Chemoprevention of Colorectal Cancer by Aspirin:
SAUD SULEIMAN,* DOUGLAS K. REX,‡ and AMNON SONNENBERG**Department of Veterans Affairs Medical Center, Albuquerque, New Mexico; and ‡Division of Gastroenterology, Department of Medicine,Indiana University School of Medicine, Indianapolis, Indiana
diagnostic test, alternative strategies to prevent colorec-
tal cancer have been sought. Regular intake of nonste-roidal anti-inflammatory drugs (NSAIDs), including as-
Background & Aims: The aim of the study is to compare
pirin, was found to cause regression of colonic polyps and
the cost-effectiveness of aspirin and colonoscopy in the
reduce the risk for developing colorectal cancer by 40%–
prevention of colorectal cancer. Methods: A Markov pro-
50%.8–19 Chemoprevention of colorectal cancer by means
cess is used to follow a hypothetical cohort of 100,000
of regular intake of aspirin or other NSAIDs may repre-
subjects aged 50 years until death. Four strategies arecompared: (1) no intervention, (2) colonoscopy once per
sent a viable option to reduce morbidity and mortality
10 years and every 3 years in subjects with polyps, (3)
from colorectal cancer. NSAIDs are associated with mul-
chemoprevention with 325 mg of daily aspirin, and (4)
tiple side effects, involving predominantly hemostasis
combination of the second and third strategies. The
and the gastrointestinal (GI) tract, which can lead to
various strategies are compared calculating incremental
excessive consumption health care resources.20–23 Before
cost-effectiveness ratios (ICERs). Results: The expected
introducing a strategy of cancer prevention through
number of colorectal cancers is 5904 per 100,000 sub-
NSAIDs, therefore, one has to weigh the benefits of
jects. Colonoscopy prevents 4428 colorectal cancers
chemoprevention against their costly side effects. The
and saves 7951 life-years at an ICER of $10,983 per
aim of the present study is to compare the cost-effective-
life-year saved compared with no intervention. Aspirin
ness of regular aspirin intake with colonoscopy once per
prevents 2952 colorectal cancers and saves 5301 life-
10 years for the prevention of colorectal cancer. Aspirin
years at an ICER of $47,249 per life-year saved com-
is chosen as a representative medication for the class of
pared with no intervention. The cost of aspirin therapy
NSAIDs because it is the most widely used and the least
plus management of aspirin-related complications wasreported to be $172 per year per patient. Varying the
annual aspirin-related costs between $50 and $200results in ICER changes between $4617 and $57,080,
with the 2 strategies breaking even at $70. Applyingaspirin chemoprevention plus colonoscopy screening
The cost-effectiveness of 3 cancer prevention strategies
concomitantly yields an ICER of $227,607 per life-year
are compared with a strategy of nonprevention. A previously
saved compared with screening colonoscopy alone.
published model of a Markov process is used to follow a
Conclusion: As compared with colonoscopy once per 10
hypothetical cohort of 100,000 persons aged 50 years until
years, the use of aspirin to prevent colorectal cancer
death.5 A cohort of 50-year-old persons is subjected to the
saves fewer lives at higher costs. The high complication
following 4 prevention strategies: (1) no intervention; (2) 1
cost and the lower efficacy of aspirin render screening
colonoscopy every 10 years or, in case of adenomatous polyps,
colonoscopy a more cost-effective strategy to prevent
every 3 years until polyps are no longer found; (3) no colonos-
copy but chemoprevention with 325 mg of daily aspirin; and(4) combination of the second and third strategy, that is,colonoscopy every 10 or 3 years plus daily aspirin. As in the
Colorectal cancer ranks second among the causes of previous model, the time frame of the analysis is divided into
cancer death in the United States.1 More than 95%
equal increments of 1 year, during which the subjects transi-
of colorectal cancer arises from adenomatous polyps.2Colonoscopy by way of polypectomy reduces colorectal
Abbreviations used in this paper: ACER, average cost-effectiveness
cancer, and this modality has been established as a cost-
ratio; GI, gastrointestinal; ICER, incremental cost-effectiveness ratio.
2002 by the American Gastroenterological Association
effective method for the prevention of colorectal can-
cer.3–7 Because colonoscopy is an expensive and invasive
Individual transitions between different states are associated
with costs, the costs being estimated from the perspective of athird party payer. The costs of colorectal cancer therapy,colonoscopy, polypectomy, and their related complications relyon published cost data and Medicare reimbursements in theyear 2000.5 Published cost estimates for the medical care ofsubjects with colorectal cancer range between $25,000 and$45,000.7,30–32 These costs include expenditures for diagnosis,surgery, radiation, and chemotherapy. We use the most recentdata available from Lee et al.32 Smalley et al.22 published dataon the excess costs from GI disease associated with NSAIDs,comparing a cohort of 46,000 nonusers with 5,000 regular
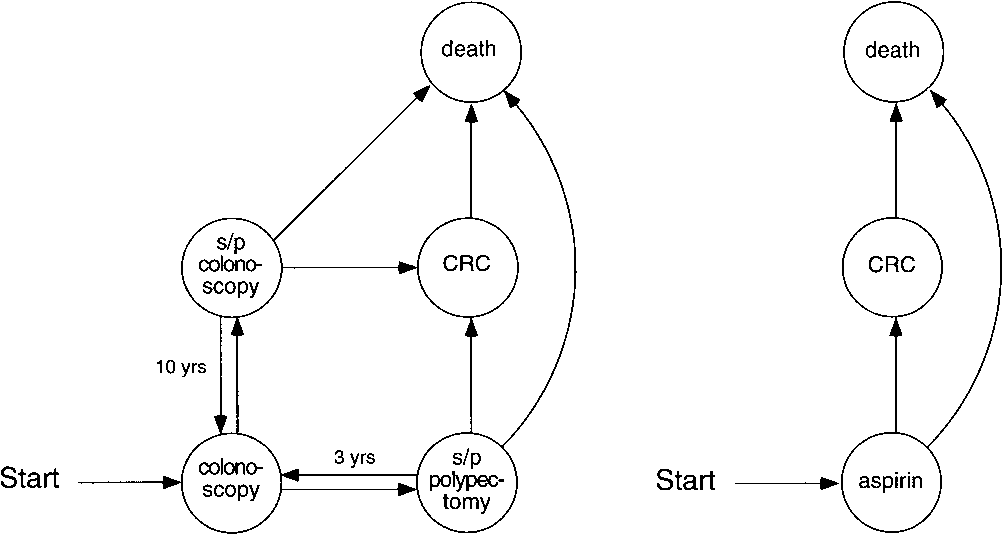
Figure 1. (Left) A Markov state diagram of screening for colorectalcancer (CRC) by repeat colonoscopy every 10 years in case of normal
users. Assuming a 3% interest rate, their 1989 costs data were
colonoscopy or every 3 years after polypectomy. (Right) A Markov
updated to an average net present value of $154 per patient per
state diagram for CRC prophylaxis using daily aspirin. The arrows
year. Adding the annual drug cost of $18 spent on 325 mg of
symbolize transitions between the various states. s/p, status post.
aspirin per day, the total cost of chemoprevention amounts to$172 per patient per year. These estimates were used as
tion from one state of health to another. The Markov chains
baseline cost. Similar cost data are also available from other
underlying the preventive strategies are depicted in Figure 1.
sources. Based on 527 Medicaid patients treated over 786
In the colonoscopy model, all subjects start with a colonoscopy
treatment quarters with NSAIDs, Bloom21 estimated that in
at age 50. Subjects can then transition among 4 different
1982, $66 was spent per quarter on adverse GI drug reactions.
states, that is, (1) a state after a negative colonoscopy without
These numbers translate to $449 per patient per year in 2000.
polyps, (2) a state after colonoscopy plus polypectomy, (3) a
Lastly, in a Canadian population of 5,268 NSAID users, GI
state after developing colorectal cancer, and (4) death from
adverse events during a 2-year follow-up cost $134 (1995
colorectal cancer or other causes. In case of aspirin prophylaxis,
Canadian dollars), resulting in a current estimate of $78 per
all subjects are started on a daily dose of aspirin. Subsequently,
year.23 Although the absolute Canadian price levels for all
they can transition among 3 different states, that is, (1) remain
medical interventions were lower than in the United States,
disease-free on aspirin prophylaxis, (2) develop a colorectal
the percentage of GI-related costs of NSAID therapy was
cancer, or (3) die from colorectal cancer or other causes. The
found to be similar in both countries.21–23 In a sensitivity
various Markov models of the 4 strategies for cancer preventionare simulated on Excel spreadsheets (Microsoft, Redmond,
Table 1. Transitions and Costs Used in the Markov Model
The transitions among the various states are governed by
chance, the annual transition rates being shown in Table 1. To
facilitate comparison with other strategies of cancer preven-
tion, the same transition probabilities as in previous models of
colorectal cancer are used.5,24 The Markov model uses an
Efficacy of colonoscopy in preventing CRC
annual 1% incidence polyp rate to calculate the number of
polypectomies and repeat colonoscopies after polypectomy.25
The annual age-specific incidence rate of colorectal cancer is
taken from published statistics of the Surveillance, Epidemi-
ology, and End Results Program.26 The population in each
state is also subjected to natural attrition by the annual age-
specific death rate of the US population.27
Colonoscopy, polypectomy, or aspirin prevent colorectal
cancer by reducing its incidence. In addition, early detection of
colorectal cancer through colonoscopy lowers cancer-related
mortality. The National Polyp Study3 showed an efficacy of
colonoscopy in reducing the incidence of colorectal cancer
ranging between 76% and 90%. As other studies have sug-
gested an efficacy of only 49% to 59%,4,28,29 a median value of
75% is chosen as a baseline rate for the present analysis with
a range of 50%–75% used in a subsequent sensitivity analysis.
The 50% efficacy of aspirin has been reported in preventing
colorectal cancer.8–10 In the sensitivity analysis, this efficacy
NOTE. Expenditures include professional fees and facility costs.
Table 2. Outcome of Various Programs to Prevent Colorectal Cancer
NOTE. Numbers in the table relate to a cohort of 100,000 persons aged 50 and followed on the average for 28.5 years. Future life-years savedand future costs are discounted using an annual rate of 3%. CRC, colorectal cancer; ICER, incremental cost-effectiveness ratio of costs per saved life-year.
analysis, the baseline cost of chemoprevention is varied be-
50% efficacy prevents 2,952 colorectal cancers and saves
5,301 life-years. The ACERs and ICERs are both larger
Effectiveness of screening is measured in terms of life-years
than those of colonoscopy. Chemoprevention as an added
saved through prevention of colorectal cancer and improved
measure to colonoscopy is assumed to prevent an addi-
survival of earlier cancer stages. The amount of life-years saved
tional 50% of all cancers failed to prevent through
through prevention corresponds to the difference in life-years
colonoscopy alone. The ACERs and ICERs are smaller
lost from cancer-related deaths between each 2 Markov models,
than those of chemoprevention alone, but much larger
1 with and 1 without a preventive strategy. All costs arising
than those of colonoscopy alone. The ICER of combined
from screening colonoscopy, chemoprevention, and the care ofcolorectal cancer and all future life-years saved are discounted
chemoprevention plus colonoscopy, compared with
at an annual rate of 3%.33 The average cost-effectiveness ratio
colonoscopy alone, exceeds $200,000 per life-year saved
(ACER) corresponds to the total costs in the patient cohort
(Table 2). On the other hand, if aspirin prevention was
divided by the total amount of life-years saved. The incremen-
already implemented in the general population, the ad-
tal cost-effectiveness ratio (ICER) compares each screening
dition of 1 colonoscopy per 10 years to prevent even more
strategy with the previous less effective option, including a
deaths from colorectal cancers would result in a relatively
strategy of no screening. The ICER is calculated as the differ-
low ICER of $34,836 compared with chemoprevention
ence in costs divided by the corresponding difference in effec-
alone. In other words, chemoprevention on top of screen-
ing colonoscopy is not cost-effective, whereas screeningcolonoscopy on top of chemoprevention still represents a
Table 2 shows the outcomes of modeling 4 dif-
Figure 2 shows the results of a sensitivity analysis
ferent strategies to prevent colorectal cancer. Without
varying the cost of chemoprevention and the preventive
any prevention, the expected number of colorectal can-
efficacy of both colonoscopy and daily aspirin. Under
cers in a cohort of 100,000 subjects is 5,904, and the
baseline conditions, the costs of chemoprevention need to
only costs incurred relate to the care of colorectal cancer.
fall below $70 to become more cost-effective than
Colonoscopy once per 10 years at 75% efficacy prevents
colonoscopy. Even under the assumption of highly effi-
4,428 colorectal cancers and saves 7,951 life-years. The
cacious (75%) chemoprevention and a comparatively in-
cost of colonoscopy screening in this cohort amounts to
efficacious (50%) colonoscopy, the threshold is only
$223,780,829. This includes facility fees, physician fees,
$150. This value still lies below the actual costs of $172
and the costs incurred for the care of associated compli-
cations. The ACER is $28,143 per life-year saved. The
Under baseline assumptions, colonoscopy combined
ICER is calculated at $10,983 per life-year saved when
with chemoprevention prevents 87.5% of all colorectal
compared with no intervention. Chemoprevention at
cancers. In a second sensitivity analysis, the combined
sent a conceptually interesting but presently not cost-effective strategy. The relatively large costs associatedwith the adverse effects of NSAIDs render 1 colonoscopyevery 10 years a more cost-effective alternative. A com-bined prevention strategy using both colonoscopy plusdaily aspirin could increase the overall effectiveness of acancer prevention program. However, the incrementalcost-effectiveness of chemoprevention combined withcolonoscopy alone would be rather high, costing morethan $100,000 per additional life-year saved as comparedwith colonoscopy alone.
In the assessment of cost-effectiveness, our analysis
was based on the comparison of 4 management options,
Figure 2. Influence of cost and efficacy of chemoprevention on itsICER compared with no prevention. The intersection between the lines
that is, no prevention, colonoscopy alone, aspirin alone,
of colonoscopy and chemoprevention delineates the threshold costs
and combination of colonoscopy plus aspirin. The argu-
of chemoprevention to become less or more expensive than colonos-
ments against or in favor of a particular strategy are based
on the comparison of 2 ICERs rather than their absolutevalues. In terms of absolute values, however, all ICERsfall within a range that is still considered economically
efficacy is varied between 50% and 100%. The lower
feasible. To put values of ICERs in perspective, it has
value corresponds to the efficacy of colonoscopy alone
become customary to compare the cost-effectiveness of
with a 0% contribution of chemoprevention, whereas
various health care interventions by “league tables.”35
100% corresponds to a 25% or 50% efficacy of chemo-
Different types of medical procedures and therapies are
prevention added to a 75% or 50% baseline efficacy of
ranked in a league table by their cost-effectiveness. For
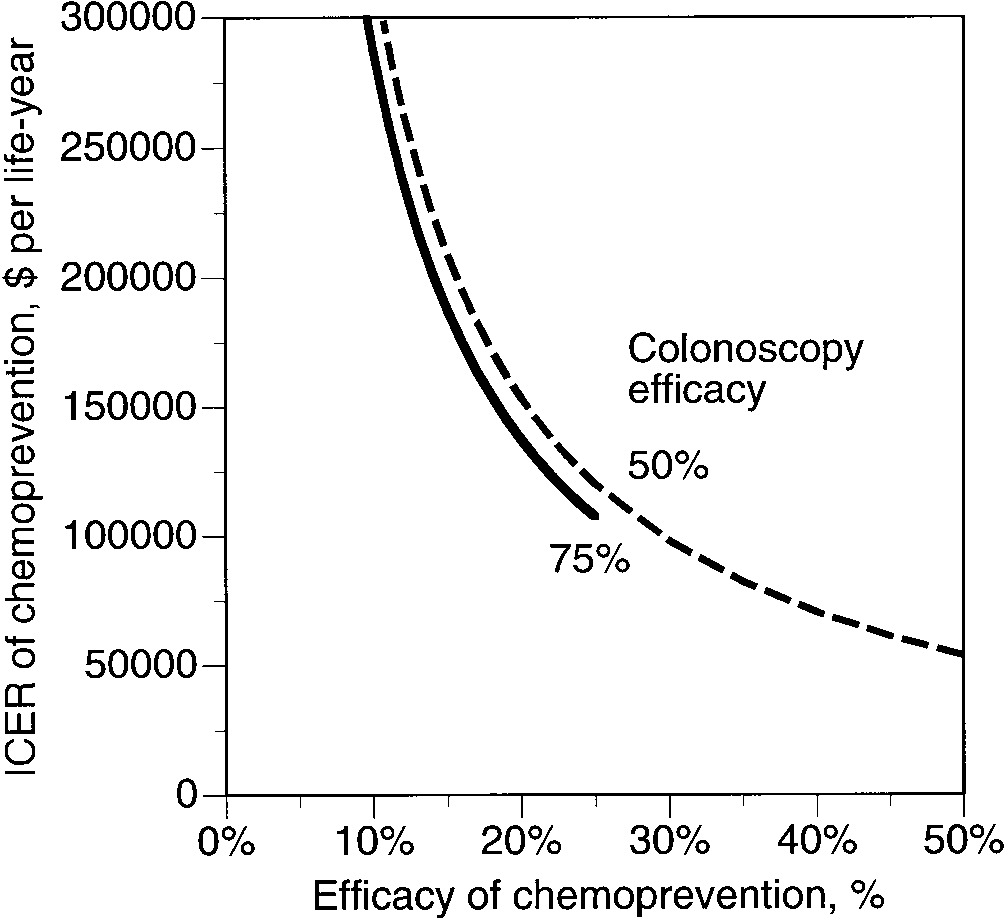
colonoscopy alone. On the x-axis of Figure 3, the addi-
instance, it has been estimated that endoscopic surveil-
tional efficacy of chemoprevention (beyond the baseline
lance of Barrett’s esophagus would cost $98,000 per
efficacy of colonoscopy) is varied between 0% and 50%.
quality adjusted life-year gained. Cervical cancer screen-
The 2 curves represent 2 baseline efficacy rates of
ing may cost as much as $250,000 per life saved.36
colonoscopy. The lower curve representing 75% baseline
The present decision analysis uses a previously pub-
efficacy of colonoscopy ends at 25% efficacy of chemo-
lished model of a Markov process to assess the impact of
prevention, because otherwise the joint efficacy would
various screening strategies on the prevention of colorec-
rise beyond 100%. As the figure shows, a higher addedefficacy of chemoprevention makes it a more cost-effec-tive option. If endoscopy and aspirin combined were ableto prevent all cancers, the incremental cost-effectivenessof aspirin would vary between $50,000 and $100,000,dependent on the preventive efficacy of colonoscopyalone. Such expectations seem unrealistic, and with moremoderate success of chemoprevention, its cost-effective-ness ratio (as compared with colonoscopy alone) is morelikely to fall into the $100,000 to $200,000 range. Thisholds true even if due to the reduced incidence rate ofpolyps under chemoprevention, the interval of surveil-lance colonoscopy after polypectomy is increased to 5years.
The notion is quite appealing that by taking
a daily aspirin pill, one could reduce the risk of colo-rectal cancer and avoid unpleasant, repeated, and costlycolonoscopy. As the present analysis shows, unfortu-
Figure 3. Influence of chemoprevention efficacy on the ICER of che-
nately, chemoprevention of colorectal cancer may repre-
moprevention plus colonoscopy compared with colonoscopy alone.
tal cancer.5 As compared with colonoscopy, the previous
To reduce the side effects of NSAIDs, new specific
model showed screening by annual fecal occult blood
cyclooxygenase-2 inhibitors have been developed.37,38
testing to cost less, but also save fewer life-years. A
Results from laboratory studies suggest that, like con-
screening strategy based on flexible sigmoidoscopy every
ventional NSAIDs, these newer compounds with a lesser
5 or 10 years was not cost-effective compared with the
GI toxicity may also protect against colorectal can-
other 2 screening methods. Because under baseline as-
cer.39–41 The cost saved by the drugs’ safer profile and
sumptions, screening through fecal occult blood testing
lesser side effects, however, becomes spent on the drug
and decennial colonoscopy were comparable, fecal occult
itself. A year’s supply of daily 100 mg celecoxib (Cele-
blood testing was not again included in this study. The
brex; Searle, Skokie, IL) costs about $600. These costs
incidence rates of colon polyps and the length of the time
exceed by far the threshold for chemoprevention to be-
intervals between each 2 endoscopic examinations had
come a cost-effective alternative. It is conceivable, how-
already been shown to exert a lesser influence on the
ever, that in the future other and cheaper drugs with few
outcome of the analysis. The present analysis also relies
or no adverse effects on the GI tract will make chemo-
on other results of the foregoing cost-effectiveness study.
prevention of colorectal cancer a cost-effective option.
Because low compliance of colonoscopy, for instance,
Several economic analyses have dealt with the use of
reduces both the overall number of cancers prevented and
aspirin in the secondary prevention of recurrent myocar-
the total costs in a linear fashion, it does not affect the
dial infarction, transient ischemic attack, or stroke. In
cost-effectiveness ratio of colonoscopy. A low compliance
addition to being clinically efficacious, these studies sug-
rate of aspirin intake would reduce its efficacy and render
gest that aspirin therapy also represents a cost-effective
it even less cost-effective than the other means of cancer
management option.42–44 In patients who are already put
on aspirin to prevent recurrent cardiovascular disease,
Chemoprevention alone is not cost-effective compared
therefore, the prevention of colorectal cancer adds to the
with colonoscopy alone for 2 reasons. The first reason
overall cost-effectiveness of the preventive strategy.
relates to the overall high annual costs associated with
Three large randomized clinical trials have shown that
regular intake of nonsteroidals. The common occurrence
aspirin is efficacious in the primary prevention of cardio-
of adverse effects during the treatment with NSAIDs
vascular disease.45–47 It reduces the overall occurrence of
renders this drug class costly, even if the expenses for the
cardiovascular death, nonfatal myocardial infarction, and
drug itself may appear relatively cheap. The annual costs
stroke by 15%–30%. These results were achieved in
of chemoprevention, including the expenditures for the
populations of hypertensive patients or patients who
NSAIDs and their side effects, would need to fall below
presented with an increased risk for cardiovascular dis-
a threshold that seems by today’s standards unrealisti-
ease. Chemoprevention in the general population would
cally low. The second influence to determine the out-
be associated with a lesser benefit, but excess GI bleeding
come of chemoprevention relates to its efficacy in pre-
and hemorrhagic cerebrovascular events. It is currently
venting colorectal cancer. Even if chemoprevention alone
being debated among cardiologists and public health
were as efficacious as colonoscopy and averted, for in-
researchers whether, in the general population as well,
stance, 75% of all colorectal cancers, its overall annual
the benefit of aspirin outweighs its adverse effects.48,49
costs would need to be less than $100 to $150 to become
Data derived through meta-analysis and modeling sug-
a cost-effective alternative. Again, such assumptions
gest that primary prevention of cardiovascular disease
seem overly optimistic. Chemoprevention represents
may be cost-effective only in subpopulations with an
only a viable, yet expensive means to reduce the occur-
increased risk.49–51 Because cardiovascular disease is
rence of colorectal cancer if added to an endoscopic
much more frequent than colorectal cancer, the issue of
screening program. Rather than estimate the possible
cancer prevention becomes completely overwhelmed by
occurrence of various GI adverse events and the health
the cardiovascular side. From a strictly cancer-related
care expenditures associated with individual complica-
perspective, however, chemoprevention alone does not
tions, the present model relies on actual average cost
represent a cost-effective alternative to colonoscopy. If
data. The cost data from several large patient populations
primary cardiovascular prevention with aspirin were al-
treated with NSAIDs fall within the same order of
ready used in the general population, the added screen-
magnitude and support the contention that similar costs
ing through colonoscopy would still represent a cost-
could be expected if chemoprevention were to be imple-
effective strategy, because it would save many more lives
We conclude that in the prevention of colorectal can-
rectal polyps in familial adenomatous polyposis. Gastroenterol-
cer, colonoscopy once per 10 years saves more lives at
19. Spagnesi MT, Tonelli F, Dolara P, Caderni G, Valanzano R, Anas-
lower overall costs than daily aspirin. The high cost of
tasi A, Bianchini F. Rectal proliferation and polyp occurrence in
chemoprevention and its relatively low efficacy render
patients with familial adenomatous polyposis after sulindac
screening colonoscopy the more cost-effective option to
treatment. Gastroenterology 1994;106:362–366.
20. Trujilllo MA, Garewal HS, Sampliner RE. Nonsteroidal anti-inflam-
reduce morbidity and mortality related to colorectal
matory agents in chemoprevention of colorectal cancer. At what
cancer. Chemoprevention used in addition to endoscopic
cost? Dig Dis Sci 1994;39:2260 –2266.
screening provides a viable strategy to save more lives
21. Bloom BB. Direct medical costs of disease and gastrointestinal
than through colonoscopy screening alone, although this
side effects during treatment for arthritis. Am J Med 1988;84(suppl 2A):20 –24.
benefit is associated with an ICER that may be prohib-
22. Smalley WE, Griffin MR, Fought RL, Ray WA. Excess cost from
itively high for most health-care systems.
gastrointestinal disease associated with nonsteroidal anti-in-flammatory drugs. J Gen Intern Med 1996;11:461– 469.
23. Rahme E, Joseph L, Kong SX, Watson DJ, LeLorier J. Gastroin-
testinal health care resource use and costs associated with
1. American Cancer Society. Cancer facts and figures, 1998. Publi-
nonsteroidal antiinflammatory drugs versus acetaminophen. Ret-
cation No 5008.98. Atlanta, GA: American Cancer Society, 1998.
rospective cohort study of an elderly population. Arthritis Rheum
2. Peipins LA, Sandler RS. Epidemiology of colorectal adenomas.
` F. Cost-effectiveness of a single colonos-
3. Winawer SJ, Zauber AG, Ho MN, O’Brien MJ, Ho MN, Gottlieb LS,
copy in screening for colorectal cancer. Arch Intern Med 2001;in
Sternberg SS, Waye JD, Schapiro M, Bond JH, Panish JF. Preven-
tion of colorectal cancer by colonoscopic polypectomy. The Na-
25. Williams A, Balasooria B, Day D. Polyps and cancer of the large
tional Polyp Study Workgroup. N Engl J Med 1993;329:1977–
bowel: a necropsy study in Liverpool. Gut 1982;23:835– 842.
26. Ries LAG, Kosary CL, Hankey BF, Miller BA, Harras A, Edwards BK
¨ller AD, Sonnenberg A. Protection by endoscopy against death
(eds). SEER Cancer Statistics Review, 1973-1994, National Can-
from colorectal cancer: a case control study among veterans.
cer Institute. NIH Publication No. 97-2789. Bethesda, MD: NIH,
Arch Intern Med 1995;155:1741–1748.
` F, Inadomi JM. The cost-effectiveness of
27. National Center for Health Statistics. US decennial life tables for
colonoscopy in screening for colorectal cancer. Ann Intern Med
1989-91. DHHS Publication No. PHS-98-1150-1, Volume 1, No 1.
Hyattsville, MD: U.S. Department of Health and Human Services,
6. Eddy DM. Screening for colorectal cancer. Ann Intern Med 1990;
¨ller AD, Sonnenberg A. Prevention of colorectal cancer by
7. Lieberman DA. Cost-effectiveness model for colorectal cancer
flexible endoscopy: a case control study of 32,702 veterans. Ann
screening. Gastroenterology 1995;109:1781–1790.
8. Kune GA, Kune S, Watson FL. Colorectal cancer risk, chronic
29. Selby JV, Friedman GD, Quesenberry CP, Weiss NS. A case
illnesses, operations, and medications: case control results from
control study of screening sigmoidoscopy and mortality from
the Melbourne colorectal cancer study. Cancer Res 1988;48:
colorectal cancer. N Engl J Med 1992;326:653– 657.
30. Winawer SJ, Fletcher RH, Miller L, Godlee F, Stolar MH, Mulrow
9. Thun MJ, Namboodiri MM, Heath CW Jr. Aspirin use and reduced
CD, Woolf SH, Glick SN, Ganiats TG, Bond JH, Rosen L, Zapka JG,
risk of fatal colon cancer. N Engl J Med 1991;325:1593–1596.
Olsen SJ, Giardiello FM, Sisk JE, Van Antwerp R, Brown-Davis C,
10. Greenberg ER, Baron JA, Freeman DH Jr, Mandel JS, Haile R.
Marciniak DA, Mayer RJ. Colorectal cancer screening: clinical
Reduced risk of large bowel adenomas among aspirin users.
guidelines and rationale. Gastroenterology 1997;112:594 – 642.
J Natl Cancer Inst 1993;85:912–916.
31. Provenzale D, Wong JB, Onken JE, Lipscomb J. Performing a
11. Sandler RS, Galanko JC, Murray SC, Helm JF, Woosley JT. Aspirin
cost-effectiveness analysis: surveillance of patients with ulcer-
and non-steroidal anti-inflammatory agents and risk for colorectal
ative colitis. Am J Gastroenterol 1997;93:872– 880.
adenomas. Gastroenterology 1998;114:441– 447.
32. Lee JG, Vigil HT, Leung JW. The hospital costs for diagnosis and
12. Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Ascherio A,
treatment of colorectal cancer (abstr). Gastrointest Endosc
Willett WC. Aspirin use and the risk for colorectal cancer and
adenoma in male health professionals. Ann Intern Med 1994;121:241–246.
33. Weinstein MC, Stason WB. Foundations of cost-effectiveness for
13. Giovannucci E, Egan KM, Hunter DJ, Stampfer MJ, Colditz GA,
health and medical practices. N Engl J Med 1977;296:716 –721.
Willett WC, Speizer FE. Aspirin and the risk of colorectal cancer in
34. Siegel JE, Weinstein MC, Torrance GW. Reporting cost-effective-
women. N Engl J Med 1995;333:609 – 614.
ness studies and results. In: Gold MR, Siegel JE, Russel LB,
14. Suh O, Mettlin C, Petrelli NJ. Aspirin use, cancer, and polyps of
Weinstein MC, eds. Cost-effectiveness in health and medicine.
the large bowel. Cancer 1993;72:1171–1177.
New York: Oxford University Press, 1996:276 –303.
15. DuBois RN, Giardiello FM, Smalley WE. Nonsteroidal anti-inflam-
35. Drummond MF, O’Brien B, Stoddart GL, Torrance GW. Methods
matory drugs, eicosanoids, and colorectal cancer prevention.
for the economic evaluation of health care programmes. 2nd ed.
Gastroenterol Clin North Am 1996;25:773–791.
New York: Oxford University Press, 1997.
16. DuBois RN, Smalley WE. Cyclooxygenase, NSAIDs, and colorectal
36. Provenzale D, Schmitt C, Wong JB. Barrett’s esophagus: a new
cancer. J Gastroenterol 1996;31:898 –906.
look at surveillance based on emerging estimates of cancer risk.
´ JM, Rubio E, Planas R, Tarrech JM, Bordas JM.
Am J Gastroenterol 1999;94:2043–2053.
Effects of long-term sulindac therapy on colonic polyposis. Ann
37. Laine L, Harper S, Simon T, Bath R, Johanson J, Schwartz H,
Stern S, Quan H, Bolognese J. A randomized trial comparing the
18. Labayle D, Fischer D, Vielh P, Drouhin F, Pariente A, Bories C,
effect of rofecoxib, a cyclooxygenase 2-specific inhibitor, with
Duhamel O, Trousset M, Attali P. Sulindac causes regression of
that of ibuprofen on the gastroduodenal mucosa of patients with
osteoarthritis. Rofecoxib Osteoarthritis Endoscopy Study Group.
Framework. Thrombosis prevention trial: randomised trial of low-
Gastroenterology 1999;117:776 –783.
intensity oral anticoagulation with warfarin and low-dose aspirin
38. Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T, Whel-
in the primary prevention of ischaemic heart disease in men at
ton A, Makuch R, Eisen G, Agrawal NM, Stenson WF, Burr AM,
increased risk. Lancet 1998;351:233–241.
Zhao WW, Kent JD, Lefkowith JB, Verburg KM, Geis GS. Gastro-
46. Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D,
intestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory
Julius S, Menard J, Rahn KH, Wedel H, Westerling S. Effects of
drugs for osteoarthritis and rheumatoid arthritis: the CLASS
intensive blood-pressure lowering and low-dose aspirin in pa-
study: a randomized controlled trial. Celecoxib Long-term Arthritis
tients with hypertension: principal results of the Hypertension
Safety Study. JAMA 2000;284:1247–1255.
Optimal Treatment (HOT) randomised trial. HOT Study Group.
39. Boolbol SK, Dannenberg AJ, Chadburn A, Martucci C, Guo XJ,
Ramonetti JT, Abreu-Goris M, Newmark HL, Lipkin ML, DeCosse
47. Collaborative Group of the Primary Prevention Project (PPP). Low-
JJ, Bertagnolli MM. Cyclooxygenase-2 overexpression and tumor
dose aspirin and vitamin E in people at cardiovascular risk: a
formation are blocked by sulindac in a murine model of familial
randomised trial in general practice. Lancet 2001;357:89 –95.
adenomatous polyposis. Cancer Res 1996;56:2256 –2260.
48. Hebert PR, Hennekens CH. An overview of the 4 randomized trials
40. Sheng H, Shao J, Kirkland SC, Isakson P, Coffey RJ, Morrow J,
of aspirin therapy in the primary prevention of vascular disease.
Beauchamp RD, DuBois RN. Inhibition of human colon cancer
Arch Intern Med 2000;160:3123–3127.
cell growth by selective inhibition of cyclooxygenase-2. J Clin
49. Sanmuganathan PS, Ghahramani P, Jackson PR, Wallis EJ, Ram-
say LE. Aspirin for primary prevention of coronary heart disease:
41. Kawamori T, Rao CV, Seibert K, Reddy BS. Chemopreventive
safety and absolute benefit related to coronary risk derived from
activity of celecoxib, a specific cyclooxygenase-2 inhibitor,
meta-analysis of randomised trials. Heart 2001;85:265–271.
against colon carcinogenesis. Cancer Res 1998;58:409 – 412.
50. Augustovski FA, Cantor SB, Thach CT, Spann SJ. Aspirin for
42. Shah H, Gondek K. Aspirin plus extended-release dipyridamole or
primary prevention of cardiovascular events. J Gen Intern Med
clopidogrel compared with aspirin monotherapy for the preven-
tion of recurrent ischemic stroke: a cost-effectiveness analysis.
51. Troche CJ, Tacke J, Hinzpeter B, Danner M, Lauterbach KW.
Cost-effectiveness of primary and secondary prevention in car-
43. Ebrahim S. Cost-effectiveness of stroke prevention. Brit Med Bull
diovascular disease. Eur Heart J 1999;19(suppl C):C59 – 65.
44. Sarasin FP, Gaspoz JM, Bounameaux H. Cost-effectiveness of
new antiplatelet regimes used as secondary prevention of stroke
Received June 1, 2001. Accepted August 2, 2001.
or transient ischemic attack. Arch Intern Med 2000;160:2773–
Address requests for reprints to: Amnon Sonnenberg, M.D., M.Sc.,
Department of Veterans Affairs Medical Center 111F, 1501 San Pedro
45. The Medical Research Council’s General Practice Research
Drive SE, Albuquerque, New Mexico 87108. e-mail: [email protected].
IBEW NECA Sound and Communications Trust Fund Health Reimbursement Account (HRA): What’s Eligible? The IRS defines eligible health care expenses as amounts paid for the diagnosis, cure, mitigation or treatment of a disease, and for treatments affecting any part or function of the body. The expenses must be primarily to alleviate a physical or mental condition or illness. This list is not
Tejcukortól mentes termékek Ez a terméklista szakembereknek: orvosoknak, dietetikusoknak, védőnőknek táplálékintoleranciában szenvedő betegeknek nyújtott tanácsadásban, a rendelkezésre ál ó élelmiszerekből a megfelelőek kiválasztásában. A terméklistát a rászorulók az Adatbanktól közvetlenül is megrendelhetik. A füzetcsomag a kilenc leggyakoribb al ergén komp
 Individual transitions between different states are associated
with costs, the costs being estimated from the perspective of athird party payer. The costs of colorectal cancer therapy,colonoscopy, polypectomy, and their related complications relyon published cost data and Medicare reimbursements in theyear 2000.5 Published cost estimates for the medical care ofsubjects with colorectal cancer range between $25,000 and$45,000.7,30–32 These costs include expenditures for diagnosis,surgery, radiation, and chemotherapy. We use the most recentdata available from Lee et al.32 Smalley et al.22 published dataon the excess costs from GI disease associated with NSAIDs,comparing a cohort of 46,000 nonusers with 5,000 regular
Figure 1. (Left) A Markov state diagram of screening for colorectalcancer (CRC) by repeat colonoscopy every 10 years in case of normal
users. Assuming a 3% interest rate, their 1989 costs data were
colonoscopy or every 3 years after polypectomy. (Right) A Markov
updated to an average net present value of $154 per patient per
state diagram for CRC prophylaxis using daily aspirin. The arrows
year. Adding the annual drug cost of $18 spent on 325 mg of
symbolize transitions between the various states. s/p, status post.
Individual transitions between different states are associated
with costs, the costs being estimated from the perspective of athird party payer. The costs of colorectal cancer therapy,colonoscopy, polypectomy, and their related complications relyon published cost data and Medicare reimbursements in theyear 2000.5 Published cost estimates for the medical care ofsubjects with colorectal cancer range between $25,000 and$45,000.7,30–32 These costs include expenditures for diagnosis,surgery, radiation, and chemotherapy. We use the most recentdata available from Lee et al.32 Smalley et al.22 published dataon the excess costs from GI disease associated with NSAIDs,comparing a cohort of 46,000 nonusers with 5,000 regular
Figure 1. (Left) A Markov state diagram of screening for colorectalcancer (CRC) by repeat colonoscopy every 10 years in case of normal
users. Assuming a 3% interest rate, their 1989 costs data were
colonoscopy or every 3 years after polypectomy. (Right) A Markov
updated to an average net present value of $154 per patient per
state diagram for CRC prophylaxis using daily aspirin. The arrows
year. Adding the annual drug cost of $18 spent on 325 mg of
symbolize transitions between the various states. s/p, status post.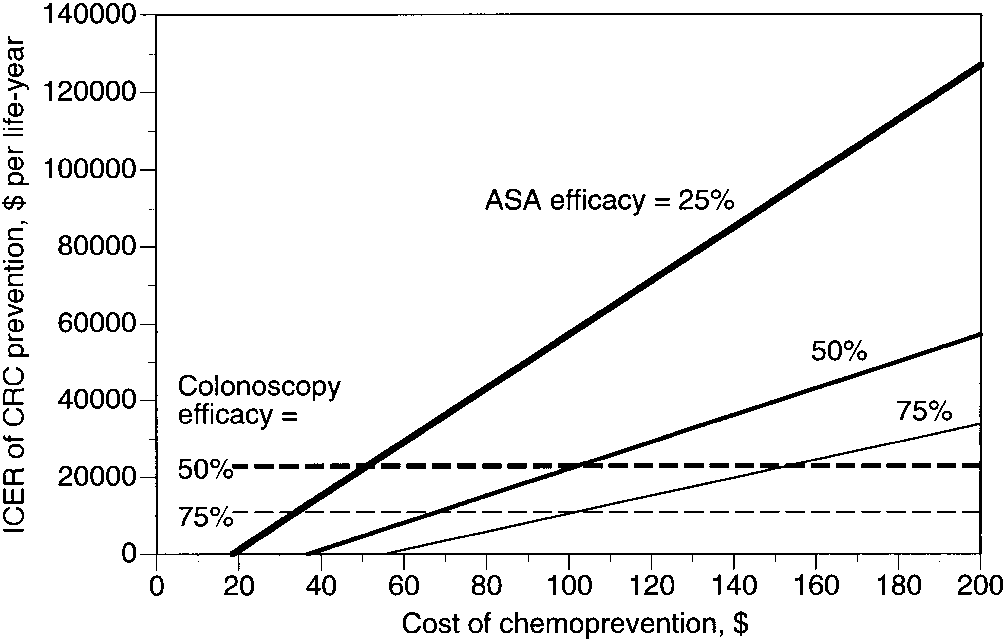
 sent a conceptually interesting but presently not cost-effective strategy. The relatively large costs associatedwith the adverse effects of NSAIDs render 1 colonoscopyevery 10 years a more cost-effective alternative. A com-bined prevention strategy using both colonoscopy plusdaily aspirin could increase the overall effectiveness of acancer prevention program. However, the incrementalcost-effectiveness of chemoprevention combined withcolonoscopy alone would be rather high, costing morethan $100,000 per additional life-year saved as comparedwith colonoscopy alone.
sent a conceptually interesting but presently not cost-effective strategy. The relatively large costs associatedwith the adverse effects of NSAIDs render 1 colonoscopyevery 10 years a more cost-effective alternative. A com-bined prevention strategy using both colonoscopy plusdaily aspirin could increase the overall effectiveness of acancer prevention program. However, the incrementalcost-effectiveness of chemoprevention combined withcolonoscopy alone would be rather high, costing morethan $100,000 per additional life-year saved as comparedwith colonoscopy alone.