and slow
population for aggressive preventive therapy.
Other important interventions that have a well-established role
Progestins regulate the growth, differentiation and function
in the secondary prevention of CVD include aspirin therapy (ISIS
of target tissues primarily within the reproductive system.
Collaborative Group, 1988; Gaziano et al., 2000). Inadequate
Progesterone is produced primarily by the dominant follicles
utilization is still problematic however (Rogers et al., 1994;
following ovulation, with levels falling signi®cantly once the
Hennekens et al., 1997), as even in study settings such as the
ovarian follicle pool is deplete and menopause occurs (Teede and
secondary prevention `HERS' study, only 78% of women with
Burger, 1998). In post-menopausal women, progestins are used
established CVD received aspirin therapy (Hulley et al., 1998).
therapeutically to oppose the proliferative effects of estrogens on
Neurohormonal modulation of the cardiovascular system with
the endometrium and protect against endometrial malignancy
beta blockade and angiotensin-converting enzyme inhibitors has
(Beresford et al., 1997). Progesterone is the only natural form, but
also been shown to have a role in the prevention of CVD
its therapeutic use is limited by reduced oral bioavailability. The
(Hjalmarson et al., 1981; Progress Collaborative Group, 2001).
majority of therapeutic progestins are therefore synthetic
Despite the established ef®cacy of these strategies, smoking
progestins; these are subdivided into those related structurally to
rates are declining more slowly in women, obesity is increasing,
either progesterone or testosterone (Whitehead, 1994). The
and physical inactivity is escalating. In the USA, 50% of women
different synthetic progestins also have variable pharmacokinetics
aged >45 years have hypertension, and 40% aged >55 years have
and biological activity with additional complex and diverse
elevated cholesterol (Mosca et al., 1999). The under-utilization of
effects outside the reproductive system.
preventive strategies may be related to women's misconceptions
that they are more likely to die of breast cancer, or that heart
Mechanisms of action: estrogen receptors (ER) and progesterone
disease predominantly affects males (Giardina, 2000; Mosca et
al., 2000). This highlights the need for further public health
ER and PR are members of a superfamily of related proteins that
measures and education. The attitude and role of the health
mediate the nuclear effects of steroid hormones (Baysal and
professional is pivotal in the promotion of both appropriate
Losordo, 1996; Mendelsohn and Karas, 1999). These intracellular
prevention strategies and treatments for established CVD. Current
receptors function as ligand-activated transcriptional factors,
evidence suggests that neither prevention nor treatment is
regulating the synthesis of speci®c RNAs and proteins (Baysal
optimal, especially in women (Rosano et al., 1993; Mosca et
and Losordo, 1996). They are characterized by a large and
complex ligand-binding domain, a DNA-binding domain (which
is highly conserved) and a hypervariable regionÐthe amino-
terminal region (Katzenellenbogen, 1996).
Estrogen actions are largely mediated by the ER, although non-
Observational studies have long suggested that in post-menopau-
genomic effects have been documented (Mendelsohn and Karas,
sal women, estrogen combined with progestin may have a role in
1999). The diversity of action of different estrogenic compounds
the prevention of CVD (Wolf et al., 1991; Grady et al., 1992;
or ligands can be attributed to the complex ER system. Estrogenic
Grodstein and Stampfer, 1995). These observations have been
receptor activity is not dependent on steroidal con®gurations
supported by interventional studies focusing on the isolated
(Davies, 1998; Stanczyk, 1998), with both steroidal and non-
mechanisms of sex steroid action within the vasculature. These
steroidal compounds having estrogenic activity. Binding af®nity
mechanisms are ubiquitous and are affected by the dose, type and
does not directly translate to functional estrogenic activity, so the
route of administered estrogen, as well as the co-administered
true `biological estrogenicity' of a compound cannot be studied
progestin. Appropriate interpretation of the vascular effects of
directly (Kuiper et al., 1998; Anderson, 2000). This complexity of
HRT requires an appreciation of the diversity and complexity of
the system re¯ects many factors including the subtype and
distribution of the ER (Kuiper et al., 1997; Makela et al., 1999;
Mendelsohn and Karas, 1999). There are two known ER isoforms,
ERa and ERb (Kuiper et al., 1997). ERs combined with different
Estrogens regulate the growth, differentiation and function of
estrogenic compounds can have different ligand-dependent
diverse target tissues, both within and outside the reproductive
conformational changes. This is by virtue of the ER subtype,
system. There are three primary natural circulating estrogens:
the presence of a variety of co-activators and co-repressors, and
estradiol, estriol and estrone sulphate (converted in the periphery
the cell and tissue type (Mendelsohn and Karas, 1999). It has been
from estrone and estradiol) (Stanczyk, 1998). Follicle numbers
hypothesized that the complexity of this system may facilitate
fall as menopause approaches (Richardson et al., 1987), and when
selective targeting of ERb, potentially inducing cardiovascular
follicles are deplete at menopause the estradiol levels fall by
effects without adverse stimulation of the reproductive tissues
around 90% compared with reproductive levels (Teede and
Burger, 1998). Estrogen replacement, in the form of HRT, can be
There are also two isoforms of PR: hPR-A and hPR-B. The PR
used therapeutically in post-menopausal women, and a wide
has important interrelationships with the ER system, and
variety of estrogens is available including the natural estrogens
modulates biological responses (Baysal and Losordo, 1996).
(e.g. estradiol), synthetic estrogens (e.g. ethinylestradiol) and
PRs combined with ligand can suppress ER activity; this is
conjugated equine estrogens (CEE) (Anderson, 2000). The
in¯uenced by the PR isoform, the ligand, the promotors and the
pharmacokinetics and potency of these estrogens vary signi®-
cell type (Katzenellenbogen, 1996). Cross-talk occurs between
cantly based on the type of hormone and the route of
ER and PR signalling systems in the modulation of biological
administration, potentially contributing to signi®cantly different
responses (Katzenellenbogen, 1996). The complexity of effects of
observed clinical effects (Anderson, 2000).
the different progestins are likely to re¯ect their structural
divergence from natural progestins, rendering their hormonal
CVD in ever-users of HRT compared with non-users at 0.65 [95%
effects more complex with variable androgenic and estrogenic
con®dence interval (CI) 0.59±0.71] (Grady et al., 1992) and 0.64
(95% CI 0.59±0.68) (Grodstein and Stampfer, 1995). The relative
The complexity of the sex steroid receptor system and the
risk in current users was estimated at 0.5 (95% CI 0.45±0.59)
variety of different estrogenic compounds and progestins used in
(Grodstein and Stampfer, 1995). Although the observational data
clinical practice render the interpretation of existing literature
are almost unanimous, a recent observational study in women
very dif®cult. Ideally, each study needs to be interpreted
with established vascular disease and unstable angina has
individually, and the ®ndings attributed only to the speci®c
suggested a deleterious effect of HRT. In this study, increased
preparations, combinations, doses and routes of administration
events were noted in those initiated on HRT after acute
used for each given tissue end-point and each species studied.
myocardial infarction (Alexander et al., 2001).
Inherent in the design of all observational studies is the
problem of bias, and there are important caveats that must be
applied when interpreting these data. First, most of these studies
HRT has been utilized to treat post-menopausal women for over
compared women who had elected to take HRT with women who
50 years. The bene®ts of HRT include the amelioration of
had either not considered it or elected not to take it (Barrett-
menopausal symptoms, and an improvement in the quality of life.
Connor, 1991). Even in socioeconomically homogeneous pop-
However, HRT has been increasingly prescribed for potential
ulations, these two groups of women differ. Women who elect to
long-term indications including protection against bone loss,
take HRT tend to be better educated, exercise more, have lower
urogenital atrophy and prevention of CVD (MacLennan et al.,
blood pressure and better lipid pro®les and are more likely to
1999). Questions remain about the effectiveness of HRT for long-
participate in preventive health measures than women who do not
term indications, especially cardiovascular disease prevention
take HRT (Barrett-Connor, 1991; Matthews et al., 1996). HRT
(Mosca, 2000, 2001; Mosca et al., 2001a). The clinical
users may therefore be at lower risk of CVD compared with non-
advantages of therapy remain to be proven, and the potential
users even before starting HRT (the `healthy user effect').
disadvantages also need to be clari®ed, including the indication
Adjustment for known confounding variables has little effect on
from epidemiological studies that the incidence of breast cancer
the estimated relative risk of CVD. It does seem likely though that
may be increased with post-menopausal estrogen use.
the healthy user effect would not account for all of the 35±50%
reduction in CVD risk (Bush et al., 1987). Indeed, many of these
biases are less notable in the large cohort study, The Nurses
Health Study, where 70 533 nurses have been followed for 20
years. Those on HRT still have a lower risk of CVD compared
A protective role of estrogen in CVD in post-menopausal women
with non-users (Grodstein et al., 1996, 2000). Nonetheless,
has been suggested by the low risk of CVD among premenopausal
confounding variables (recognized and unrecognized) may have
women and a narrowing of the gender gap after menopause. The
led to an overestimate of the magnitude of HRT reduction in CVD
suggestion that endogenous estrogen maybe cardioprotective was
Second, most women in reported studies were taking
supported by observational data suggesting lower CVD risk in
unopposed estrogen, rather than combined estrogen-progestin,
women on HRT as opposed to non-users (Grady et al., 1992). The
as is now prescribed for women with an intact uterus (Beresford et
assumption that exogenous HRT lowers CVD risk is primarily
al., 1997). Progestins may negate some of the cardiovascular
based on observational data, although supportive mechanistic
effects of estrogens. The apparent opposing effects of progestins
interventional studies suggest bene®cial cardiovascular actions of
has been reviewed (Sitruk-Ware, 2001). In mechanistic studies,
estrogen. In contrast, human controlled trials of HRT focusing on
modulation of the effects of estrogen on plasma lipids, arterial
clinical cardiovascular end-points in both men and women have
dilatation, blood ¯ow and ultimately atherosclerosis have all been
failed to con®rm any bene®t. De®nitively, two large controlled
noted (Adams et al., 1997; Sitruk-Ware, 2001). Limited available
primary prevention studies in post-menopausal women are now
human observational data based on combined estrogen and
underway to address both the risks and bene®ts of HRT, and these
progestin use suggest that this effect may not be substantial
results are awaited with great interest. In the interim, a
(Falkeborn et al., 1992; Psaty et al., 1994; Grodstein et al., 1996),
comprehensive review of the literature is presented herein.
although the type and regimen of progestin used may also be
Extensive cohort and case±control studies have focused on the
relevant (Adams et al., 1990, 1997; Anonymous, 1995).
in¯uence of HRT on a range of cardiovascular end-points
including death, myocardial infarction, angiographic coronary
Proposed mechanisms of the cardioprotective effects of estrogen
stenosis grades and angioplasty and bypass grafting rates (Wolf et
Multiple mechanisms have been proposed to account for the
al., 1991; Grodstein and Stampfer, 1995; Grodstein et al., 1996,
apparent protective effects of estrogen against coronary artery
1997, 2000; Sullivan et al., 1997, 1998). The studies vary
considerably in their end-points and design, and also in the
methods used to eliminate the effects of confounding variables.
Most studies have suggested a 40±50% reduction in cardiovas-
The primary proposed mechanisms of bene®cial estrogen action
cular disease in HRT users compared with non-users (Wolf et al.,
on the cardiovascular system are the effects on lipid metabolism
1991; Grodstein and Stampfer, 1995; Grodstein et al., 1996,
(Godsland, 2001). Oral estrogen treatment reduces plasma total
1997). Two meta-analyses have estimated the relative risk of
and LDL-cholesterol by 5±15%, increases HDL-cholesterol by
Table I. Proposed mechanisms of estrogen action on the cardiovascular
Progestins tend to lower HDL concentrations, and this partially
antagonizes the favourable effects of estrogen (Anonymous, 1994,
1995). The more androgenic progestins have a greater deleterious
effect on HDL (Crook et al., 1992; Anonymous, 1995; Hart et al.,
1998; Godsland, 2001). The least deleterious effects are observed
with dydrogesterone, progesterone and cyproterone acetate
(Godsland, 2001). Pending further clari®cation of the clinical
relevance of combined estrogen and progestin-induced lipid
changes, statins should be ®rst-line therapy for hypercholester-
olaemic women. However, women who require estrogen for other
indications may derive further lipid bene®ts, and in theory the
Reduced proliferation after endothelial injury
selection of less androgenic progestins may be more appropriate
The changes in vasoreactivity observed with estrogen have been
partly attributed to increased nitric oxide (NO) production.
Animal studies have noted gender-speci®c differences in the
NO pathway, with NO release being greater in females, whilst a
lower basal vasomotor tone and less responsiveness to vasocon-
strictors has been noted compared with males (Hayashi et al.,
1992; Binko et al., 1998). Exogenous estrogen increases the
expression of nitric oxide synthase (NOS) in both animals
10%, and reduces lipoprotein Lp(a) concentrations (resistant to
(Weiner et al., 1994) and humans (Hishikawa et al., 1995).
conventional lipid-lowering therapy) (Anonymous, 1995; Darling
Furthermore, estrogen produces relaxation of vascular smooth
et al., 1997; Godsland, 2001). The effect on HDL may be
muscle by a NO-dependent process (Darkow et al., 1997).
especially important, as low plasma HDL is a strong predictor of
Interestingly though, estrogen does not activate downstream
cardiovascular mortality in women. Estrogen also inhibits
mediators in the NO pathway, including the primary effector
oxidation of LDL (Sack et al., 1994), which may render them
molecule protein kinase G (Teede et al., 2001b). However,
less atherogenic. A possible unfavourable effect of estrogen is an
production of the potent vasodilator NO may be cardioprotective
increase (20±25%) in plasma triglyceride concentrations
as it not only regulates blood ¯ow but also inhibits platelet
(Anonymous, 1995; Darling et al., 1997; Godsland, 2001), as
aggregation at the level of the endothelium (Ignarro, 1989).
Endothelin-1 is the most potent of the vasoconstrictor
high triglyceride levels are also predictors of cardiovascular
hormones. Females have lower endothelin levels, especially when
mortality in women. In contrast to oral estrogens, the effects of
pregnant. Trans-sexuals receiving estrogen have been noted to
transdermal estrogen preparations on serum lipids are either
have a fall in endothelin-1 levels (Polderman et al., 1993). A
minimal (Crook et al., 1992) or absent (Lufkin et al., 1992;
recent review based on randomized, controlled studies of HRT on
Modena et al., 1999; Teede et al., 2001d). This is thought to be
the cardiovascular system in post-menopausal women concluded
related to the fact that it is not orally absorbed and therefore does
that HRT reduced endothelin levels (van Baal et al., 2000).
not cause an acute increase in concentrations within the liverÐthe
Potentially, this reduction may also improve vascular tone
It has been estimated that lipid changes resulting from oral
The direct assessment of the effects of sex steroids on arterial
HRT use may only account for 25±50% of the reduction in CVD
blood ¯ow, arterial resistance and vessel diameter has been
in observational studies (Bush et al., 1987). Unlike statins,
studied extensively (Reis et al., 1994). Most studies have
controlled trials are limited and the clinical signi®cance of HRT-
determined endothelial dependence of the artery or vascular
induced lipid changes is not well characterized. In the secondary
territory in question by examining responses to acetylcholine.
prevention HERS trial, lipid bene®ts were observed, yet reduction
Invasive vascular reactivity studies have demonstrated that
in CVD events was not noted (Hulley et al., 1998).
atherosclerotic arteries exhibit a reduced response to acetylcho-
The clinical relevance of the HRT-induced lowering of Lp(a)
line administration, which is reversed by estrogen addition in the
also needs clari®cation, as the pathophysiological signi®cance of
monkey model (Williams et al., 1990). Non-invasive studies of
this complex polymorphic lipoprotein particle remains unclear
endothelial function using ultrasound techniques including ¯ow-
(Marcova and Koschinsky, 1999; Godsland, 2001). Interestingly,
mediated vasodilation have been contradictory. Observational and
a recent HERS study subgroup analysis suggested that Lp(a) was
short-term estrogen studies have suggested bene®t, whilst long-
an independent risk factor for recurrent coronary heart disease in
term controlled trials have not necessarily supported these results
post-menopausal women, and that treatment with estrogen and
(McCrohon et al., 1996; Sorensen et al., 1997; Teede et al.,
progestin lowered Lp(a) levels. It also demonstrated that among
women with a high baseline Lp(a) level, those on HRT had a
Studies in post-menopausal women have suggested that
lower rate of cardiovascular events compared with those with
estrogen therapy may have anti-ischaemic effects in women with
lower baseline Lp(a) (Shlipak et al., 2000).
established CVD. A controlled trial in 74 post-menopausal
women with stable angina showed that HRT increased the time to
estrogen-mediated inhibition of the migration and replication of
ST depression and total exercise duration compared with placebo
smooth muscle cells in vitro (Makela et al., 1999). In the rabbit,
therapy (Sanderson et al., 2001). This ®nding supported the
rat and mouse, intimal thickening after mechanical carotid
results of a previous uncontrolled trial (Rosano et al., 1997).
balloon injury appears to be reduced by estrogen pretreatment,
this being mediated by inhibition of vascular smooth muscle
Atherosclerosis and vascular structural changes
proliferation (Foegh et al., 1994; Sullivan et al., 1995; Oparil et
The effect of HRT on atherosclerosis is perhaps best appreciated
al., 1997). Interestingly, progestin (MPA) blocked the effects of
from an extensive series of experiments in the cynomolgus
estrogen in this model (Oparil et al., 1997). When given alone,
monkey atherosclerosis model (Clarkson, 1994; Clarkson et al.,
MPA enhanced the neointimal response to balloon injury in intact
1995, 2001). Monkeys were oophorectomized, and then rando-
females, presumably by blocking productionÐand thus the
mized to placebo, oral or transdermal estrogen alone, combined
vasoprotective effectÐof endogenous estrogen. However, when
HRT with continuous or cyclic progestin or tibolone. They were
given in combination with exogenous estrogen, MPA negated the
fed an atherogenic diet for 2 years, after which (at necropsy) a
bene®cial reduction in neointimal proliferation with estrogen
comprehensive assessment of coronary atherosclerosis was
alone (Oparil et al., 1997). Estrogen has also been shown to
undertaken (Clarkson, 1994; Clarkson et al., 1995, 2001).
facilitate the re-endothelialization of the carotid artery after
Estrogen alone reduced the cholesteryl ester content (Wagner et
balloon injury (White et al., 1997). Furthermore, in vitro estrogen
al., 1997) and the atherosclerotic plaque by either 50%
inhibits vascular smooth muscle cell proliferationÐan effect that
(transdermal therapy) or 70% (oral therapy) compared with those
is directly mediated by the ER (Baysal and Losordo, 1996).
animals receiving placebo (Clarkson et al., 1995). Studies in
atherosclerosis models in other species, including rabbits, have
also suggested that estrogen provides protection against athero-
Thrombosis is an important component of arterial vascular events
sclerosis (Brehme et al., 1999). It should be noted, however, that
as well as venous thromboembolic events (VTE). Previously,
debate persists as to whether animal models of atheroma, induced
arterial cardiovascular events were attributed to progressive
solely by an atherogenic diet, actually provide a true model of
obstruction from atherosclerotic plaques, though this concept
has been revised as it has become clear that cardiovascular events
The effects of additional progestins on atherosclerosis in
are characterized by an acute obstructive process superimposed
animal models are less clear. In the cynomolgus monkey, natural
on a previously mild to moderate single atherosclerotic lesion
progesterone or cyclic medroxyprogesterone acetate (MPA) did
(Theroux and Cairns, 1998). Subsequent morphological analysis
not appear to in¯uence the bene®cial effects of estrogen on
has revealed plaque disruption and intraluminal thrombi (Ross,
atherosclerosis (Adams et al., 1990). However, the effects of
1993). Indeed, coronary thrombosis was noted on underlying
continuous MPA in this model were con¯icting. Some studies
ruptured plaque in 95% of those suffering sudden cardiovascular
suggested that continuous MPA negated the bene®cial effects of
death (Davies and Thomas, 1984). Accordingly, the mainstay of
estrogen, including reduced atherosclerosis, aortic connective
acute treatment of acute myocardial infarction is now thrombo-
tissue remodelling after lipid lowering and a reduction in
lytic therapy aimed at dissolving the occluding thrombus and
dobutamine-induced myocardial ischaemia (Adams et al., 1997;
reperfusing the ischaemic myocardium (ISIS Collaborative
Register et al., 1998; Williams et al., 2002). However, in a recent
Group, 1992). Moreover, simple measures including aspirin and
study in the same monkey model, continuous MPA did not affect
heparin therapy have proven useful in both the treatment and
the bene®cial reduction in atherosclerosis seen with estrogen
prevention of clinical events (Hansson et al., 1998; Gaziano et al.,
(Clarkson et al., 2001). In rabbits, coronary ¯ow rates were
2000). Furthermore, in¯ammatory changes within atherosclerotic
increased with estrogen therapyÐan effect not observed when
plaque appear to increase vulnerability to rupture, leading to
estrogen was combined with several types of progestin, including
thrombus formation, myocardial ischaemia and clinically overt
MPA (Gorodeski et al., 1998). The atherosclerotic effects of
disease. In this setting an intervention which is pro-in¯ammatory
combining speci®c progestins with estrogen are not yet clari®ed,
and procoagulant, potentially may increase arterial thrombosis
and therefore also clinical cardiovascular events.
Interestingly, it was noted (Hanke et al., 1999) that estrogen
Concerns have been raised about the prothrombotic effects of
could inhibit the progression of atherosclerosis in rabbits when
estrogen, with an increase in both VTE and potentially also
only mild or moderate vessel wall abnormalities were present, but
arterial events (Coronary Drug Project Research Group, 1970;
appeared unable to do so once severe atherosclerotic disease was
Hulley et al., 1998; Hoibraaten et al., 2000, 2001; Teede et al.,
established. The anti-atherosclerotic effects of estrogen were
2000a; Alexander et al., 2001; Peverill et al., 2001). In controlled
apparently mediated by the endothelium, which becomes
trials, HRT increased the risk of VTE by 3- to 4-fold, with the
dysfunctional once atherosclerosis develops. This is supported
increase noted in the early 1±2 years of treatment (Figure 1)
by studies in the monkey model where the bene®cial effect of
(Hulley et al., 1998; Hoibraaten et al., 2000). This increase
estrogen on acetylcholine-mediated vasodilation only occurred in
appeared to be independent of, and multiplicative with, other
segments of the coronary artery where mild atherosclerosis was
prothrombotic risk factors (Lowe et al., 2000).
present. No effects were noted in arterial segments with severe
It has also been proposed that the prothrombotic effect of HRT
atherosclerosis, suggesting that estrogen may not be useful in
may have been responsible for the early increase in thrombotic
secondary prevention (Clarkson, 1994).
arterial cardiovascular events observed in the secondary preven-
In a rat model of carotid injury, vascular ERb receptors were
tion of cardiovascular disease, the HERS study (Hulley et al.,
up-regulated, and this was accompanied by a dose-dependent,
1998), though this has yet to be clari®ed. A population-based
Additional effectsA plethora of additional mechanisms of HRT action on the
vascular system has been demonstrated, including effects on ion
channels, membrane receptor aggregation and changes in protein
phosphorylation status (Mendelsohn and Karas, 1999; Pines et al.,
1999; Stefano et al., 2000). Other estrogen effects include
changes in the renin±angiotensin system (Proudler et al., 1995)
and bene®cial changes in carbohydrate metabolism and body fat
distribution (Barrett-Connor et al., 1989). A recent review based
on randomized, controlled studies of HRT on the cardiovascular
system in post-menopausal women also concluded that HRT
reduced homocysteine levels (van Baal et al., 2000).
Whilst individual mechanisms of estrogen action are of interest,
Figure 1. Cardiovascular (CV) outcomes by treatment group and year since
the mosaic of data available on the cardiovascular effects of sex
randomization in the `HERS' study (Hulley et al., 1998). AMI = acute
hormones is complex and in¯uenced by a variety of factors,
myocardial infarction; DVT = deep vein thrombosis.
including natural versus synthetic hormones, species, age,
hormonal status, which vessel is studied, baseline endothelial
case±control study has demonstrated that in hypertensive women
function, arterial structure, lipid and coagulation factors.
with a ®rst non-fatal acute myocardial infarction (AMI), there was
Furthermore, it remains controversial as to whether there is a
a positive association between genetic thrombophilia, HRT use
true animal model for atherosclerosis as the models used to date
and AMI (Psaty et al., 2001). Overall, the concern is that the
have atherosclerosis induced by very high levels of cholesterol
procoagulant effects of HRT may negate the cardiovascular
intake without other co-existent risk factors. Therefore, despite
this wealth of data it remains dif®cult to assess the effect of HRT
In mechanistic studies based on the use of accurate immuno-
on the vascular system (Teede and McGrath, 1999).
diagnostic haemostatic markers, HRT appears primarily to
activate coagulation, and although it increases ®brinolytic
potential this may only be a secondary physiological response
Randomized controlled human interventional data
to the up-regulation noted in coagulation (Teede et al., 2000;
Although the extensive data on the in¯uence of HRT on vascular
Hoibraaten et al., 2001). Although the mechanism of estrogen-
disease in both human and animal studies appear positive, the
induced up-regulation of coagulation remains unknown, in
picture portrayed in the randomized trials on the effects of HRT
controlled trials HRT has been shown to reduce the vital tissue
on cardiovascular disease suggests that HRT may not be
factor pathway inhibitor (TFPI), along with a reduction in other
bene®cial, but rather have a neutral effect or even increase the
endogenous anticoagulants (Peverill et al., 2001; Hoibraaten et
al., 2001). Potentially, this may allow up-regulation of the
Early data were available from the 1960s with the randomized
coagulation cascade. Tissue factor is the principal initiator of the
Coronary Drug Project (CDP) involving over 7500 male subjects
extrinsic coagulation pathway, and the fall in TFPI has been
with documented myocardial infarction (Coronary Drug Project
directly correlated to the degree of coagulation activation noted
Research Group, 1970). This project was stopped prematurely as
with HRT (Hoibraaten et al., 2001). The effects on platelets may
no bene®ts of estrogen were observed. However, a higher rate of
be neutral (Teede et al., 2001), though further research is required
venous thrombosis was observed, and in a recent reanalysis of the
CDP data a signi®cant increase in coronary heart disease within
As noted, the pathophysiology of an acute arterial ischaemic
the ®rst 4 months of treatment was demonstrated (Mosca, 2001).
event includes plaque rupture and subsequent thrombosis. At
Recently, a substantial human study on the effects of HRT on
present, there is no available test that will predict which plaques
vascular disease in women, the `HERS' study, was reported
are vulnerable to rupture, occurring in the setting of an
(Hulley et al., 1998). This was a well-designed, double-blind,
in¯ammatory process within the plaque. C-reactive protein
placebo-controlled, randomized study of combined continuous
(CRP) has been noted to be an independent cardiovascular risk
oral HRT (0.625 mg conjugated equine estrogen + 5 mg medroxy
factor (Koenig, 2001), though as yet it has not been ascertained
progesterone acetate) use in the secondary prevention of vascular
whether CRP is a marker or is truly pathogenic in the
disease, in 2763 post-menopausal women of mean age 66.7 years,
in¯ammatory process, or whether modulation of CRP will alter
with pre-existing coronary atherosclerotic disease over 4.1 years.
the disease process (Koenig, 2001). HRT has been documented to
The study failed to demonstrate any overall difference in vascular
increase CRP plasma levels (Ridker et al., 1999; Walsh et al.,
events, including myocardial infarction, coronary revasculariza-
2000), potentially increasing the risk of plaque rupture. In contrast
tion, unstable angina, congestive cardiac failure, stroke, transient
to these results, reductions in circulating levels of the in¯amma-
ischaemic attack or peripheral arterial disease, between the
tory markers E-selectin, vascular cell adhesion molecule (V-
placebo and active treatment groups. This was despite an
CAM) and intracellular adhesion molecule (I-CAM), which may
improvement in lipid parameters in those patients receiving
also re¯ect plaque stability, have been noted with HRT (van Baal
HRT (Hulley et al., 1998). The arterial vascular event rate in the
et al., 1999, 2000). However, again the net clinical signi®cance of
®rst year was actually signi®cantly increased [relative risk
these ®ndings has yet to be established.
(RR) = 1.52], falling over time to a RR of 0.67 by the fourth
year (Figure 1). The trend towards a fall in the cardiovascular
compared estradiol + monthly gestodene, estradiol + 3-monthly
event rate over the 4 years was signi®cant, yet overall, no
gestodene, or a control group on no HRT. In 321 healthy post-
differences were noted between the active and placebo groups
menopausal women with increased IMT (representing early
subclinical atherosclerosis), one year of HRT did not slow IMT
On the basis of previously published data, these results were
progression despite falls in LDL-cholesterol levels (Angerer et
unexpected. Clinically signi®cant effects of HRT on the
al., 2001). However, a more recent study in 222 post-menopausal
haemostatic system were con®rmed, with an increase in venous
women without pre-existing CVD compared unopposed estrogen
thrombosis similar to that seen with the oral contraceptive pill
with placebo therapy with and without lipid-lowering agents over
(Hulley et al., 1998). A two-edged sword effect of HRT was
2 years. The rate of progression of subclinical atherosclerosis
proposed, with the authors theorising that the prothrombotic
(IMT) was lower in those patients randomized to unopposed
effects of estrogen may negate any possible atherosclerotic
estradiol compared with placebo, although a signi®cant effect of
bene®ts in women with established cardiovascular disease and
estradiol was only noted in those women not receiving lipid-
pre-existing plaques, which are prone to rupture, though this has
lowering therapy (Hodis et al., 2001). The women in the latter
study did not have pre-existing CVD, and were studied for longer
The criticisms of the HERS study were related primarily to the
compared with the previously described investigation (Angerer et
progestin regimens used (continuous medroxy progesterone
acetate, shown in some animal studies to negate the bene®cial
A pooled study which was published in 2000, analysed data
effects of estrogen, yet not in others) (Adams et al., 1997;
from 28 randomized controlled trials that compared HRT
Clarkson et al., 2001), although this progestin regimen is common
(n = 2206) with another agent (n = 1278) for up to 3 years
in clinical practice. Otherwise, it was a well-designed and well-
(Hemminki and McPherson, 2000). The focus was to compare the
executed study, and the only human controlled trial based on
rate of cardiovascular events in these controlled trials to the
clinical disease end-points to date. It is a landmark study, which
reduced cardiovascular event rate in those on HRT noted
has sounded an important note of caution for practitioners
previously in observational trials (Barrett-Connor and Grady,
prescribing HRT in women with known cardiovascular disease.
1998). The pooled data demonstrated an increased cardiovascular
The most signi®cant limitation is that the results apply only to the
event rate in those on HRT (OR 1.78, 95% CI 0.7±4.52) that was
speci®c HRT preparation used and the population studied. The
not statistically signi®cant. The ®ndings do not support a
®ndings are not applicable to those without established vascular
disease; nor can they be extrapolated to encompass the effects of
bene®cial effect of HRT on cardiovascular event rate seen in
other estrogen doses and routes of administration or other
Other controlled trials focusing on surrogate outcomes are
The `ERA' trial, which was published in 2000, compared 3.2
ongoing. The Women's Angiographic Vitamin and Estrogen
years of treatment with estrogen (n = 100), combined estrogen +
(WAVE) trial, the Women's Estrogen/ Progestin and Lipid-
progestin (n = 104) or placebo (n = 105) in post-menopausal
Lowering Hormone Atherosclerosis Regression Trial (WELL-
women aged 42±80 years with pre-existing coronary disease
HART) and the Estrogen and Graft Atherosclerosis Research
(Herrington et al., 2000). There was no signi®cant difference in
(EAGAR) trial based on angiography in women with bypass
the rate of progression of coronary atherosclerosis between the
grafts, are all due for completion in the near future should add
three groups. Coronary atherosclerosis based on angiographic
further to our knowledge base. These studies, along with the
data does not necessarily predict the risk of subsequent clinical
HERS and ERA studies, involve women with established vascular
events, and is not a hard clinical end-point. As with all currently
disease. Animal data suggest that estrogen may not have
available surrogate markers of vascular disease, it does not re¯ect
bene®cial cardiovascular effects in women once atherosclerosis
plaque stability and therefore cannot predict those most likely to
is established and endothelial damage has occurred (Honore et al.,
rupture and suffer acute cardiovascular events. However, it does
1996; Hanke et al., 1999). Both human observational data
provide a human study similar to the original monkey data
(Herrington et al., 2001) and interventional data suggest that this
focusing on atherosclerosis development, and the results of this
may be the case (Haines et al., 2001), thus highlighting the need
study are important for two primary reasons. First, an estrogen-
for further investigation into the role of HRT in primary
alone arm was included and did not demonstrate bene®ts over
combined therapy; second, this study suggested that previous
The Women's Health Initiative trial, a primary prevention trial,
controlled animal trials focusing on coronary atherosclerosis may
is an ongoing study comparing estrogen + progestin to estrogen
not be representative of responses in humans.
alone in healthy post-menopausal women aged 55±79 years, with
This is also supported by the recent double-blind, placebo-
a target enrolment of 27 500 cases. In April 2000, the
controlled trial in 664 post-menopausal women with ischaemic
investigators informed the participants that `during the ®rst 2
stroke or transient ischaemic attack. Treatment with 1 mg of oral
years there was a small increase in the number of heart attacks,
17b-estradiol daily did not alter the risk of subsequent events,
strokes and blood clots in women taking active hormones
with a total of 99 strokes or deaths in the active and 93 in the
compared to inactive pills'. Over time, these differences appeared
placebo groups over 2.8 years. The RR was 1.1 (95% CI 0.8±1.4)
to diminish. The overall event rate was low, occurring in <1% of
women, and the difference between the groups did not reach
Further randomized controlled studies focusing on another
statistical signi®cance. Yet, the effects of HRT would be
surrogate end-point, carotid artery intimal medial thickness
consistent with the HERS study, and given that they are seen in
(IMT), have also examined the effect of HRT. The ®rst study
healthy women, even infrequent events are concerning. A report
a reduction in vascular adhesion molecules by endothelial cellsÐ
a theoretically bene®cial effect (Simoncini and Genazzani, 2000).
Rabbit studies have suggested a reduction in atherosclerosis
development (Zandberg et al., 1998), although a comparative
study in the cynomolgus monkey atherosclerosis model demon-
strated improved lipids and reduced atherosclerosis with CEE, but
not with tibolone. Tibolone reduced HDL, but had no impactÐ
either adverse or bene®cialÐon coronary artery atherosclerosis
(Clarkson et al., 2001). A small trial in 10 post-menopausal
women with angina has demonstrated increased exercise
tolerance similar to that observed with estrogen use (Lloyd et
al., 1998), whilst a randomized trial based on the effects of
tibolone on the surrogate marker, carotid IMT, is pending. There
is a suggestion that tibolone may not increase thrombotic risk,
although the data are inadequate to draw any such conclusions at
present (Winkler et al., 2000). The net clinical signi®cance of
these changes in surrogate endpoints remains unknown, and we
must await data from controlled trials focusing on de®nitive
clinical end-points to establish the role of tibolone in CVD
Figure 2. The chemical structures of 17b-estradiol, genestein and daidzein.
Selective ER modulatorsSelective ER modulators (SERMS) are non-steroidal estrogenic
scheduled for 2005 will provide more de®nitive data on the
compounds with both estrogenic and non-estrogenic actions. They
are established for the prevention of breast cancer and for the
treatment of osteoporosis (Bush et al., 2001). The data on the
cardiovascular effects of SERMS are based on in-vivo animal and
human studies, as well as limited data from controlled interven-
tional trials on clinical cardiovascular end-points.
Lower-dose regimens (0.3 mg CEE or equivalent) have been the
The data on the vascular effects of raloxifene have been
focus of much recent research into HRT (Ettinger, 1999). Studies
extensively reviewed (Moscarelli and Cox, 2000). Clinical trials
have suggested that low-dose HRT can relieve menopausal
have demonstrated that SERMs do not change HDL or
symptoms and vaginal atrophy (Utian et al., 2001), prevent bone
triglyceride levels, but do signi®cantly improve Lp(a) and LDL
loss when combined with calcium (Genant et al., 1997; Recker et
levels (Walsh et al., 1998; Godsland, 2001). Other circulating
markers (including homocysteine levels) each fell, but CRP levels
al., 1999) and improve lipid pro®les without inducing endometrial
were not changed with raloxifene, compared with falls in
hyperplasia (Genant et al., 1997; Lobo et al., 2001). The primary
homocysteine and a rise in CRP seen with HRT (Walsh et al.,
advantage of low-dose regimens is the improved side-effect
pro®le and better long-term compliance. A recent analysis from
Vascular structural and functional effects have been noted with
the 20-year cohort study, The Nurses' Health Study in 70 533
animal data which are suggestive of up-regulation of NO with
women, suggested that the cardioprotective effect of 0.3 mg of
vasorelaxation and reduced arterial intimal thickening in response
CEE was equivalent to that of the higher dose of 0.625 mg
to injury. Raloxifene inhibited atherosclerosis in the cholesterol-
(Grodstein et al., 2000). This ®nding is encouraging, but is based
fed rabbit model (Bjarnason et al., 1997), but not in the monkey
on observational data, and once again further clinical trials are
model, where no reduction in atherosclerosis was observed
required to clarify the role of low-dose HRT regimens in the
Human interventional data have been completed with tamox-
ifen in a randomized controlled clinical trial in 13 388 women
focusing on breast cancer prevention (Reis et al., 2001). No effect
The estro-progestogen tibolone is a steroid hormone with a
was noted on CVD end-points. Even in a subsequent subgroup
progestin-like structure that is converted to estrogenic and
analysis for those at high baseline risk akin to the HERS study
androgenic derivatives in vivo. It has been shown to improve
population, no effect of tamoxifen on cardiovascular events was
menopausal symptoms and to improve bone density (although
noted (Reis et al., 2001). The ongoing double-blind, placebo-
fracture data are still lacking), and it potentially has fewer side
controlled Raloxifene Use for the Heart (RUTH) study, focusing
effects than conventional HRT (Hammar et al., 1998; Crook,
on the effects of raloxifene in 10 101 post-menopausal women
2001). Inadequate human observational data exist on the
aged >55 years and with established vascular disease or multiple
cardiovascular effects of tibolone. Human studies have provided
risk factors, should signi®cantly contribute to our understanding
mixed results with reductions in HDL, but also reductions in
of the net clinical cardiovascular effects of raloxifene (Mosca et
triglycerides and Lp(a) levels, with less effect than conventional
al., 2001b). Also, the increase in risk of venous thromboembolic
HRT on LDL levels (Godsland, 2001). Animal studies suggested
disease appears to be equivalent to that seen with estrogen
Table II. The American Heart Association guidelines on HRT and the prevention of cardiovascular disease
Secondary preventiond HRT should not be initiated for the secondary prevention of CVD. d The decision to continue or to stop HRT in women with CVD who have been undergoing long-term HRT
should be based on established non-coronary bene®ts and risks and patient preference.
d If a woman develops an acute CVD event or is immobilized while undergoing HRT, it is prudent to
consider discontinuance of the HRT, or to consider VTE prophylaxis while she is hospitalized to minimize
risk of VTE associated with immobilization. Reinstitution of HRT should be based on established non-
coronary bene®ts and risks, as well as patient preference.
Primary preventiond Firm clinical recommendations for primary prevention await the results of ongoing randomized clinical
d There are insuf®cient data to suggest that HRT should be initiated for the sole purpose of primary
d Initiation and continuation of HRT should be based on established non-coronary bene®ts and risks,
possible coronary bene®ts and risks, and patient preference.
From Mosca et al. and the American Heart Association (2001a). Hormone replacement therapy and
cardiovascular disease. Circulation, 104, 499±503.
(Ettinger et al., 1999). Given the established prothrombotic risks
soybean nor isolated sources of phytoestrogens reduce menopau-
of the currently available SERMS, the lack of knowledge on the
sal symptoms over placebo therapy (Baber et al., 1999;
clinical relevance of changes in surrogate CVD risk factors, and
Kotsopoulos et al., 1999; Murkies et al., 2000). In the setting of
the apparent neutral cardiovascular effects of tamoxifen in clinical
the apparent selectivity and complexity of the endocrine effects of
trials, these agents cannot be presently considered as cardiopro-
phytoestrogens, it has been suggested that individual effects need
to be characterized for each putative estrogenic compound on
each estrogenic end-point (Hughes et al., 1991).
Diets rich in phytoestrogens may reduce cardiovascular disease.
Phytoestrogens are a diverse group of plant-derived compounds,
Speci®cally, high soy intake is associated with a lower incidence
similar to estrogenic steroids (Figure 2) (Davies, 1998).
of cardiovascular disease, and the ingestion of vegetable
Iso¯avones are the most common phytoestrogens (Davis et al.,
proteinÐparticularly soyÐis associated with a reduced risk of
1999), with genistein and diadzein being the most estrogenically
coronary heart disease and improved risk factor status
active and found in greatest concentrations in soybean (Price and
(Aldercreutz, 1998; Davis et al., 1999; Teede et al., 2001c).
Fenwick, 1985). Phytoestrogens have been reported to have both
Interventional studies indicate that soy has favourable effects on
agonist and antagonist estrogenic effects (Kuiper et al., 1998),
lipid pro®les in both primates and humans, and on blood pressure
which are not necessarily parallel to those of estrogen. More
in humans (Anderson et al., 1995; Davis et al., 1999; Teede et al.,
recently however, the relative binding af®nities of several
2001c). A meta-analysis of controlled human clinical trials noted
phytoestrogens to ERa and ERb have been shown to be
that soy protein consumption signi®cantly reduced total choles-
signi®cant, especially for ERb. ERb is highly expressed in
terol (9.3% decrease, 95% CI 0.35±0.85 mmol/l), LDL-cholester-
vascular endothelium and smooth muscle cells; therefore, in
ol (12.9% decrease, 95% CI 0.30±0.82 mmol/l) and triglycerides
theory phytoestrogens may trigger many of the biological
(10.5% decrease, 95% CI 0.003±0.29 mmol/l), with little change
responses that are evoked by physiological estrogens (Kuiper et
in HDL (Anderson et al., 1995). Responses were related to pre-
al., 1998). However, whilst the af®nity of phytoestrogens for ER
treatment plasma cholesterol levels. Most research has focused on
has been established, ligand±ER interactions are inherently
phytoestrogen-rich whole foods or protein isolates, with little
complex, and our understanding of the biological potencies of
information on concentrated phytoestrogen subfractions in tablet
form. However, limited data suggest that isolated phytoestrogens
The observed estrogenic effects of phytoestrogens have been
are less effective at improving cardiovascular risk factors
reviewed extensively (Davis et al., 1999; Murkies et al., 2000). In
(Hodgson et al., 1998). Soy supplementation has also been
animals, they include reproductive dysfunction, selective neu-
associated with reduced atherosclerosis in animals and improved
roendocrine effects and effects on sexual development (Davis et
vascular function in female monkeys, but not in humans (Honore
al., 1999; Murkies et al., 2000). In premenopausal women,
et al., 1996; Teede et al., 2001c). The active components of soy
menstrual disturbances have been noted, whilst in post-menopau-
are not yet established, with potential contributors including
sal women improvement in the vaginal maturation index has been
vegetable protein, antioxidants and phytoestrogens.
noted (Bickoff et al., 1961; Dalais et al., 1998). Yet more studies
Despite observational data on humans and animal and human
have failed to show estrogenic effects of dietary soybean in both
interventional data focusing on surrogate end-points, once again
animals and humans (Baird et al., 1995; Tansey et al., 1998;
the net clinical effects of either soy or isolated phytoestrogens on
Teede et al., 2001c). Controlled trials have suggested that neither
the cardiovascular system remain unknown. Although ongoing
studies with combinations of phytoestrogens, antioxidants and
atherosclerosis: a randomised controlled trial. Arterioscler. Thromb. Vasc.
micronutrients are awaited with interest, there are currently
Anonymous (1994) Randomised comparison of oestrogen versus oestrogen
insuf®cient data available to recommend the consumption of
plus progestogen hormone replacement therapy in women with
isolated supplements for the prevention of CVD. In contrast, the
hysterectomy. Medical Research Council's General Practice Research
consumption of diverse and balanced diets, which are rich in
Framework. Br. Med. J., 312, 473±478.
foods containing many nutrients, including antioxidants and
Anonymous (1995) Effects of estrogen or estrogen/progestin regimens on
heart disease risk factors in postmenopausal women. The postmenopausal
phytoestrogens, can be safely recommended (Teede and
estrogen/progestin interventions (PEPI) trial. JAMA, 273, 199±208.
Anonymous (1998) Effect of intensive blood-glucose control with metformin
on complications in overweight patients with type 2 diabetes (UKPDS
34). UK Prospective Diabetes Study (UKPDS) Group. Lancet, 352, 854±
Baber, R.J., Templeman, C., Morton, T., Kelly, G.E. and West, L. (1999)
CVD is the number one killer of both men and women in Western
Randomized placebo-controlled trial of an iso¯avone supplement and
countries. Prevention strategies are very effective in reducing the
menopausal symptoms in women. Climacteric, 2, 85±92.
Baird, D.D., Umbach, D.M., Lansdell, L., Hughes, C.L., Setchell, K.D.,
burden of CVD. Well-established prevention strategies including
Weinberg, C.R., Haney, A.F., Wilcox, A.J. and Mclachlan, J.A. (1995)
lifestyle modi®cations and speci®cally targeted pharmacological
Dietary intervention study to assess estrogenicity of dietary soy among
treatments remain under-utilized, especially in women.
postmenopausal women. J. Clin. Endocrinol. Metab., 80, 1685±1690.
Considering the controversy surrounding the role of HRT in the
Barrett-Connor, E. (1991) Postmenopausal estrogen and prevention bias. Ann.
prevention of CVD, it is arguable that although this remains a
Barrett-Connor, E. and Grady, D. (1998) Hormone replacement therapy, heart
potentially exciting area for further research, the issue of
disease and other considerations. Annu. Rev. Public Health, 19, 55±72.
appropriate clinical use of HRT for CVD prevention is yet to
Barrett-Connor, E., Wingard, D. and Criqui, M.H. (1989) Postmenopausal
be clari®ed. There is a need to appreciate the limitations of
estrogen use and heart disease risk factors in the 1980s. JAMA, 261, 2095±
existing observational and interventional data on the vascular
Baysal, K. and Losordo, D. (1996) Estrogen receptors and cardiovascular
effects of HRT. Ongoing research in this area is important. The
disease. Clin. Exp. Pharmacol. Physiol., 23, 537±548.
role of lower-dose HRT needs to be clari®ed, but potentially most
Beresford, S.A.A., Weiss, N.S., Voigt, L.F. and McKnight, B. (1997) Risk of
endometrial cancer in relation to use of oestrogen combined with cyclic
exciting is the prospect of selective modulation of the estrogen
progestagen therapy in postmenopausal women. Lancet, 349, 458±461.
receptor to activate the bene®cial cardiovascular effects of HRT,
Bickoff, E.M. (1961) Estrogen-like substances in plants. In: Physiology of
without adverse procoagulant and reproductive effects. Whilst the
Reproduction: Proceedings of the 22nd Annual Biology Colloquium,
observational data need not be discarded and the potential for
Hisaw, Fl. Oregon State University Press, Oregon, p. 140.
Binko, J., Murphy, T.V. and Majewski, H. (1998) 17Beta-oestradiol enhances
HRT to provide primary CVD prevention has still to be
nitric oxide synthase activity in endothelium-denuded rat aorta. Clin. Exp.
considered, the recent American Heart Association guidelines
suggest that there is no current indication to commence HRT for
Bjarnason, N.H., Haarbo, J., Byrjalsen, I., Kauffman, R.F. and Christiansen, C.
the prevention of CVD alone (Table II). Essentially, these
(1997) Raloxifene inhibits aortic accumulation of cholesterol in
ovariectomized, cholesterol-fed rabbits. Circulation, 96, 1964±1969.
guidelines recommend that HRT should be instituted based on
Brehme, U., Bruck, B., Gugel, N., Wehrmann, M., Hanke, S., Finking, G.,
other accepted indications, with caution applied to those with
Schmahl, F.W. and Hanke, H. (1999) Aortic plaque size and endometrial
established CVD. Furthermore, HRT should not precludeÐand
response in cholesterol-fed rabbits treated with estrogen plus continuous
sequential progestin. Arterioscler. Thromb. Vasc. Biol., 19, 1930±1937.
cannot replaceÐspeci®c targeted therapies proven to reduce the
Burger, H. and Teede, H. (2001) Guest editorial: the AHA guidelines on
hormone replacement therapy and cardiovascular disease. Maturitas, 40,
Bush, T.L., Barrett-Connor, E., Cowan, L.D., Criqui, M.H., Wallace, R.B.,
Suchindran, C.M., Tyroler, H.A. and Rifkind, B.M. (1987) Cardiovascular
mortality and noncontraceptive use of estrogen in women: results from the
Adams, M., Register, T., Golden, D., Wagner, J. and Williams, K. (1997)
lipid research clinics program follow-up study. Circulation, 75, 1102±
Medroxyprogesterone acetate antagonises inhibitory effects of conjugated
equine estrogens on coronary artery atherosclerosis. Arterioscler. Thromb.
Bush, T.L., Blumenthal, R., Lobo, R. and Clarkson, T.B. (2001) SERMs and
cardiovascular disease in women. How do these agents affect risk?
Adams, M.R., Kaplan, J.R., Manuck, S.B., Koritnik, D.R., Parks, J.S., Wolfe,
M.S. and Clarkson, T.B. (1990) Inhibition of coronary artery
Clarkson, T. (1994) Estrogens, progestins, and coronary heart disease in
atherosclerosis by 17-b estradiol in ovariectomized monkeys. Lack of
cynomolgus monkeys. Fertil. Steril., 62, 147S±151S.
an effect of added progesterone. Arteriosclerosis, 10, 1051±1057.
Clarkson, T.B., Hughes, C.L. and Klein, K.P. (1995) The nonhuman primate
Ades, P. (2001) Cardiac rehabilitation and secondary prevention of coronary
model of the relationship between gonadal steroids and coronary heart
heart disease. N. Engl. J. Med., 345, 892±902.
disease. Prog. Cardiovasc. Dis,. 38, 189±198.
Aldercreutz, H. (1998) Epidemiology of phytoestrogens. BallieÁre's Clin.
Clarkson, T.B., Anthony, M.S. and Jerome, C.P. (1998) Lack of effect of
raloxifene on coronary artery atherosclerosis of postmenopausal monkeys.
Alexander, K.P., Newby, L.K., Hellkamp, A.S., Harrington, R.A., Peterson,
J. Clin. Endocrinol. Metab., 83, 721±726.
E.D., Kopecky, S., Langer, A., O'Gara, P., O'Connor, C.M., Daly, R.N. et
Clarkson, T.B., Anthony, M.S. and Wagner, J.D. (2001) A comparison of
al. (2001) Initiation of hormone replacement therapy after acute
tibolone and conjugated equine estrogens effects on coronary artery
myocardial infarction is associated with more cardiac events during
atherosclerosis and bone density of postmenopausal monkeys. J. Clin.
follow-up. J. Am. Coll. Cardiol., 38, 1±7.
Anderson, F. (2000) Kinetics and pharmacology of estrogens in pre- and
Coronary Drug Project Research Group (1970) The Coronary Drug Projects
postmenopausal women. Int. J. Fertil., 38, 55±64.
initial ®ndings leading to modi®cations of the research protocol. JAMA,
Anderson, J.W., Johnstone, B.M. and Cook-Newell, M.E. (1995) Meta-
analysis of the effects of soy protein intake on serum lipids. N. Engl. J.
Crook, D. (2001) Cardiovascular risk assessment for postmenopausal hormone
replacement therapies such as tibolone (Livial). In: Genazzani, A.R. (ed.),
Angerer, P., Stork, S., Kothny, W., Schmitt, P. and von Schacky, C. (2001)
Hormone Replacement Therapy and Cardiovascular Disease. Parthenon,
Effects of oral postmenopausal hormone replacement on progression of
Crook, D., Cust, M.P., Gangar, K.F., Worthington, M., Hillard, T.C.,
combined hormone replacement therapy on arterial reactivity in
Stevenson, J.C., Whitehead, M.I. and Wynn, V. (1992) Comparison of
postmenopausal women with angina pectoris. Atherosclerosis, 159,
transdermal and oral oestrogen-progestin replacement therapy: effects on
serum lipids and lipoproteins. Am. J. Obstet. Gynecol., 166, 950±955.
Hammar, M., Christau, S., Nathorst-Boos, J., Rud, T. and Garre, K. (1998) A
Dalais, F.S., Rice, G.E., Wahlqvist, M.L. et al. (1998) Effects of dietary
double blind, randomised trial comparing the effects of tibolone and
phytoestrogens in postmenopausal women. Climacteric, 1, 124±129.
continuous combined hormone replacement therapy in postmenopausal
Darkow, D.J., Lu, L. and White, R.E. (1997) Estrogen relaxation of coronary
women with menopausal symptoms. Br. J. Obstet. Gynaecol., 105, 904±
artery smooth muscle is mediated by nitric oxide and cGMP. Am. J.
Hanke, H., Kamenz, J., Hanke, S., Spiess, J., Lenz, C., Brehme, U., Bruck, B.,
Darling, G.M., Johns, J.A., McCloud, P.I. and Davis, S.R. (1997) Estrogen and
Finking, G. and Hombach, V. (1999) Effect of 17b estradiol on pre-
progestin compared with simvastatin for hypercholesterolemia in
existing atherosclerotic lesions: role of the endothelium. Atherosclerosis,
postmenopausal women. N. Engl. J. Med., 337, 595±601.
Davies, G.C. (1998) Chemistry of antihormones. In: Fraser, I.S. (ed.),
Hansson, L., Zanchetti, A., Carruthers, S.G., Dahlof, B., Elmfeldt, D., Julius,
Estrogens and Progestogens in Clinical Practice. Churchill Livingstone,
S., Menard, J., Rahn, K.H., Wedel, H. and Westerling, S. (1998) Effects of
intensive blood-pressure lowering and low-dose aspirin in patients with
Davies, M.J. and Thomas, A. (1984) Thrombosis and acute coronary artery
hypertension: principal results of the Hypertension Optimal Treatment
lesions in sudden cardiac ischaemic death. N. Engl. J. Med., 310, 1137±
(HOT) randomised trial. Lancet, 351, 1755±1762.
Hart, D.M., Farish, E., Fletcher, C.D., Barnes, J.F., Hart, H., Nolan, D. and
Davis, S.R., Dalais, F.S., Simpson, E.R. and Murkies, A.L. (1999)
Spowart, K. (1998) Long-term effects of continuous combined HRT on
Phytoestrogens in health and disease. Rec. Prog. Hormone Res., 54,
bone turnover and lipid metabolism in postmenopausal women.
Ettinger, B. (1999) Personal perspective on low-dosage estrogen therapy for
Hayashi, T., Fukuto, J.M., Ignarro, L.J. and Chaudhuri, G. (1992) Basal
postmenopausal women. J. North Am. Menopause Soc., 6, 273±276.
release of nitric oxide from aortic rings is greater in female rabbits than in
Ettinger, B., Black, D.M., Mitlak, B.H., Knickerbocker, R.K., Nickelsen, T.,
male rabbits: implications for atherosclerosis. Proc. Natl Acad. Sci. USA,
Genant, H.K., Christiansen, C., Delmas, P.D., Zanchetta, J.R., Stakkestad,
J. et al. (1999) Reduction of vertebral fracture risk in postmenopausal
Heart Protection Study Collaborative Group (2001) MRC/BHF Heart
women with osteoporosis treated with raloxifene. JAMA, 282, 637±645.
Protection Study of cholesterol- lowering therapy and anti-oxidant
Falkeborn, M., Persson, I., Adami, H., Bergstrom, R., Eaker, E., Lithell, H.,
vitamin supplementation in a wide range of patients at increased risk of
Mohsen, R. and Naessen, T. (1992) The risk of acute myocardial
coronary heart disease death. (abstract) http://www.ctsu.ox.ac.uk/hps/
infarction after estrogen and estrogen-progestogen replacement. Br. J.
Hemminki, E. and McPherson, K. (2000) Value of drug-licensing documents
Foegh, M.L., Asotra, S., Howell, M.H. and Ramwell, P.W. (1994) Estradiol
in studying the effect of postmenopausal HRT on cardiovascular disease.
inhibition of arterial neointimal hyperplasia after balloon injury. J. Vasc.
Hennekens, C.H., Dyken, M.L. and Fuster, V. (1997) Aspirin as a therapeutic
Friday, K.E. (2001) Diabetes, obesity and cardiovascular disease. In:
agent in cardiovascular disease: a statement for healthcare professionals
Genazzani, A.R. (ed.), Hormone Replacement Therapy and
from the American Heart Association. Circulation, 96, 2751±2753.
Cardiovascular Disease. Parthenon, New York, pp. 37±43.
Herrington, D.M., Reboussin, D.M., Brosnihan, K.B., Sharp, P.C., Shumaker,
Gaziano, J.M., Skerrett, P.J. and Buring, J.E. (2000) Aspirin in the treatment
S.A., Snyder, T.E., Furberg, C.D., Kowalchuk, G.J., Stuckey, T.D.,
and prevention of cardiovascular disease. Haemostasis, 30 (Suppl. 3), 1±
Rogers, W.J. et al. (2000) Effects of estrogen replacement therapy on the
progression of coronary artery atherosclerosis. N. Engl. J. Med., 343, 522±
Genant, H.K., Lucas, J., Weiss, S., Akin, M., Emkey, R., McNaney-Flint, H.,
Downs, R., Mortola, J., Watts, N., Yang, H.M. et al. (1997) Low-dose
Herrington, D.M., Espeland, M.A., Crouse, J.R., Robertson, J., Riley, W.A.,
esteri®ed estrogen therapy: effect on bone, plasma estradiol
McBurnie, M.A. and Burke, G.L. (2001). Estrogen replacement and
concentrations, endometrium and lipid levels. Estrabab/Osteoporosis
brachial artery ¯ow mediated vasodilation in older women. Arterioscler.
Study Group. Arch. Intern. Med., 157, 2609±2615.
Thromb. Vasc. Biol., 21, 1955±1961.
Giardina, E.G. (2000) Heart disease in women. Int. J. Fertil. Womens Med.,
Hishikawa, K., Nakaki, T., Marumo, T., Suzuki, H., Kato, R. and Saruta, T.
(1995) Up-regulation of nitric oxide synthase by estradiol in human aortic
Glassberg, H. and Balady, G.J. (1999) Exercise and heart disease in women:
endothelial cells. FEBS Lett., 360, 291±293.
why, how and how much? Cardiol. Rev., 7, 301±308.
Hjalmarson, A., Elmfeldt, D., Herlitz, J., Holmberg, S., Malek, I., Nyberg, G.,
Godsland, I.F. (2001) Effects of postmenopausal hormone replacement
Ryden, L., Swedberg, K., Vedin, A., Waagstein, F. et al. (1981) Effects on
therapy on lipid, lipoprotein and apolipoprotein (a) concentrations:
mortality of metoprolol in acute myocardial infarction: a double blind
analysis of studies published from 1974±2000. Fertil. Steril., 75, 898±915.
randomised trial. Lancet, 2, 823±827.
Gorodeski, G.I., Yang, T., Levy, M.N., Goldfarb, J. and Utian, W.H. (1998)
Hodgson, J.M., Puddey, I.B. and Beillin, L.J. (1998) Supplementation with
Modulation of coronary vascular resistance in female rabbits by estrogen
iso¯avonoid phytoestrogens does not alter serum lipid concentrations: a
and progesterone. J. Soc. Gynecol. Invest., 5, 197±202.
randomised controlled trial in humans. J. Nutrition, 28, 728±732.
Grady, D., Rubin, S.M., Petitti, D.B., Fox, C.S., Black, D., Ettinger, B.,
Hodis, H.N., Mack, W.J., Lobo, R.A., Shoupe, D., Sevanian, A., Mahrer, P.R.,
Ernster, V.L. and Cummings, S.R. (1992) Hormone therapy to prevent
Selzer, R.H., Liu, C.R., Liu, Ch C.H. and Azen, S.P. (2001) Estrogen in
disease and prolong life in postmenopausal women. Ann. Intern. Med.,
the prevention of atherosclerosis. A randomized, double-blind, placebo-
controlled trial. Ann. Intern. Med., 135, 939±953.
Grodstein, F. and Stampfer, M. (1995) The epidemiology of coronary heart
Hoibraaten, E., Qvigstad, E., Arnesen, H., Larson, S., Wickstrom, E. and
disease and estrogen replacement in postmenopausal women. Prog.
Sandset, P.M. (2000) Increased risk of recurrent venous thromboembolism
during hormone replacement therapy. Thromb. Haemost., 84, 961±967.
Grodstein, F., Stampfer, M.J., Manson, J.E., Colditz, G.A., Willett, W.C.,
Hoibraaten, E., Qvigstad, E., Andersen, T.O., Mowinckel, M. and Sandset,
Rosner, B., Speizer, F.E. and Hennekens, C.H. (1996) Postmenopausal
P.M. (2001) The effects of hormone replacement therapy (HRT) on
estrogen and progestin use and the risk of cardiovascular disease. N. Engl.
hemostatic variables in women with previous venous thromboembolism.
Results from a randomised, double-blind, clinical trial. Thromb. Haemost.,
Grodstein, F., Stampfer, M.J., Colditz, G.A., Willett, W.C., Manson, J.E.,
Joffe, M., Rosner, B., Fuchs, C., Hankinson, S.E., Hunter, D.J. et al.
Honore, E.K., Williams, J.K., Washburn, S.A. and Herrington, D.M. (1996)
(1997) Postmenopausal hormone therapy and mortality. N. Engl. J. Med.,
The effects of disease severity and sex on coronary endothelium-
dependent vasomotor function in an atherosclerotic primate model.
Grodstein, F., Manson, J.E., Colditz, G.A., Willett, W.C., Speizer, F.E. and
Stampfer, M.J. (2000) A prospective, observational study of
Hooper, L., Summerbell, C.D. Higgins, J.P.T., Thompson, R.L., Clements, G.,
postmenopausal hormone replacement therapy and primary prevention
Capps, N., Davey, S., Riemersma, R.A. and Ebrahim, S. (2001) Reduced
of cardiovascular disease. Ann. Intern. Med., 133, 933±941.
or modi®ed dietary fat for preventing cardiovascular disease. Cochrane
Haines, C.J., Yim, S.F. and Sanderson, J.E. (2001) The effects of continuous
Database of Systematic Reviews; Issue 2.
Hu, F.B., Stampfer, M.J., Manson, J E., Grodstein, F., Colditz, G.A., Speizer,
and apolipoprotein (a) size. A synergistic role in advanced
F.E. and Willett, W.C. (2000) Trends in the incidence of coronary heart
atherosclerosis? Circulation, 100, 1151±1153.
disease and changes in diet and lifestyle in women. N. Engl. J. Med., 343,
Matthews, K.A., Kuller, L.H., Wing, R.R., Meilahn, E.N. and Plantinga, P.
(1996) Prior to use of estrogen replacement therapy, are users healthier
Hu, F.B., Manson, J.E., Stampfer, M.J., Colditz, G., Liu, S., Solomon, C.G.
than nonusers? Am. J. Epidemiol., 143, 971±978.
and Willett, W.C. (2001) Diet, lifestyle and the risk of type 2 diabetes
McCrohon, J.A., Adams, M.R., McCredie, R.J., Robinson, J., Pike, A., Abbey,
mellitus in women. N. Engl. J. Med., 345, 790±797.
M., Keech, A.C. and Celermajer, D.S. (1996) Hormone replacement
Hughes, C.L., Jr, Chakinala, M.M., Reece, S.G., Miller, R.N., Schomberg,
therapy is associated with improved arterial physiology in healthy post-
D.W., Jr and Basham, K.B. (1991) Acute and subacute effects of naturally
menopausal women. Clin. Endocrinol., 45, 435±441.
occurring estrogens on luteinizing hormone secretion in the
Mendelsohn, M.E. and Karas, R.H. (1999) Mechanisms of disease: the
ovariectomized rat: Part 2. Reprod. Toxicol., 5, 127±132.
protective effects of estrogen on the cardiovascular system. N. Engl. J.
Hulley, S., Grady, D., Bush, T., Furberg, C., Herrington, D., Riggs, B. and
Vittinghoff, E. (1998) Randomized trial of estrogen plus progestin for
Modena, M.G., Molinari, R., Muia, N., Jr, Castelli, A., Pala, F. and Rossi, R.
secondary prevention of coronary heart disease in postmenopausal
(1999) Double-blind randomized placebo-controlled study of transdermal
estrogen replacement therapy on hypertensive postmenopausal women.
Ignarro, L.J. (1989) Biological actions and properties of endothelium-derived
nitric oxide formed and released from artery and vein. Circ. Res., 65, 1±
Mosca, L. (2000) The role of hormone replacement therapy in the prevention
of postmenopausal heart disease. Arch. Intern. Med., 160, 2263±2272.
ISIS Collaborative Group ISIS-2 (1988) Randomised trial of intravenous
Mosca L. (2001) Hormone replacement therapy and myocardial infarction. In:
streptokinase, oral aspirin, both or neither among 17,187 cases of
Genazzani, A.R. (ed.), Hormone Replacement Therapy and
suspected acute myocardial infarction: ISIS-2. Lancet, 2, 349±360.
Cardiovascular Disease. Parthenon, New York, pp. 173±176.
ISIS Collaborative Group ISIS-3 (1992) A randomised comparison of
Mosca, L., Grundy, S.M., Judelson, D., King, K., Limacher, M., Oparil, S.,
streptokinase vs. tissue plasminogen activator vs. anistreplase and of
Pasternak, R., Pearson, T.A., Redberg, R.F., Smith, S.C., Jr et al. (1999)
aspirin plus heparin vs. aspirin alone among 41,299 cases of suspected
Guide to preventive cardiology for women. Circulation, 99, 2480±2484.
acute myocardial infarction. ISIS-3 (Third International Study of Infarct
Mosca, L., Jones, W.J., King, K.B., Ouyang, P., Redberg, R.F. and Hill, M.N.
(2000) Awareness, perception and knowledge of heart disease risk and
Katzenellenbogen, B.S. (1996) Estrogen receptors: bioactivities and
prevention among women in the United States. Arch. Family Med., 9,
interactions with cell signaling pathways. Biol. Reprod., 54, 287±293.
Koenig W. (2001) C-reactive protein: risk assessment in the primary
Mosca, L., Collins, P., Herrington, D.M., Mendelsohn, M.E., Pasternak, R.C.,
prevention of atherosclerotic disease. Has the time come for including it
Robertson, R.M., Schenck-Gustafsson, K., Smith, S.C., Jr, Taubert, K.A.,
in the risk pro®le? Ital. Heart J., 2, 157±163.
Wenger, N.K. and the American Heart Association (2001a) Hormone
Kotsopoulos, D., Dalais, F., Liang, Y., McGrath, B.P. and Teede, H.J. (1999)
replacement therapy and cardiovascular disease. A statement for
The effects of phytoestrogens on menopausal symptoms in
healthcare professionals from the American Heart Association.
postmenopausal women. Climacteric, 3, 61±67.
Kuiper, G.G., Carlson, B., Grandien, K., Enmark, E., Haggblad, J., Nilsson, S.
Mosca, L., Barrett-Connor, E., Wenger, N.K., Collins, P., Grady, D.,
and Gustafsson, J.A. (1997) Comparison of the ligand binding speci®city
Kornitzer, M., Moscarelli, E., Paul, S., Wright, T.J., Helterbrand, J.D.
and transcript tissue distribution of estrogen receptors alpha and beta.
and Anderson, P.W. (2001b) Design and methods of the Raloxifene Use
for the Heart (RUTH) study. Am. J. Cardiol., 88, 392±395.
Kuiper, G.G., Lemmen, J.G., Carlsson, B., Corton, J.C., Safe, S.H., van der
Moscarelli, E. and Cox, D.A. (2000) Cardiovascular effects of raloxifene: data
Saag, P.T., van der Burg, B. and Gustafsson, J.A. (1998) Interaction of
from preclinical studies and clinical trials in postmenopausal women. In:
estrogenic chemicals and phytoestrogens with estrogen receptor beta.
Genazzani, A.R. (ed.), Hormone Replacement Therapy and
Cardiovascular Disease. Parthenon, New York, pp. 159±164.
Murkies, A.L., Teede, H.J. and Davis, S.R. (2000) What is the role of
Lloyd, G.W., Patel, N.R., McGing, E.A., Cooper, A.F., Kamalvand, K. and
phytoestrogens in treating menopausal symptoms. Med. J. Aust., 173,
Jackson, G. (1998) Acute effects of hormone replacement therapy with
tibolone on myocardial ischaemia in women with angina. Int. J. Clin.
Oparil, S., Levine, R.L., Chen, S.J., Durand, J. and Chen, Y.F. (1997) Sexually
dimorphic response of the balloon-injured rat carotid artery to hormone
Lobo, R.A., Bush, T., Carr, B.R. and Pickar, J.H. (2001) Effects of lower doses
treatment. Circulation, 95, 1301±1307.
of conjugated equine estrogens and medroxyprogesterone acetate on
Peverill, R., Teede, H., Smolich, J., Malan, E., Kotsopoulos, D., Tipping, P.
plasma lipids and lipoproteins, coagulation factors and carbohydrate
and McGrath, B. (2001) Effect of combined oral hormone replacement
metabolism. Fertil. Steril., 76, 13±24.
therapy on tissue factor pathway inhibitor and Factor VII. Clin. Sci., 101,
Lowe, G., Woodward, M., Vessey, M., Rutney, A., Gough, P. and Daly, E.
(2000) Thrombotic variables and risk of idiopathic venous
Pines, A., Averbuch, M., Fisman, E.Z. and Rosano, G.M. (1999) The acute
thromboembolism in women aged 45±64 years. Thromb. Haemost., 83,
effects of sublingual 17beta-estradiol on the cardiovascular system.
Lowel, H., Koenig, W., Engel, S., Hormann, A. and Keil, U. (2000) The
Polderman, K.H., Stehouwer, C.D.A., Kamp, G.J., Dekker, G.A., Verheugt,
impact of diabetes mellitus on survival after myocardial infarction: can it
F.W. and Gooren, L.J. (1993) In¯uence of sex hormones on plasma
be modi®ed by drug treatment? Diabetologia, 43, 218±226.
endothelin levels. Ann. Intern. Med., 341, 1264±1265.
Lufkin, E.G., Wahner, H.W., O'Fallon, W.M., Hodgson, S.F., Kotowicz,
Pollock, M.L., Franklin, B.A., Balady, G.J., Chaitman, B.L., Fleg, J.L.,
M.A., Lane, A.W., Judd, H.L., Caplan, R.H. and Riggs, B.L. (1992)
Fletcher, B., Limacher, M., Pina, I.L., Stein, R.A., Williams, M. and
Treatment of postmenopausal osteoporosis with transdermal estrogen.
Bazzarre, T. (2000) Resistance exercise in individuals with and without
cardiovascular disease: an advisory from the committee on exercise,
MacLennan, A.H., Wilson, D.H. and Taylor, A.W. (1999) Hormone
rehabilitation, and prevention, council on clinical cardiology. Circulation,
replacement therapies in women at risk of cardiovascular disease and
osteoporosis in South Australia in 1997. Med. J. Aust., 170, 524±527.
Progress Collaborative Group (2001) Randomised trial of a perindopril-based
Makela, S., Savolainen, H., Aavik, E., Myllarniemi, M., Strauss, L., Taskinen,
blood-pressure-lowering regimen among 6105 individuals with previous
E., Gustafsson, J.A. and Hayry, P. (1999) Differentiation between
stroke or transient ischaemic attack. Lancet, 358, 1033±1041.
vasculoprotective and uterotrophic effects of ligands with different
Price, K.R. and Fenwick, G.R. (1985) Naturally occurring oestrogens in foods
binding af®nities to estrogen receptors alpha and beta. Proc. Natl Acad.
± a review. Food Addit. Contam., 2, 73±106.
Proudler, A.J., Ahmed, A.I.H., Crook, D., Fogelman, I., Rymer, J.M. and
Manson, J.E., Colditz, G.A., Stampfer, M.J., Willett, W.C., Krolewski, A.S.,
Stevenson, J.C. (1995) Hormone replacement therapy and serum
Rosner, B., Arky, R.A., Speizer, F.E. and Hennekens, C.H. (1991) A
angiotensin-converting enzyme activity in postmenopausal women.
prospective study of maturity onset diabetes and risk of coronary heart
disease and stroke in women. Arch. Intern. Med., 151, 1141±1147.
Psaty, B.M., Heckbert, S.R., Atkins, D., Lemaitre, R., Koepsell, T.D., Wahl,
Marcova, S.M. and Koschinsky, M.L. (1999) Lipoprotein (a) concentration
P.W., Siscovick, D.S. and Wagner, E.H. (1994) The risk of myocardial
infarction associated with the combined use of estrogens and progestins in
assessment of endothelial vasomotor function. In: Born, G.V.R. and
postmenopausal women. Arch. Intern. Med., 154, 1333±1339.
Schwarz, C.J. (eds), Vascular Endothelium. Schattauer, New York, pp.
Psaty, B.M., Smith, N.L., Lemaitre, R.N., Vos, H.L., Heckbert, S.R., LaCroix,
A.Z. and Rosendaal, F.R. (2001) Hormone replacement therapy,
Stampfer, M.J., Hu, F.B., Manson, J.E., Rimm, E.B. and Willett, W.C. (2000)
prothrombotic mutations, and the risk of incident nonfatal myocardial
Primary prevention of coronary heart disease in women through diet and
infarction in postmenopausal women. JAMA, 285, 906±913.
lifestyle. N. Engl. J. Med., 343, 16±22.
Recker, R.R., Davies, K.M., Dowd, R.M. and Heaney, R.P. (1999) Effect of
Stanczyk, F. (1998) Structure-function relationships and estrogens and
low-dose continuous estrogen and progesterone therapy with calcium and
progestins. In: Fraser, I.S. (ed.), Estrogens and Progestogens in Clinical
vitamin D on bone in elderly women. Ann. Intern. Med., 130, 897±904.
Practice. Churchill Livingstone, London, pp. 27±39.
Register, T.C., Adams, M.R., Golden, D.L. and Clarkson, T.B. (1998)
Stefano, G.B., Prevot, V., Beauvillain, J.C., Cadet, P., Fimiani, C., Welters, I.,
Conjugated equine estrogens alone, but not in combination with
Fricchione, G.L., Breton, C., Lassalle, P., Salzet, M. and Bil®nger, T.V.
medroxyprogesterone acetate, inhibit aortic connective tissue
(2000) Cell-surface estrogen receptors mediate calcium-dependent nitric
remodeling after plasma lipid lowering in female monkeys. Arterioscler.
oxide release in human endothelia. Circulation, 101, 1594±1597.
Thromb. Vasc. Biol., 18, 1164±1171.
Sullivan, J.M., El-Zeky, F., Vander Zwaag, R. and Ramanathan, K.B. (1997)
Reis, S.E., Gloth, S.T., Blumenthal, R.S., Resar, J.R., Zacur, H.A.,
Effect on survival of estrogen replacement therapy after coronary artery
Gerstenblith, G. and Brinker, J.A. (1994) Ethinyl estradiol acutely
bypass grafting. Am. J. Cardiol., 79, 847±850.
attenuates abnormal coronary vasomotor responses to acetylcholine in
Sullivan, J.M., Vander Zwagg, R., Lemp, G.F., Hughes, J.P., Maddock, V.,
postmenopausal women. Circulation, 89, 52±60.
Kroetz, F.W., Ramanathan, K.B. and Mirvis, D.M. (1988)
Reis, S.E., Costantino, J.P., Wickerham, D.L., Tan-Chiu, E., Wang, J. and
Postmenopausal estrogen use and coronary atherosclerosis. Ann. Intern.
Kavanah, M. (2001) Cardiovascular effects of tamoxifen in women with
and without heart disease: Breast Cancer Prevention Trial. J. Natl Cancer
Sullivan, T.R., Karas, R.H., Aronovitz, M., Faller, G.T., Ziar, J.P., Smith, J.J.,
O'Donnell, T.F., Jr and Mendelsohn, M.E. (1995) Estrogen inhibits the
Richardson, S.J., Senikas, V. and Nelson, J.F. (1987) Follicular depletion
response-to-injury in a mouse carotid artery model. J. Clin. Invest., 96,
during the menopausal transition: evidence for accelerated loss and
ultimate exhaustion. J. Clin. Endocrinol. Metab., 65, 1231±1234.
Tansey, G., Hughes, C.L., Jr, Cline, J.M., Krummer, A., Walmer, D.K. and
Ridker, P.M., Hennekens, C.H., Rifai, N., Buring, J.E. and Manson, J.E.
Schmoltzer, S. (1998) Effects of dietary soybean estrogens on the
(1999) Hormone replacement therapy and increased plasma concentration
reproductive tract in female rats. Proc. Soc. Exp. Biol. Med., 217, 340±
of C-reactive protein. Circulation, 100, 713±716.
Rogers, W.J., Bowlby, L.J., Chandra, N.C., French, W.J., Gore, J.M.,
Teede, H.J. and Burger, H. (1998) Endocrine changes across the
Lambrew, C.T., Rubison, R.M., Tiefenbrunn, A.J. and Weaver, W.D.
Perimenopause. In: Lobo, R. (ed.), Management of the Menopause.
(1994). Treatment of myocardial infarction in the United States:
Lippincott Ravenswood, New York, pp. 52±64.
observations from the national Health Registry of myocardial infarction.
Teede, H.J. and Kritharides, L. (2000) Dietary prevention of cardiovascular
disease, In: Identifying and promoting speci®c nutritional and physical
Rosano, G.M.C., Sarrel, P.N.M., Poole-Wilson, P.A. and Collins, P. (1993)
activity needs of women over 40. Med. J. Aust., 173, (Suppl.) S93±S112.
Bene®cial effects of estrogen on exercise-induced myocardial ischaemia
Teede, H.J. and McGrath, B.P. (1999) Cardiovascular effects of sex hormones.
in women with coronary artery disease. Lancet, 342, 133±136.
Rosano, G.M.C., Caixeta, A.M., Chierchia, S.L., Arie, S., Lopez-Hidalgo, M.,
Teede, H.J., McGrath, B.P., Smolich, J.J., Malan, E., Kotsopoulos, D., Liang,
Pereira, W.I., Leonardo, F., Webb, C.M., Pileggi, F. and Collins, P. (1997)
Y. and Peverill, R.E. (2000) Postmenopausal hormone replacement
Acute anti-ischemic effect of estradiol in postmenopausal women with
therapy increases both coagulation activity and ®brinolysis. Arterioscler.
coronary artery disease. Circulation, 96, 2837±2841.
Thromb. Vasc. Biol., 20, 1404±1409.
Ross, R. (1993) The pathogenesis of atherosclerosis: a perspective for the
Teede, H.J., Majewski, H., McGrath, B.P. and Turner, A. (2001a) Platelet
aggregation is not reduced in postmenopausal women on oral hormone
Rubins, H.B., Robins, S.J., Collins, D., Fye, C.L., Anderson, J.W., Elam,
replacement therapy. Clin. Sci., 100, 207±213.
M.B., Faas, F.H., Linares, E., Schaefer, E.J., Schectman, G. et al. (1999)
Teede, H.J., van der Zypp, A. and Majewski, H. (2001b) Gender differences in
Gem®brozil for the secondary prevention of coronary heart disease in men
protein kinase G vasorelaxation of rat aorta. Clin. Sci., 100, 473±479.
with low levels of high-density lipoprotein cholesterol. N. Engl. J. Med.,
Teede, H.J., Dalais, F., Kotsopoulos, D., Liang, Y. and McGrath, B.P. (2001c)
Soy protein dietary supplementation containing phytoestrogens improves
Sack, M.N., Rader, D.J. and Cannon, R.O. (1994) Estrogen and inhibition of
lipid pro®les and blood pressure: a double blind, randomised, placebo
oxidation of low-density lipoproteins in postmenopausal women. Lancet,
controlled study in men and postmenopausal women. J. Clin. Endocrinol.
Sacks, F.M., Pfeffer, M.A., Moye, L.A., Rouleau, J.L., Rutherford, J.D., Cole,
Teede, H.J., Liang, Y., Zoungas, S., Kotsopoulos, D., Craven, R. and
T.G., Brown, L., Warnica, J.W., Arnold. J.M., Wun, C.C. et al. (1996)
McGrath, B.P. (2001d) A placebo controlled trial of transdermal estrogen
The effects of pravastatin on coronary events after myocardial infarction
replacement therapy in postmenopausal women: effects on arterial
in patients with average cholesterol levels. N. Engl. J. Med., 335, 1001±
compliance and endothelial function. Climacteric, 4, 1±10.
Teede, H.J., Liang, Y., Kotsopoulos, D., Zoungas, S., Craven, R. and
Sanderson, J.E., Haines, C.J., Yeung, L., Yip, G.W., Tang, K., Yim, S.F.,
McGrath, B.P. (2001e) A placebo controlled trial of long-term oral
Jorgensen, L.N. and Woo, J. (2001) Anti-ischemic action of estrogen-
combined continuous hormone replacement therapy in postmenopausal
progestogen continuous combined hormone replacement therapy in
women: effects on arterial compliance and endothelial function. Clin.
postmenopausal women with established angina pectoris: a randomized,
placebo-controlled, double-blind, parallel group trial. J. Cardiovasc.
Theroux, P. and Cairns, J.A. (1998) Unstable angina. In: Yusef, S., Cairns, J.,
Camm, A.J., Fallen, E.L. and Gersh, B.J. (eds), Evidence-Based
Scandanavian Simvastatin Survival Study Group (1994) Randomised trial of
Cardiology. BMJ Books, London, pp. 395±417.
cholesterol lowering in 4444 patients with coronary heart disease. Lancet,
Tsang, T.S., Barnes, M.E., Gersh, B.J. and Hayes, S.N. (2000) Risks of
coronary heart disease in women: current understanding and evolving
Shlipak, M.G., Simon, J.A., Vittinghoff, E., Lin, F., Barrett-Connor, E.,
concepts. Mayo Clin. Proc., 75, 1289±1303.
Knopp, R.H., Levy, R.I. and Hulley, S.B. (2000) Estrogen and progestin,
Tuomilehto, J., Lindstrom, J., Eriksson, J.G., Valle, T.T., Hamalainen, H.,
lipoprotein(a), and the risk of recurrent coronary heart disease events after
Ilanne-Parikka, P., Keinanen-Kiukaanniemi, S., Laakso, M., Louheranta,
A., Rastas, M., Salminen, V., Uusitupa, M. and the Finnish Diabetes
Simoncini, T. and Genazzani, A.R. (2000) Tibolone inhibits leukocyte
Prevention Study Group (2001) Prevention of type 2 diabetes mellitus by
adhesion molecule expression in human endothelial cells. Mol. Cell.
changes in lifestyle among subjects with impaired glucose tolerance. N.
Sitruk-Ware, R. (2001) Progestins and the cardiovascular system. In:
Utian, W.H., Shoupe, D., Bachmann, G., Pinkerton, J.V. and Pickar, J.H.
Genazzani, A.R. (ed.), Hormone Replacement Therapy and
(2001) Relief of vasomotor symptoms and vaginal atrophy with lower
Cardiovascular Disease. Parthenon, New York, pp. 37±43.
doses of conjugated equine estrogens and medroxyprogesterone acetate.
Sorensen, K.E., Dorup, I. and Celermajer, D.S. (1997) Noninvasive
Van Baal, W.M., Emeis, J.J., Kenemans, P., Kessel, H., Peters-Muller, E.R.,
Williams, J.K., Adams, M.R. and Klopfenstein, H.S. (1990) Estrogen
Schalkwijk, C.G., van der Mooren, M.J. and Stehouwer, C.D. (1999)
modulates responses of atherosclerotic coronary arteries. Circulation,
Short-term hormone replacement therapy: reduced plasma levels of
soluble adhesion molecules. Eur. J. Clin. Invest., 29, 913±921.
Williams, J.K., Hall, J., Anthony, M.S., Register, T.C., Reis, S.E. and
Van Baal, W.M., Kooistra, T. and Stehouwer, C.D. (2000) Cardiovascular
Clarkson, T.B. (2001) A comparison of tibolone and hormone
disease risk and hormone replacement therapy (HRT): a review based on
replacement therapy on coronary artery and myocardial function in
randomised, controlled studies in postmenopausal women. Curr. Med.
ovariectomised atherosclerotic monkeys. Menopause, 9, 41±51.
Wilson, K., Gibson, N., Willan, A. and Cook, D. (2000) Effect of smoking
Viscoli, C.M., Brass, L.M., Kernan, W.N., Sarrel, P.M., Suissa, S. and
cessation on mortality after myocardial infarction: meta-analysis of cohort
Horwitz, R.I. (2001) A clinical trial of estrogen-replacement therapy after
studies. Arch. Intern. Med., 160, 939±944.
ischaemic stroke. N. Engl. J. Med., 345, 1243±1249.
Winkler, U.H., Altkemper, R., Kwee, B., Helmond, F.A. and Coelingh
Wagner, J.D., Cefalu, W.T., Anthony, M.S., Litwak, K.N., Zhang, L. and
Bennink, H.J. (2000) Effects of tibolone and continuous combined
Clarkson, T.B. (1997) Dietary soy protein and estrogen replacement
hormone replacement therapy on parameters in the clotting cascade:
therapy improve cardiovascular risk factors and decrease aortic
a multicenter, double-blind, randomised study. Fertil. Steril., 74,
cholesteryl ester content in ovariectomized cynomolgus monkeys.
Wolf, P.H., Madans, J.H., Finucane, F.F., Higgins, M. and Kleinman, J.C.
Walsh, B., Kuller, L., Wild, R., Paul, S., Farmer, M., Lawrence, J.B., Shah,
A.S. and Anderson, P.W. (1998) Effects of raloxifene on serum lipids and
(1991) Reduction of cardiovascular disease-related mortality among
coagulation factors in healthy postmenopausal women. JAMA, 279, 1445±
postmenopausal women who use hormones: evidence from a national
cohort. Am. J. Obstet. Gynecol., 164, 489±494.
Walsh, B.W., Paul, S., Wild, R.A., Dean, R.A., Tracy, R.P., Cox, D.A. and
World Health Organization (1999) World Health Organization-International
Anderson, P.W. (2000) The effects of hormone replacement therapy and
Society of Hypertension (WHO-ISH) Guidelines Subcommittee. J.
raloxifene on C-reactive protein and homocysteine in healthy
postmenopausal women: a randomised controlled trial. J. Clin.
Wood, D., and the Joint European Task Force (2001) Established and
emerging cardiovascular risk factors. Am. Heart J., 141, S49±S57.
Weiner, C.P., Lizasoain, I., Baylis, S.A., Knowles, R.G., Charles, I.G. and
Yusef, S., Cairns, J., Camm, A.J., Fallen, E.L. and Gersh, B.J. (eds) (1998)
Moncada, S. (1994) Induction of calcium-dependent nitric oxide synthases
Evidence-Based Cardiology. BMJ Books, London.
by sex hormones. Proc. Natl Acad. Sci. USA, 91, 5212±5216.
Zandberg, P., Peters, J.L., Demacker, P.N., Smit, M.J., de Reeder, E.G. and
White, C.R., Shelton, J., Chen, S.J., Darley-Usmar, V., Allen, L., Nabors, C.,
Meuleman, D.G. (1998) Tibolone prevents atherosclerotic lesion
Sanders, P.W., Chen, Y.F. and Oparil, S. (1997) Estrogen restores
formation in cholesterol fed ovariectomised rabbits. Arterioscler.
endothelial cell function in an experimental model of vascular injury.
Thromb. Vasc. Biol., 18, 1844±1854.
Whitehead, M. (1994) Progestins and androgens. Fertil. Steril., 62, 161±167.
Submitted on December 11, 2001; accepted on February 21, 2002
Sheraton Soma Bay Suppléments pour vos transferts. Exemple de prix TTC par personne par trajet, en euros, à partir de : 15 € (véhicule privé avec chauffeur parlant français). Durée : 50 min Compagnies aériennes de référence vers Hurghada : Air Med, XL Airways, Air Cairo (direct) – départ le samedi Compagnies alternatives : Egyptair/Air France (via Le Caire) – dépa
The Whitman Building, 8380 Riverwalk Park Blvd., Suite 200, Fort Myers, FL 33919 Telephone (239) 561-7337 Fax (239) 561-0244 Evelyn R. Kessel, M.D. Brent M. Myers, M.D. Irma Cruz, M.D Date and time of your procedure:_______________________ Arrive at:_____________________ Location: ⃞ Riverwalk Endoscopy Center 8380 Riverwalk Park Blvd #220, Fort Mye
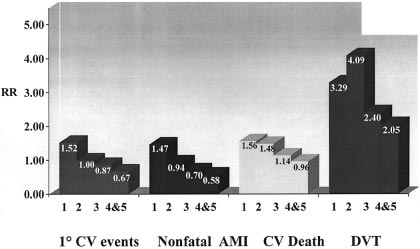 Additional effectsA plethora of additional mechanisms of HRT action on the
vascular system has been demonstrated, including effects on ion
channels, membrane receptor aggregation and changes in protein
phosphorylation status (Mendelsohn and Karas, 1999; Pines et al.,
1999; Stefano et al., 2000). Other estrogen effects include
changes in the renin±angiotensin system (Proudler et al., 1995)
and bene®cial changes in carbohydrate metabolism and body fat
distribution (Barrett-Connor et al., 1989). A recent review based
on randomized, controlled studies of HRT on the cardiovascular
system in post-menopausal women also concluded that HRT
reduced homocysteine levels (van Baal et al., 2000).
Additional effectsA plethora of additional mechanisms of HRT action on the
vascular system has been demonstrated, including effects on ion
channels, membrane receptor aggregation and changes in protein
phosphorylation status (Mendelsohn and Karas, 1999; Pines et al.,
1999; Stefano et al., 2000). Other estrogen effects include
changes in the renin±angiotensin system (Proudler et al., 1995)
and bene®cial changes in carbohydrate metabolism and body fat
distribution (Barrett-Connor et al., 1989). A recent review based
on randomized, controlled studies of HRT on the cardiovascular
system in post-menopausal women also concluded that HRT
reduced homocysteine levels (van Baal et al., 2000).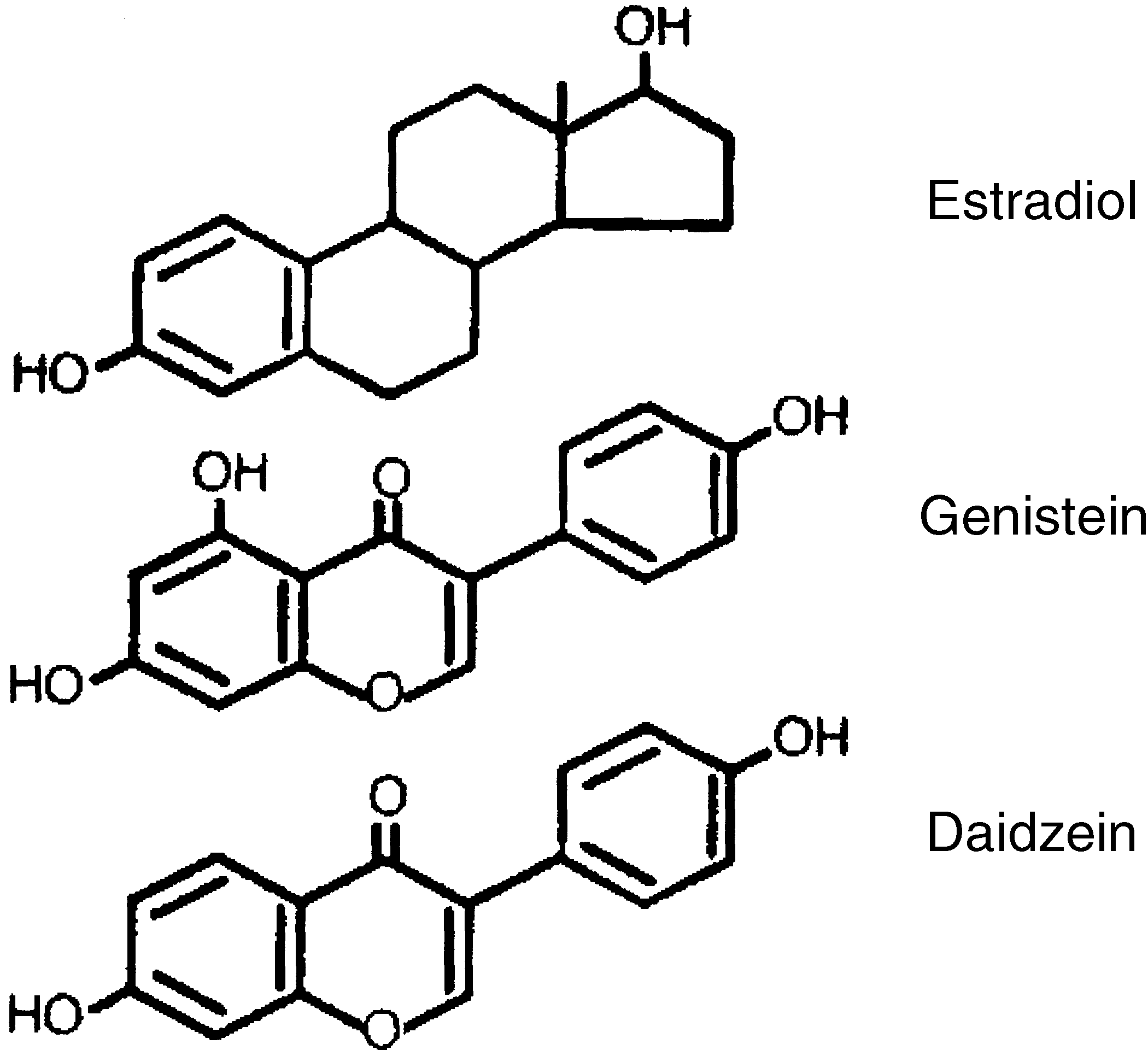 a reduction in vascular adhesion molecules by endothelial cellsÐ
a theoretically bene®cial effect (Simoncini and Genazzani, 2000).
a reduction in vascular adhesion molecules by endothelial cellsÐ
a theoretically bene®cial effect (Simoncini and Genazzani, 2000).