Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Pii: s1542-3565(04)00288-5
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:656 – 664
Effectiveness of Proton Pump Inhibitors in Nonerosive Reflux
BONNIE B. DEAN,* ANACLETO D. GANO, JR.,* KEVIN KNIGHT,* JOSHUA J. OFMAN,*,‡ andRONNIE FASS§*Cerner Health Insights, Beverly Hills, California; ‡Cedars-Sinai Medical Center, Department of Medicine, Los Angeles, California;and §Southern Arizona VA Health Care System, Tucson, Arizona
Background & Aims: Little information is available
injury.2–5 Attention recently has shifted to patient symp-
about the efficacy of proton pump inhibitors (PPIs) in
toms rather than endoscopically verified esophageal mu-
patients with nonerosive reflux disease (NERD). We
aimedto synthesize available data anddetermine the
In practice, decisions about diagnosis and clinical in-
effectiveness of PPIs on symptom resolution in patients
terventions for GERD often are based on symptomology,
with NERD. Methods: A systematic review of the litera-
with heartburn and acid regurgitation as 2 of the defin-
ture identified studies reporting the effects of PPIs inpatients with NERD. Heartburn resolution data were
ing characteristics. Diagnostic clinical confirmation with
pooledacross studies. The effectiveness of PPI therapy
upper endoscopy or 24-hour esophageal pH monitoring
in inducing complete heartburn resolution was com-
is invasive, costly, and may not be readily available for
paredin patients with NERD vs. erosive esophagitis (EE). Results: Seven trials evaluating heartburn resolution in
The use of proton pump inhibitors (PPIs) is becoming
NERD were identified. Higher proportions of patients
more common because mounting evidence indicates their
reportedachieving sufficient heartburn resolution com-
superior efficacy in both NERD and erosive esophagitis
paredwith complete heartburn resolution. The effect of
(EE).6 Despite available information pertaining to the
PPIs on sufficient heartburn resolution was observed
efficacy of PPI therapy in NERD, little has been done to
sooner than was complete heartburn resolution. Thera-
synthesize existing data with respect to different PPI
peutic gain of PPI therapy over placebo rangedfrom30% to 35% for sufficient heartburn control andfrom
therapeutic regimens.7 Clinical efficacy measures for EE
25% to 30% for complete heartburn control. Pooled
therapies commonly focus on acute healing and mainte-
response rates at 4 weeks were significantly higher for
nance of healing using upper-gastrointestinal endoscopy.
patients with EE comparedwith NERD (56% vs. 37%,
Much less information pertaining to symptomatic reso-
P < 0.0001). Conclusions: PPIs provide a more modest
lution in EE patients can be found. Most clinical end
therapeutic gain in patients with NERD as compared
points in NERD are based on less-verifiable clinical
with those with EE. A trendin increasedtherapeutic gain
outcomes such as symptom severity, frequency, and in-
for NERD patients was shown throughout the 4 weeks,
tensity. Furthermore, outcome assessment in NERD is
suggesting that 4 weeks of follow-up evaluation may be
complicated by the lack of clear disease definition and
insufficient to show full therapeutic gain in this patient
inconsistent definition of symptom relief.8
The objective of this study was to perform a systematic
review of the literature and to synthesize all available
Gastroesophagealrefluxdisease(GERD)isacommon data on the effectiveness of PPI therapy in resolving
disorder characterized by heartburn and acid regur-
symptoms in NERD patients. The secondary objective
gitation, with or without the presence of esophagealmucosal damage.1 Patients with nonerosive reflux disease
Abbreviations used in this paper: CI, confidence interval; EE, erosive
(NERD) may experience severe and even debilitating
esophagitis; GERD, gastroesophageal reflux disease; NERD, nonero-
heartburn episodes. In fact, studies have shown that
sive reflux disease; PPI, proton pump inhibitor.
2004 by the American Gastroenterological Association
GERD symptom severity, frequency, and intensity are
correlated poorly with degree of esophageal mucosal
EFFECT OF PPI USE IN PATIENTS WITH NERD 657
was to compare the effectiveness of PPI therapy between
Table 2. Classification of Esophageal Mucosal Involvement
patients with NERD and those with EE.
a) Endoscopically negative and erythema and friabilityb) Erythema and friability
A review of the medical literature was conducted to
b) Endoscopically negative and erythema and friability
identify trials evaluating the effect of PPIs in patients with
classic symptoms of GERD and negative upper endoscopy. Medline and HealthStar databases were searched for Englishlanguage articles published between 1980 and 2002. Medicalsubject headings for the search included: proton pump inhib-
tation, daytime heartburn, nighttime heartburn, and measures
itor (PPI), esophagitis, gastroesophageal reflux, rabeprazole,
of symptom severity. Information on available outcome mea-
omeprazole, lansoprazole, esomeprazole, and pantoprazole. We
sures was abstracted for all available periods.
searched the Food and Drug Administration web site for
Applying the definitions of complete and sufficient heart-
pertinent reports concerning PPI treatment indications for
burn resolution as described later (see the Complete Versus
NERD and abstracts presented during the American College
Sufficient Resolution Over Time section), we abstracted the
of Gastroenterology and the Digestive Disease Week confer-
proportions of patients meeting these definitions from the
ences between 1999 and 2001. Additional articles were iden-
selected articles based on intent-to-treat results. Data were
tified through a hand search of references from relevant articles
available on the following combinations: complete heartburn
and from physicians and researchers in the field.
resolution, sufficient heartburn resolution, complete heartburn
Titles, abstracts, and articles were reviewed serially against
maintenance, and sufficient heartburn maintenance.
explicit exclusion criteria. Two reviewers conducted indepen-
dent appraisals and resolved disagreements by consensus. In-terrater reliability was tested on a 10% sample, with val-
In accepted manuscripts, the study population was
identified as having NERD or mild nonerosive GERD based
Articles were rejected at the title stage if they did not
on endoscopic results. A majority of investigators classified
pertain to PPI monotherapy or a condition of interest (i.e.,
patients based on the grade of EE. A few investigators did not
esophagitis, acid reflux, heartburn, GERD, NERD, gastric or
use a standard esophageal grading scheme but provided
esophageal acid), or were classified as reviews, case reports,
enough information to determine if patients were endoscopy
editorials, letters, or meta-analyses. Similar criteria were ap-
negative, had erythema or friability, and/or had erosions. The
plied to abstracts, with the additional requirement of data on
most common classification schemes were the Savary–Miller,
NERD, on esophagitis grade 0 and/or 1, and on outcomes of
the Hetzel–Dent, and the Los Angeles, along with their mod-
interest. The full text of selected articles were reviewed and
rejected if they did not report primary results from a random-
Criteria varied across the classification systems (Table 1). For
ized trial of symptomatic resolution with acute PPI treatment,
example, although patients without erythema or friability
or failed to include adults age 18 or older with esophagitis
would receive no grade using the Savary–Miller or Los Angeles
systems, they would be assigned a grade 0 using the Hetzel–Dent system. Likewise, patients with erythema or friability are
assigned a grade I using the Savary–Miller, a grade 1 using the
Abstracted study data included: location, design, de-
Hetzel–Dent, and no grade using the Los Angeles system.
scription, multi- or single-center setting, endoscopic grade and
Another issue in comparing patient populations was that some
definition of included patients, classification system, treatment
studies included only patients with negative endoscopy, others
goal, and symptom severity. Data pertaining to reported
with erythema or friability only, and still others included
symptom occurrence, frequency, and severity also were col-
patients with negative endoscopy, erythema, or friability, but
lected. Symptom measures included heartburn, acid regurgi-
Because of the different definitions of endoscopic findings
and study populations, we developed a system for classifying
Table 1. Classification of Esophageal Mucosal Involvement
studies based on reported grades from various classification
systems (Table 2). Treatment comparisons were separated into3 groups. Group 1 included only endoscopically negative
patients. Group 2 was more flexible, allowing for erythema and
friability but without erosions; this group included mixed
patient populations, some with no endoscopic findings and
others with erythema and friability. Group 3 combined all
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 8
studies of patients with negative endoscopy, negative endos-
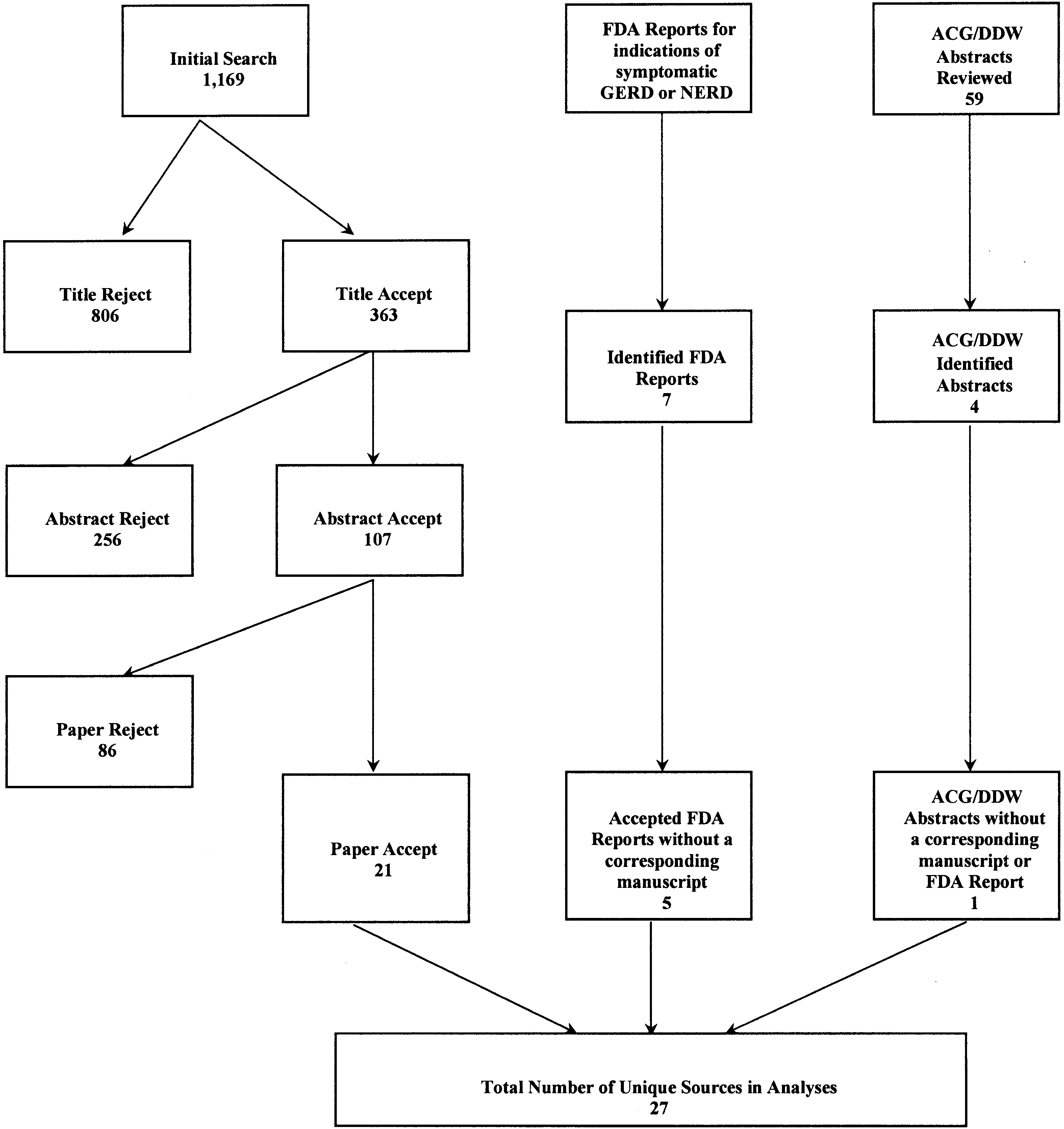
indications for symptomatic GERD or NERD. Our
copy or erythema and friability, or erythema and friability
search of the American College of Gastroenterology and
Digestive Disease Week databases resulted in 59 ab-
stracts for review. None presented data that were not also
available in the published literature or Food and DrugAdministration reports. Seven trials10–16 were included
Acute heartburn resolution was defined as either com-
plete or sufficient. Complete resolution was defined as no
Of the 7 clinical trials evaluating heartburn resolu-
heartburn during the preceding 7 days. Studies also measured
tion, there were 2 rabeprazole studies,15,16 2 esomepra-
sufficient (or satisfactory) heartburn resolution, defined as less
zole studies,13,14 and 3 omeprazole studies.10–12 All 7
than 1 day of moderate heartburn during the preceding 7 days
studies evaluated PPI therapy vs. placebo in patients
with NERD. A total of 1854 patients were evaluated,
with the smallest study including 123 patients16 and theremaining studies including over 200 patients each. Al-
We focused our analysis on placebo-controlled trials.
though all studies allowed for a run-in period without
Estimates of the pooled treatment effect were calculated for therisk difference (the proportion with heartburn resolution in the
PPI or histamine-2 receptor antagonists, only one
treated group minus the proportion with heartburn resolution
study10 excluded patients with any previous use.
in the placebo group) using Bayesian modeling. The risk
Five10,12–15 of the 7 studies presented data with multiple
difference captures the therapeutic gain or effect of treatment
treatment arms. A total of 12 treatment arms and 7
placebo arms were identified. The most frequent drug-
We stratified available treatment arms by the following
dose combination examined was omeprazole 20 mg (3
parameters: endoscopic grade of study population (Table 2),
treatment arms). Two treatment arms were available for
duration of PPI administration, and complete or sufficient
omeprazole 10 mg, esomeprazole 20 mg, esomeprazole
control of heartburn. Differences across grades, time periods,
40 mg, and rabeprazole 20 mg, with only one treatment
and definitions of heartburn control were evaluated.
Table 4 shows all sufficient and complete heartburn
resolution outcomes at all time periods across all 7
We compared the effectiveness of PPI treatment on
studies. The majority of studies reported heartburn res-
complete heartburn resolution in patients with NERD vs. EE.
olution rates for 2 time periods. Thus, our analysis
We conducted a systematic review of the published literature
explored the risk difference (therapeutic gain) for the
and Food and Drug Administration reports pertaining to theeffectiveness of PPI therapy in patients with endoscopically
confirmed EE (Hetzel–Dent, grades 2– 4).9 Strict criteria were
Complete Versus Sufficient Resolution Over
used to identify relevant placebo-controlled articles of PPI
therapy in EE. Results were pooled in a similar manner to theNERD estimates.
Group 1: endoscopically negative subjects. Two
studies10,11 provided data on heartburn resolution for
endoscopically negative patients (Figure 2). The thera-peutic gain of PPI treatment over placebo for sufficient
resolution at the 2-week assessment was 0.29 (95%
The search identified 1169 references published
confidence interval [CI ], 0.21– 0.37). At 4 weeks, the
between January 1980 and January 2002. Figure 1 shows
therapeutic gain increased to 0.34 (95% CI, 0.28 – 0.41).
the inclusion and exclusion of articles at different points
No significant difference was observed between the ther-
during the review process. We accepted 363 titles for
apeutic gains at 2 and 4 weeks (P ϭ 0.42). No measure-
further screening and reviewed their abstracts, and re-
ments of complete resolution were available at 2 weeks.
viewed the full text of 107 articles.
At the 4-week assessment, the therapeutic gain of PPI
Three published articles met inclusion criteria, pre-
treatment over placebo was 0.25 (95% CI, 0.18 – 0.31).
senting results from randomized placebo-controlled trials
In comparing therapeutic gains at 4 weeks, a higher
with sufficient information for estimating the effects of
proportion of treated vs. placebo patients achieved suffi-
acute treatment on symptomatic GERD or NERD. Our
cient resolution compared with achieving complete res-
search of the Food and Drug Administration web site
olution. This difference between therapeutic gains was
yielded 4 additional reports concerning PPI treatment
not statistically significant (P ϭ 0.14).
EFFECT OF PPI USE IN PATIENTS WITH NERD 659
Figure 1. Flowchart of the sys-tematic review for NERD andsymptomatic GERD.
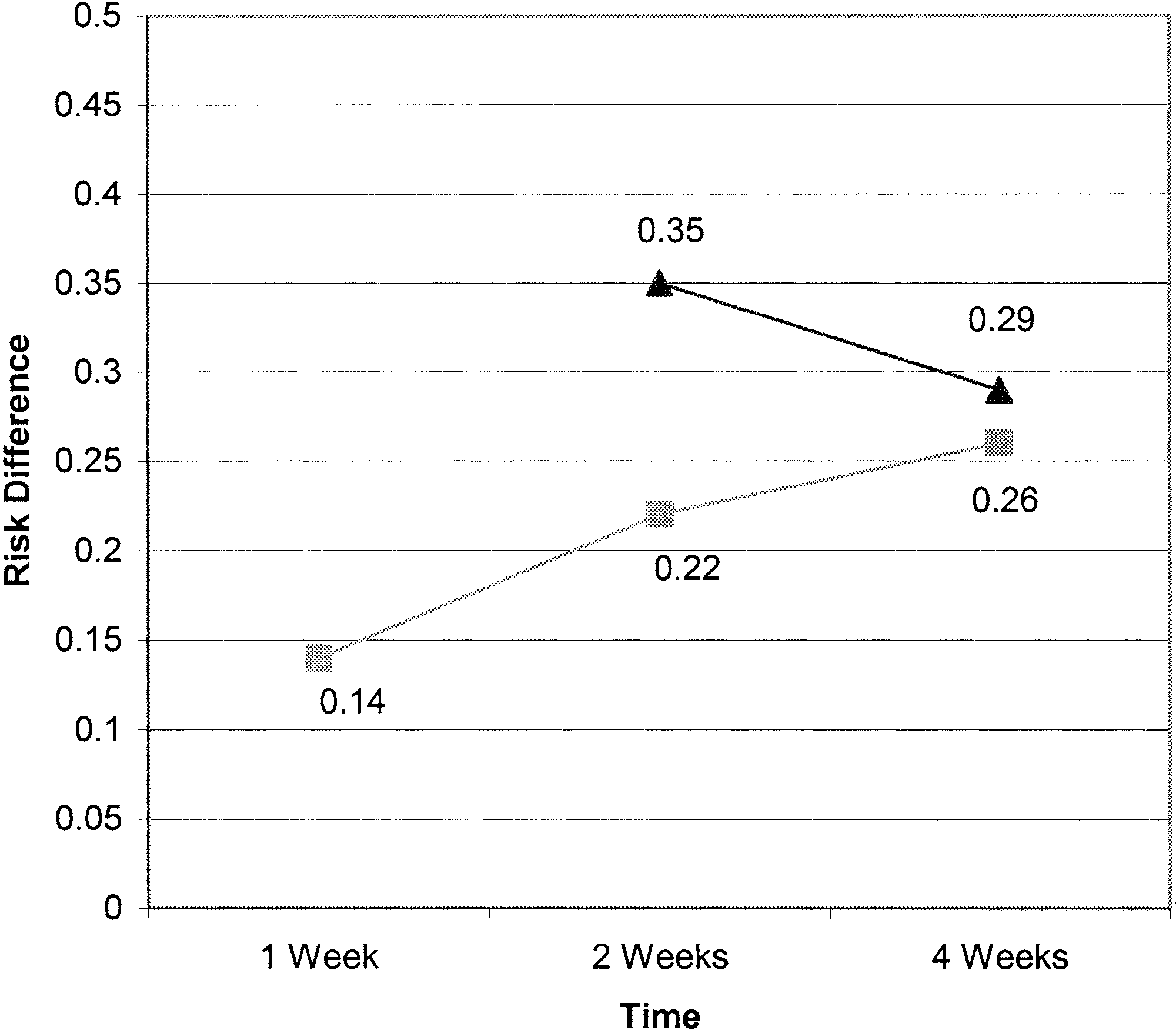
Group 2: patients with negative endoscopy and
the therapeutic gain of PPI treatment was 0.26 (95% CI,
erythema andfriability, or erythema andfriability alone.
0.23– 0.30). Although therapeutic gains increased over
Five studies12–16 contributed data on heartburn resolu-
time, no significant difference was observed between the
tion for our group 2 patient population (Figure 3). For
assessments (1-week vs. 2-week, P ϭ 0.58; 2-week vs.
sufficient resolution, the therapeutic gain of PPI treat-
ment over placebo at the 2-week measurement was 0.35
When therapeutic gains were compared within time
(95% CI, 0.26 – 0.44). At the 4-week measurement, the
periods, a higher proportion of group 2 patients reported
therapeutic gain decreased to 0.29 (95% CI, 0.19 – 0.39).
achieving sufficient resolution compared with achieving
The difference between the therapeutic gains at the 2-
complete resolution. The therapeutic gain for sufficient
and 4-week measurements was nonsignificant (P ϭ
resolution was significantly different from the therapeu-
tic gain for complete resolution at 2 weeks (P ϭ 0.04).
For complete resolution, therapeutic gains were calcu-
At 4 weeks, the gap between the therapeutic gains
lated for the 1-, 2-, and 4-week time periods. The
decreased, resulting in a nonsignificant difference be-
therapeutic gain of PPI treatment over placebo at 1 week
tween the 2 measurements (P ϭ 0.69).
was 0.14 (95% CI, 0.10 – 0.17). An increase in therapeu-
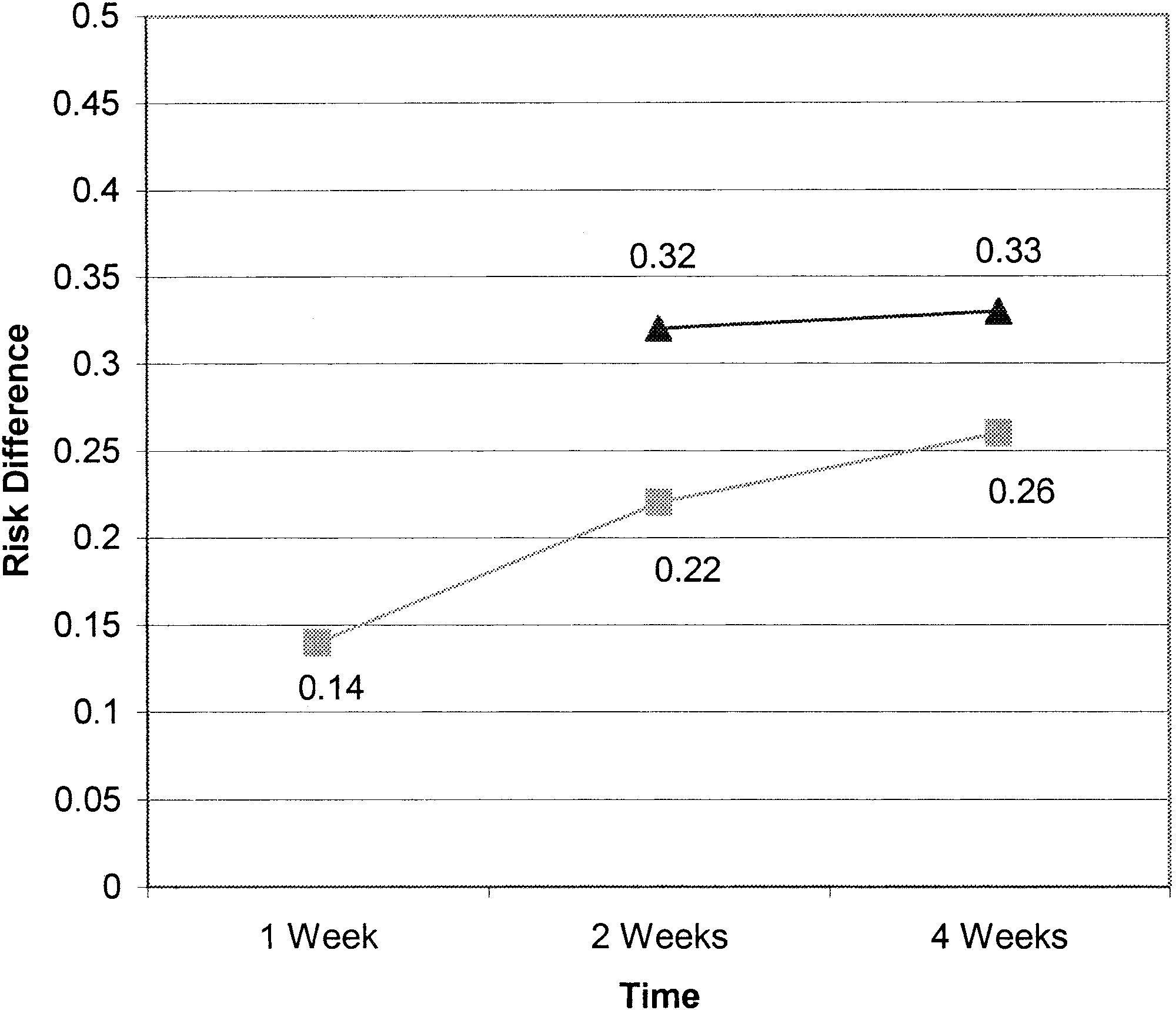
Group 3: patients with negative endoscopy, neg-
tic gain was observed between the 1- and 2-week assess-
oscopy anderythema andfriability, or ery-
ments, with the therapeutic gain at 2 weeks calculated as
thema andfriability alone. Results are consistent when
0.22 (95% CI, 0.19 – 0.25). For the 4-week assessment,
data for patients in both groups 1 and 2 are combined
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 8
Table 3. Identified Placebo-Controlled Trials of NERD Patients
OME10, omeprazole 10 mg; OME20, omeprazole 20 mg; ESO20, esomeprazole 10 mg; ESO40, esomeprazole 20 mg; FDA, Food and DrugAdministration; RAB10, rabeprazole 10 mg; RAB20, rabeprazole 20 mg. aThe JADAD score is a way of assessing the quality of reports involving randomized controlled clinical trials.30
(Figure 4). For sufficient resolution, the therapeutic gain
Again, no significant difference was observed between
of PPI treatment over placebo at 2 weeks was 0.32 (95%
the therapeutic gains at 2 and 4 weeks (P ϭ 0.25).
CI, 0.26 – 0.38). At the 4-week measurement, the ther-
Within time periods, higher proportions of patients
apeutic gain was 0.33 (95% CI, 0.27– 0.38). No signif-
achieved sufficient resolution as opposed to complete
icant difference was detected between the therapeutic
resolution. At the 2-week measurements, the difference
between therapeutic gains was significant (P Ͻ 0.05).
Results for complete resolution mirrored the results
The difference between therapeutic gains decreased at the
for group 2 patients at the 1-week (therapeutic gain ϭ
4-week measurement, and was not significant (P ϭ
0.14; 95% CI, 0.10 – 0.17) and 2-week (therapeutic
gain ϭ 0.22; 95% CI, 0.19 – 0.25) assessments. The
Summary. In general, the therapeutic gain of PPI
therapeutic gain of PPI treatment for complete heartburn
treatment over placebo ranged from 30%–35% for suf-
resolution at 4 weeks was 0.26 (95% CI, 0.23– 0.29).
ficient heartburn control and 25%–30% for complete
Table 4. Heartburn Measures Available for All Studies
OME20, omeprazole 20 mg; OME10, omeprazole 10 mg; ESO40, esomeprazole 20 mg; ESO20, esomeprazole 10 mg; RAB20, rabeprazole 20mg; RAB10, rabeprazole 10 mg.
EFFECT OF PPI USE IN PATIENTS WITH NERD 661
Figure 2. Treatment comparison with placebo for group 1 (endoscopynegative) patients: pooled difference (treatment Ϫ placebo) in propor-
Figure 4. Treatment comparison with placebo for all studies (group
tion with heartburn resolution by time. Œ, Sufficient; ■, complete.
3): pooled difference (treatment Ϫ placebo) in proportion with heart-burn resolution by time. Œ, Sufficient; ■, complete.
heartburn control. In other words, PPIs successfullytreated between one quarter and one third of the popu-
therapeutic gain for complete resolution for both group
lation. This held true for pooled estimates across all
2 patients (endoscopically negative and erythema and
treatments. Among all grades and time periods, PPIs
friability) and for all patients combined (group 3) (P ϭ
resulted in higher proportions of patients achieving suf-
0.04 and P ϭ 0.05, respectively). Over time, the thera-
ficient resolution compared with complete resolution.
peutic gain for complete resolution increased. However,
The effects of PPIs for sufficient resolution appeared
the difference between sufficient and complete resolution
sooner (approximately 2 weeks) compared with complete
at 4 weeks was not significant (P ϭ 0.14, P ϭ 0.69, and
resolution (4 weeks). At 2 weeks, the therapeutic gain for
P ϭ 0.12 for groups 1, 2, and 3, respectively).
sufficient resolution was significantly different from the
Comparison of Heartburn Resolution inNERD andEE
We compared the symptomatic response rates of
patients with NERD with those diagnosed with EE. Although endoscopic healing rates are reported com-monly in EE studies, symptomatic response to PPI ther-apy is not reported commonly. When reported, 4- and8-week data usually are presented. Thus, across theNERD and EE literature, only 4-week symptomaticresponse rates were reported for each population. As wasperformed for NERD, the combined effect of PPI ther-apy on the symptomatic response rate at 4 weeks waspooled across treatment strategies and dosages for EEpatients.
A systematic literature review of symptomatic healing
rates associated with PPI therapy in patients with EEidentified 2 randomized controlled trials.17,18 Both wereplacebo-controlled and contributed multiple treatment
Figure 3. Treatment comparison with placebo for group 2 (negative
arms of rabeprazole and pantoprazole, respectively. Com-
endoscopy and erythema and friability) patients: pooled difference
plete resolution of heartburn was the outcome measure
(treatment Ϫ placebo) in proportion with heartburn resolution by time.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 8
Table 5. Symptomatic Response Rates and Therapeutic Gains at 4 Weeks Among Patients With NERD and EE
Table 5 displays the pooled 4-week symptomatic re-
The lower symptom response rate to PPI treatment in
sponse rates and therapeutic gains for patients with
NERD patients as compared with patients with EE
NERD and EE. The 4-week symptomatic response rate
likely is owing to the different subgroups of patients
was significantly higher for patients with EE compared
identified as having NERD. A recent study by Martinez
with NERD (56% vs. 37%, respectively; P Ͻ 0.0001),
et al.28 showed that 50% of the patients with NERD
whereas the placebo symptomatic response rates were
have normal esophageal acid exposure. Of these patients
similar between the 2 groups (9.5% vs. 7.5%, respec-
with functional heartburn, 37% showed a close correla-
tively; P Ͼ 0.05). Thus, the therapeutic gain of PPI
tion between GERD symptoms and acid reflux events,
therapy over placebo was more than 75% higher among
and the rest (63%) were likely to experience heartburn
EE patients (48% for EE vs. 27% for NERD).
caused by non–acid-related stimuli. These findings areconsistent with the view that patients with NERD are a
heterogeneous group with different symptom causes and
NERD is the most common type of GERD that
thus different therapeutic responses to PPIs.
community-based physicians encounter. Because of the
The analysis also suggests that owing to the signifi-
lack of esophageal mucosal injury, treatment of NERD is
cantly lower symptom response rates to PPIs in patients
based commonly on a step-up approach. However, ther-
with NERD compared with those with EE, the step-up
apeutic studies in NERD have shown that PPIs are
approach has little merit in NERD patients. Adding the
superior to histamine-2 receptor antagonists or promo-
studies that showed a very limited (30%) symptom
tility compounds.19–21 In this study, we compared the
response rate of NERD patients to histamine-2 receptor
effectiveness of PPI therapy with that of placebo for
antagonists, a step-in approach with a PPI should be the
symptom resolution at different time periods in NERD
appropriate therapeutic intervention for NERD.19,23
patients, using published literature. Because of the lack
An important finding of our study is that the pooled
of esophageal mucosal injury, almost all NERD studies
therapeutic gain of PPI treatment for complete heartburn
limited the treatment period to 4 weeks.12,22–25 Last,
resolution increased from the 1-week to 2-week assess-
symptom response to PPI was compared between pa-
ment and again at the 4-week time period (0.14 3
0.22 3 0.26). Our study showed the need to reconsider
Several important points stand out. First, higher pro-
the 4-week study design in NERD patients undergoing
portions of NERD patients reported attaining sufficient
therapeutic intervention because some patients with
heartburn resolution as compared with attaining com-
NERD may have a longer lag time to symptom response.
plete heartburn resolution. This was apparent across all
This study systematically assessed and synthesized the
grades of NERD and across all time periods. In addition,
literature on the effectiveness of PPI therapy in the
PPI treatment led to sufficient heartburn resolution,
NERD population and compared symptomatic response
with the effects observed at the 2-week time period; the
rates on PPI therapy in both NERD and EE populations
effects of complete heartburn resolution were observed at
in the same time frame. Therapeutic gain (response to
the 4-week period. Finally, symptomatic response rate at
treatment minus response to placebo) allows for the
4 weeks was significantly higher for patients with EE
combination of data across a variety of studies and pro-
vides clinicians with a clinically meaningful range of
Our analysis suggests that to improve the outcome of
responses they should expect with therapy.
therapeutic studies in NERD, more modest clinical end
A few limitations were inherent to this study. One was
points should be considered. For many NERD patients,
the lack of a standard definition for NERD and the use
sufficient heartburn control may be a satisfactory thera-
of different classifications for GERD. Another limitation
peutic outcome. Because NERD patients rarely develop
was the lack of data points included in this analysis. This
EE, physicians can accept sufficient heartburn control as
may have resulted from the selected parameters used in
the systematic review or the definitions of NERD used
EFFECT OF PPI USE IN PATIENTS WITH NERD 663
by the researchers. A third limitation was the lack of
9. Hetzel DJ, Dent J, Reed WD, Narielvala FM, Mackinnon M, Mc-
comparable end points among included studies. Some
Carthy JH, Mitchell B, Beveridge BR, Laurence BH, Gibson GG. Healing and relapse of severe peptic esophagitis after treatment
studies reported complete daytime and/or nighttime
with omeprazole. Gastroenterology 1988;95:903–912.
heartburn resolution, whereas others reported complete
10. Lind T, Havelund T, Carlsson R, Anker-Hansen O, Glise H, Hern-
resolution of global symptoms. A hierarchy was created a
qvist H, Junghard O, Lauritsen K, Lundell L, Pedersen SA, Stub-berod A. Heartburn without oesophagitis: efficacy of omeprazole
priori to account for the choice of end points used in the
therapy and features determining therapeutic response. Scand J
analysis when a study reported more than one end point.
Last, we found low placebo symptom response rates for
11. Hatlebakk JG. Heartburn treatment in primary care: randomised,
double blind study for 8 weeks. BMJ 1999;319:550 –553.
PPI therapy in patients with NERD and with EE. Low
12. Richter JE, Peura D, Benjamin SB, Joelsson B, Whipple J. Efficacy
placebo response rates may be the result of assessing the
of omeprazole for the treatment of symptomatic acid reflux dis-
rigorous outcome of complete symptom resolution. In
ease without esophagitis. Arch Intern Med 2000;160:1810 –
addition, the low placebo response rates could be the
13. AstraZeneca. A comparative efficacy and safety study of H
result of the time period assessed because patient expec-
199/18 (20mg), H 199/18 (40mg) vs. placebo in study subjects
tations of treatment response may vary by time.
with symptomatic GERD. FDA Report 21-153-225. 1999.
In summary, as expected, NERD patients are likely to
14. AstraZeneca. A comparative efficacy and safety study of H
199/18 (20mg), H 199/18 (40mg) vs placebo in study subjects
report sufficient heartburn resolution more often than
with symptomatic GERD. FDA Report 21-153-226. 1999.
complete heartburn resolution and achieve sufficient res-
15. Janssen. A placebo-controlled trial of rabeprazole tablets, 10mg
olution sooner than complete resolution. Symptom re-
QD or 20mg QD, in the treatment of subjects with symptoms ofchronic Gastroesophageal Reflux Disease (GERD). FDA Report
sponse rate was significantly lower in NERD patients
compared with those with EE receiving standard-dose
16. Janssen. A double-blind, placebo-controlled trial of rabeprazole
PPI. Most importantly, during the first 4 weeks of
tablets, 20 mg once daily, in the treatment of subjects without
treatment, patients with NERD showed increased ther-
erosive esophagitis and who have symptoms of chronic gastro-esophageal reflux disease (GERD). FDA Report 20-973-RAB-
apeutic gain for complete heartburn resolution (from
0.14 to 0.26), suggesting that the trend of symptom
17. Cloud ML, Enas N, Humphries TJ, Bassion S. Rabeprazole in
improvement may well continue into the second month
treatment of acid peptic diseases: results of three placebo-controlled dose-response clinical trials in duodenal ulcer, gastric
of therapy. Future study designs in NERD patients
ulcer, and gastroesophageal reflux disease (GERD). The Rabe-
should not be limited to 4 weeks, and randomized pla-
prazole Study Group. Dig Dis Sci 1998;43:993–1000.
cebo-controlled studies comparing various PPI therapies
18. Richter JE, Bochenek W. Oral pantoprazole for erosive esoph-
for sufficient and complete heartburn resolution in pa-
agitis: a placebo-controlled, randomized clinical trial. Panto-prazole US GERD Study Group. Am J Gastroenterol 2000;95:
tients with NERD should be conducted.
19. Sabesin SM, Berlin RG, Humphries TJ, Bradstreet DC, Walton-
Bowen KL, Zaidi S. Famotidine relieves symptoms of gastro-
esophageal reflux disease and heals erosions and ulcerations.
1. Kahrilas PJ. Diagnosis of symptomatic gastroesophageal reflux
Results of a multicenter, placebo-controlled, dose-ranging study.
disease. Am J Gastroenterol 2003;98:S15–S23.
USA Merck Gastroesophageal Reflux Disease Study Group [see
2. Green JRB. Is there such an entity as mild oesophagitis? Eur
comments]. Arch Intern Med 1991;151:2394 –2400.
20. Kahrilas PJ, Fennerty MB, Joelsson B. High- versus standard-
3. Laursen LS, Havelund T, Bondesen S, Hansen J, Sanchez G,
dose ranitidine for control of heartburn in poorly responsive acid
Sebelin E, Fenger C, Lauritsen K. Omeprazole in the long-term
reflux disease: a prospective, controlled trial. Am J Gastroenterol
treatment of gastro-oesophageal reflux disease. A double-blind
randomized dose-finding study. Scand J Gastroenterol 1995;30:
21. Hatlebakk JG, Johnsson F, Vilien M, Carling L, Wetterhus S,
Thogersen T. The effect of cisapride in maintaining symptomatic
4. Kuster E, Ros E, Toledo-Pimentel V, Pujol A, Bordas JM, Grande L,
remission in patients with gastro-oesophageal reflux disease.
Pera C. Predictive factors of the long term outcome in gastro-
Scand J Gastroenterol 1997;32:1100 –1106.
oesophageal reflux disease: six year follow up of 107 patients.
22. Bate CM, Griffin SM, Keeling PW, Axon AT, Dronfield MW, Chap-
man RW, O’Donoghue D, Calam J, Crowe J, Mountfords RA, Watts
5. Trimble KC, Douglas S, Pryde A, Heading RC. Clinical character-
DA, Taylor MD, Richardson PD. Reflux symptom relief with ome-
istics and natural history of symptomatic but not excess gastro-
prazole in patients without unequivocal oesophagitis. Aliment
esophageal reflux. Dig Dis Sci 1995;40:1098 –1104.
6. Chiba N, De Gara CJ, Wilkinson JM, Hunt RH. Speed of healing
23. Venables TL, Newland RD, Patel AC, Hole J, Wilcock C, Turbitt
and symptom relief in grade II to IV gastroesophageal reflux disease:
ML. Omeprazole 10 milligrams once daily, omeprazole 20 milli-
a meta-analysis. Gastroenterology 1997;112:1798 –1810.
grams once daily, or ranitidine 150 milligrams twice daily, eval-
7. Fass R, Fennerty MB, Vakil N. Nonerosive reflux disease— current
uated as initial therapy for the relief of symptoms of gastro-
concepts and dilemmas. Am J Gastroenterol 2001;96:303–314.
oesophageal reflux disease in general practice. Scand J
8. Fass R. Epidemiology and pathophysiology of symptomatic
gastroesophageal reflux disease. Am J Gastroenterol 2003;
24. Richter JE, Campbell DR, Kahrilas PJ, Huang B, Fludas C. Lanso-
prazole compared with ranitidine for the treatment of nonerosive
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 8
gastroesophageal reflux disease. Arch Intern Med 2000;160:
29. Harding SM, Richter JE, Guzzo MR, Schan CA, Alexander RW,
Bradley LA. Asthma and gastroesophageal reflux: acid suppres-
25. Galmiche JP, Barthelemy P, Hamelin B. Treating the symptoms of
sive therapy improves asthma outcome. Am J Med 1996;100:
gastro-oesophageal reflux disease: a double-blind comparison of
omeprazole and cisapride. Aliment Pharmacol Ther 1997;11:
30. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Ga-
vaghan DJ, McQuay HJ. Assessing the quality of reports of ran-
26. Isolauri J, Luostarinen M, Isolauri E, Reinikainen P, Viljakka M,
domized clinical trials: is blinding necessary? Control Clin Trials
Keyrilainen O. Natural course of gastroesophageal reflux dis-
ease: 17-22 year follow-up of 60 patients. Am J Gastroenterol1997;92:37– 41.
27. Fass R, Ofman JJ. Gastroesophageal reflux disease—should we
adopt a new conceptual framework? Am J Gastroenterol 2002;
Address requests for reprints to: Bonnie B. Dean, Ph.D., M.P.H.,
9100 Wilshire Boulevard, East Tower, Suite 655, Beverly Hills, Califor-
28. Martinez SD, Malagon IB, Garewal HS, Cui H, Fass R. Non-erosive
nia 90212. e-mail: [email protected].
reflux disease (NERD)—acid reflux and symptom patterns. Ali-
Supportedin part by an unrestrictedresearch grant from Janssen
ment Pharmacol Ther 2003;17:537–545.
Pharmaceutica Inc. (Titusville, NJ) andEisai Inc. (Teaneck, NJ).
SPECIFICATION FOR STOP SMOKING SERVICES PROVIDED BY PRIMARY CARE 1st April 2009 – March 2010 A local enhanced service between South East Essex PCT and General Practice 1. Introduction Smoking is the UK’s single greatest cause of preventable illness and early death. The most recent estimates show that around 114000 people in the UK are killed by smoking every year, accounting
 EFFECT OF PPI USE IN PATIENTS WITH NERD 659
Figure 1. Flowchart of the sys-tematic review for NERD andsymptomatic GERD.
EFFECT OF PPI USE IN PATIENTS WITH NERD 659
Figure 1. Flowchart of the sys-tematic review for NERD andsymptomatic GERD.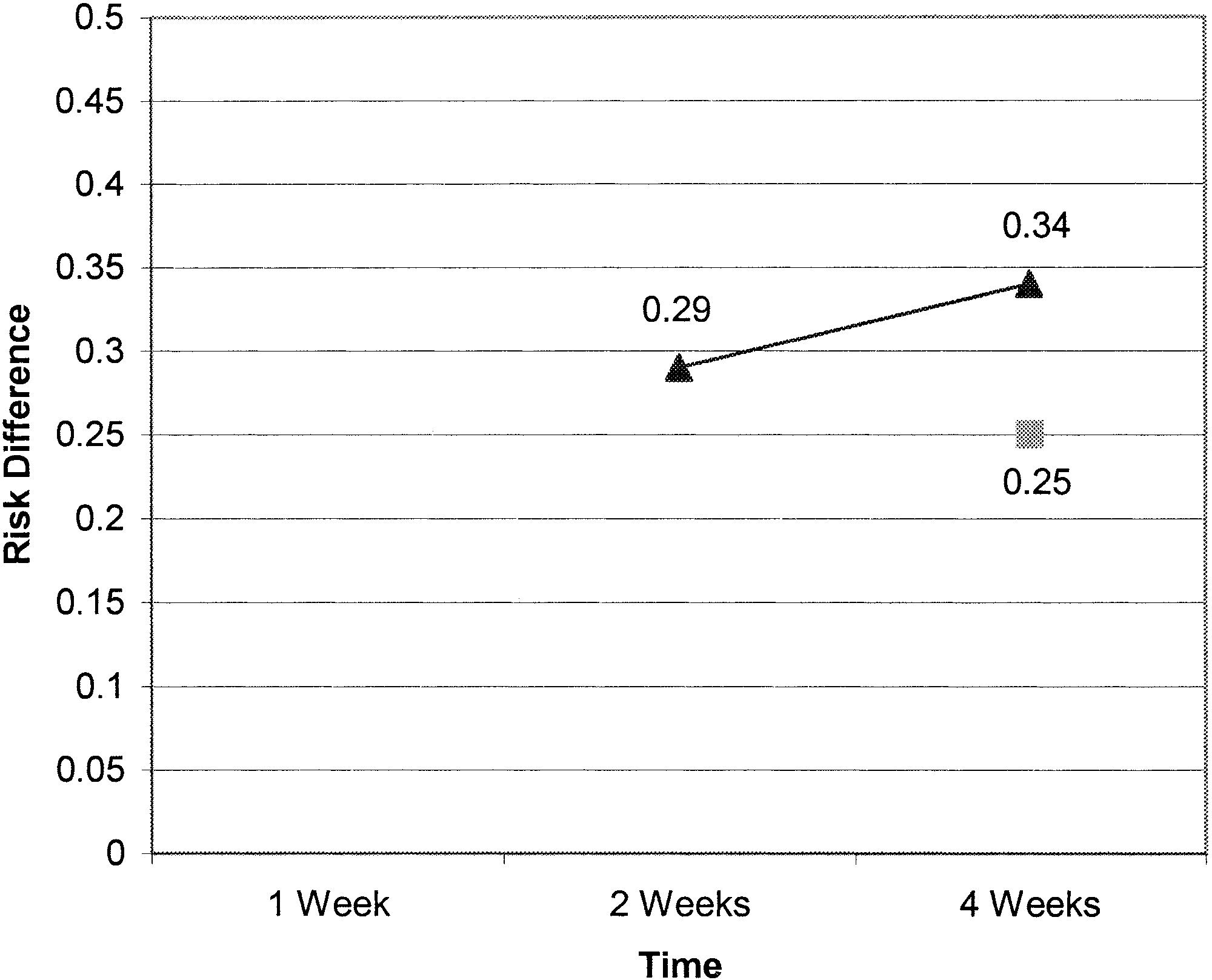
 EFFECT OF PPI USE IN PATIENTS WITH NERD 661
Figure 2. Treatment comparison with placebo for group 1 (endoscopynegative) patients: pooled difference (treatment Ϫ placebo) in propor-
Figure 4. Treatment comparison with placebo for all studies (group
tion with heartburn resolution by time. Œ, Sufficient; ■, complete.
EFFECT OF PPI USE IN PATIENTS WITH NERD 661
Figure 2. Treatment comparison with placebo for group 1 (endoscopynegative) patients: pooled difference (treatment Ϫ placebo) in propor-
Figure 4. Treatment comparison with placebo for all studies (group
tion with heartburn resolution by time. Œ, Sufficient; ■, complete.