Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Sac2.com.ar
ARTERIAL HYPERTENSION Progression of White Coat Hypertension to Sustained Hypertension After 10 Years
OLGA B. PÁEZ†, 1, PABLO A. PULEIO1, MARTA G. GOROCITO1, MIGUEL VISSER1, MIGUEL SCHIAVONE2, CLAUDIO R. MAJULMTSAC, 1, 2
ABSTRACT Background
The long-term outcome of white coat hypertension (WCH) is still controversial
despite the extensive information currently available. Objective
To evaluate the cumulative incidence of sustained hypertension (SH) among patients
with white coat hypertension compared to normotensive patients after 10 years of
Two hundred and fifty patients of both genders were prospectively included in the
study with the following office blood pressure (OBP) and 24-hour ambulatory blood
Hypertension
The patients were divided into two groups: 129 patients with WCH and 121
normotensive patients, and were evaluated after 10 years of follow-up.
Glucose blood level, lipid profile and left ventricular mass index (LVMI) were
Age, gender, smoking habits and glucose blood level were similar at baseline among
normotensive patients and patients with white coat hypertension.
However, body mass index, total cholesterol levels, lipid levels and LVMI were
significantly greater in white-coat hypertensive patients. Sustained hypertension
was developed by 48 patients with WCH and 21 normotensive patients. We found
an independent association between WCH and SH at 10 years of follow-up [OR: 2.5
Conclusion
Progression to sustained hypertension was greater in patients with white coat
hypertension compared to normotensive patients.
REV ARGENT CARDIOL 2012;80:217-221. Key words > White coat hypertension – Prognosis Abbreviations > AHR Heart rate OHR Office heart rate WCH White coat hypertension DT BP ABPM Daytime blood pressure on ABPM HT Hypertension BMI Body mass index LVMI Left ventricular mass index
MTSAC Full Member of the Argentine Society of Cardiology
† To apply as full member of the Argentine Society of Cardiology
1 Hospital Santojanni, Hypertension Unit, Autonomous City of Buenos Aires
REVISTA ARGENTINA DE CARDIOLOGÍA / VOL 80 Nº 3 / MAY-JUNE 2012
White coat hypertension (WCH) is defined as were excluded from the study.
hypertension (HT) in the clinical setting with normal
A smoker was defined as someone smoking at least one
values of home blood pressure (BP) or normal 24-
cigarette daily during the last month of the visit.
hour ambulatory blood pressure monitoring (ABPM)
Patients underwent lipid profile determination and
measurements. (1, 2) The prevalence of WCH varies ABPM one week after OBP was measured.
Ambulatory blood pressure was measured using the
between 20% and 45% depending on the population oscillometric Spacelabs 90207 monitor programmed to
studied, the value of office HT, gender and age.
take readings every 15 minutes during daytime and every
One of the main causes of the real prevalence of 30 minutes during night-time, adjusted according to the
WCH is threshold BP used to define HT in ABPM. sleeping habits of each patient.
(4) However, the cutoff value may underestimate or
Statistical Analysis
In general, WCH is considered a benign condition Quantitative variables are presented as mean and standard
in its outcome and treatment (5). One of the criteria deviation and qualitative variables as percentage. A t test was
used to characterize this outcome is the greater linear used for the analysis and comparison of quantitative variables
relationship of daytime ambulatory blood pressure with normal distribution, according to the the Kolmogorov–
compared to office blood pressure (OBP) with respect Smirnov test and homoscedasticity. The non-parametric
to target organ damage. However, this relationship Kruskall-Wallis test was used when the distribution was not
normal. Qualitative variables were analyzed using the chi
should not be the only influence of clinical WCH square test and a p value < 0.05 was considered statistically
characterization. This concept has been supported significant. The percentage of patients with normotension
by several studies demonstrating that the outcome of and with white coat hypertension at the beginning of the
WCH is not as benign as it was thought. (6-8)
study who developed SH after 10 years of follow-up was
Despite ample bibliographic information on calculated.
the characterization of WCH, it is still unclear
A stepwise multivariate analysis was performed to
if its outcome and prognosis is similar to that of evaluate association among variables. The model used
SH after 10 years of follow-up as the dependent variable
and OBP, daytime BP on ABPM (DT BP ABPM), body
The goal of the present study is to evaluate the mass index (BMI), smoking habits, hypercholesterolemia,
cumulative incidence of sustained hypertension hyperglycemia, LVMI, heart rate (HR), and WCH at baseline
(SH) among patients with white coat hypertension as independent variables. A p value < 0.05 was used to
compared to normotensive patients after 10 years of determine a significant association. A logistic regression
analysis was used to estimate the odds ratio for developing
SH including the same variables described in the former
model, adjusted for age, BMI and gender.
We conducted a prospective longitudinal study with control
Statistical analysis was performed using SPSS 17.0
group which was approved by the Ethics Committee of the statistical package for Windows (SPSS Inc., Chicago, III,
USA). A two-tailed p value < 0.05 was considered statistically
The patients were evaluated at baseline and after 10 significant.
years. Since de beginning of 1999, patients attending the
outpatient clinic at the Hospital Santojanni were invited to
participate in the study. The recruitment ended in 2000.
A total of 250 men and women between 45 to 55 years Characteristics of the population
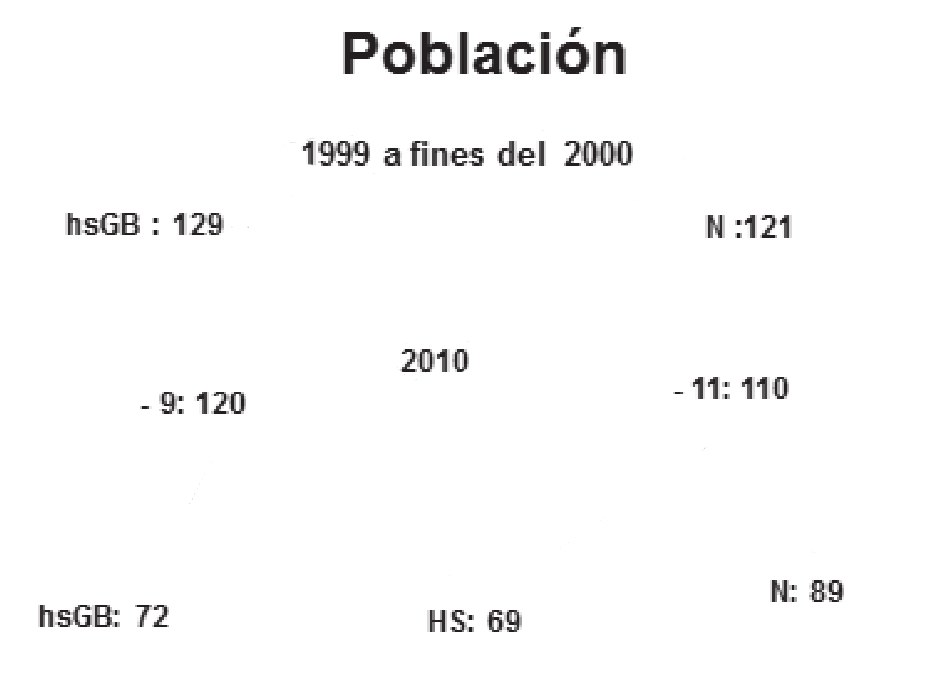
were selected and divided into two groups: 129 with WCH Of the original 250 patients, 20 patients were lost
and 121 with normotension. The diagnosis was based on to follow-up in 2010. Sustained hypertension was
systolic office blood pressure (SOBP) and/or diastolic office developed by 48 patients with WCH and by 21
blood pressure measurements plus daytime systolic and/or normotensive patients during follow-up (Figure 1).
Age, gender, BP on ABPM, office heart rate (OHR),
In 2010, 230 patients of the 250 original participants smoking habits and glucose blood levels were similar
were examined again, as it was impossible to contact 9 in both normotensive and WCH patients at baseline
patients with WCH and 11 with normal BP.
The following procedures were performed at the first examination (Table 1) and after 10 years evolution
medical visit and after 10 years of follow-up:
(Table 2). However, BMI was greater and triglycerides
Blood pressure was measured on three different visits and total cholesterol levels were higher in patients
using a Baum Manometer mercury sphygmomanometer, with WCH compared to those with normotension.
following the Argentine Council of Hypertension (9) and the
In 2010, patients with SH presented mild
American Heart Association guidelines. (10)
to moderate HT, 28 of which were receiving
Patients’ weight and height were recorded. A 12-lead antihypertensive agents (9 patients: enalapril
electrocardiogram was taken to all the patients in order to 15 mg, 3 patients: enalapril 10 mg, 4 patients:
exclude those with left ventricular hypertrophy, complete left
hydrochlorothiazide 25 mg, 10 patients: enalapril 10
bundle branch block or arrhythmias. These anomalies were
neither present during the second exam. At the first visit, mg + hydrochlorothiazide 25 mg, 2 patients enalapril
the patients were not receiving any medication, including 20 mg). Treatment was discontinued seven days
Patients with diabetes, metabolic syndrome, history of
The average time between patient inclusion in the
kidney or cardiovascular disease or any systemic condition study and the new diagnosis of SH was over five years
PROGRESSION OF WHITE COAT HYPERTENSION TO SUSTAINED HYPERTENSION AFTER 10 YEARS / Olga B. Paez et col. Table 2. Characteristics of population variables analyzed 10 years Population WCH (n = 120) N (n = 110) P Fig. 1. Progression to sustained hypertension in the population
studied. WCH: White coat hypertensive patients. N: Normoten-
sion SF: Sustained hypertension. -: Minus. The graph represents
the population according to the characteristics of office and ABPM blood pressure from the first medical visit to the 10-year
. Characteristics of the population: basal variables analyzed
Values are expressed as mean ± standard deviation. WCH: White coat
WCH (n = 120) N (n = 110) P
hypertension. SH: Sustained hypertension N: Normotension. ns: Non
significant. BMI: Body mass index. SOBP: Systolic office blood pressure. DOBP: Diastolic office blood pressure. LVMI: Left ventricular mass index.
TC: Total cholesterol. HDL: High density lipoprotein. TG: Triglycerides. w/m: Women/men. OHR: Office heart rate. bpm: Beats per minute.
ABPM: Ambulatory blood pressure monitoring. DT SBP ABPM: Daytime
in all the 69 patients. The information was obtained
There were no data on the physical examination
Anamnesis detected the presence of type 2 diabetes
(treated with metformin) in 3 patients with SH, 1 with
WCH and 1 with normotension. None of the patients
had cardiovascular events as myocardial infarction,
heart failure or kidney disease during that period.
The analysis of association among variables
identified SOBP [OR: 2.16 (95% CI 1.05-5.4)] and
WCH [OR: 2.5 (95% CI 1.7-3.5)] as predictors of SH
(Table 3). The other variables, including LVMI (B:
0.612; chi square: 1.8; p = 0.1) did not present a
significant association with the development of SH (p
DISCUSSION
WCH: White coat hypertension. N: Normotension. w/m: Women/men.
There is no agreement about morbidity and mortality
BMI: Body mass index. SOBP: Systolic office blood pressure. DOBP:
Diastolic office blood pressure. ABPM: Ambulatory blood pressure
In the different studies conducted on this
monitoring. DT SBP ABPM: Daytime systolic blood pressure on ABPM. DT
condition some authors found a greater risk of events
DBP ABPM: Daytime diastolic blood pressure on ABPM. NT SPB ABPM: Night-time systolic blood pressure on ABPM. NT DPB ABPM: Night-time
in this population; (11, 12); however, the predominant
diastolic blood pressure on ABPM. OHR: Office heart rate. bpm: Beats
concept is that the prognosis of WCH does not differ
per minute. TC: Total cholesterol. HDL: High density lipoprotein. TG:
from that of normotension. (13, 14) Based on our
Triglycerides. LVMI: Left ventricular mass index. Values are expressed as mean ± standard deviation. Values were analysed using a t test or the
previous results (8) and on those published by other
Kruskal-Wallis test with a significance level < 0.05. ns: Non significant.
authors, (15) we assume that the clinical situation of
REVISTA ARGENTINA DE CARDIOLOGÍA / VOL 80 Nº 3 / MAY-JUNE 2012
of HT, probably due to the small sample size. Table 3. Determinants of sustained hypertension by logistic regression analysis
In this study, WCH did not behave as a harmless
condition, showing a cardiovascular risk that was
Independent Standard Chi square
different from that of normotension. These results
variables
suggest the need for a tight follow-up of these patients
in order to achieve a strict control of risk factors and
SOBP: Systolic office blood pressure. WCH: White coat hypertension B: Regression coefficient. CONCLUSIONS In patients with WCH, progression to SH was greater
compared with normotensive patients after 10 years
WCH is intermediate between normotension and SH.
The results of the present study show that 40%
(95% CI 31-48) of patients with WCH developed SH
compared with 19% (95% CI 18.7-19.27) of those with RESUMEN
normotension after 10 years of follow-up. Hipertensión de guardapolvo blanco: evolución a hiper-
In general, the factors determining the clinical tensión sostenida luego de 10 años de seguimiento
outcome of WCH are not completely known, generating
Introducción
controversy. For example, daytime ambulatory blood No obstante la amplia información en la bibliografía sobre
pressure is tightly related with target organ damage as la caracterización de la hipertensión de guardapolvo blanco
left ventricular hypertrophy, heart failure and kidney (HGB), su evolución alejada es hasta el presente tema de
failure. In patients with WCH, daytime ambulatory
blood pressure is normal and not significantly greater Objetivo
Evaluar la incidencia acumulada de hipertensión sostenida
The correlation between office blood pressure, (HS) en hipertensos de guardapolvo blanco respecto de
normotensos a los 10 años de su inclusión en el estudio.
another determinant in the outcome of WCH, and
target organ damage is lower than that of ambulatory Material y Métodos
blood pressure. However, a linear relationship Se incorporaron en forma prospectiva 250 pacientes de
between OBP and cardiovascular events has been ambos sexos, según los siguientes valores de presión de
consultorio (PC) y de monitoreo ambulatorio de la presión
demonstrated, even in normotensive ranges. This arterial (MAPA) de 24 horas:
finding agrees with the results of the present study, as
SOBP was a predictor of the progression to SH in the HGB HS Normotensión
≥140 y/o 90 ≥140 y/o 90 ≤140 y/o 90
In the present study, subjects with WCH had higher
lipid values compared to normotensive patients since Se conformaron dos grupos: 129 hipertensos de guardapolvo
this population is more predisposed to atherogenesis blanco y 121 normotensos, los cuales fueron evaluados
and metabolic syndrome (16, 17). However, the nuevamente a los 10 años de seguimiento.
multivariate analysis showed that this was not a Se midieron la glucemia, el perfil lipídico y el índice de masa
major determinant of greater risk to develop SH.
The characterization of WCH as “low risk” is Resultados
mainly due to the level of daytime BP established as Las variables edad, sexo, tabaquismo y glucemia de
normal by ABPM. This means that the higher the normotensos e hipertensos de guardapolvo blanco fueron
value of chosen normal daytime BP, the greater the Los hipertensos de guardapolvo blanco, por el contrario,
likelihood of developing organ damage. On this issue, presentaron valores significativamente superiores en IMC,
Staessen et al. (18) defined WCH when daytime BP on colesterol total, hipertrigliceridemia e IMVI. Cuarenta y
ABPM was ≤ 146/91 mm Hg, and Pickering et al. (1) ocho hipertensos de guardapolvo blanco y 21 normotensos
originales evolucionaron a HS. La HGB se asoció en forma
independiente con HS a los 10 años de seguimiento [OR: 2,5
We considered normal BP when the value of (IC 95% 1,2-4,2)].
daytime BP on ABPM was ≤ 135/85 mm Hg so as not
to overestimate target organ damage in patients with Conclusión
La evolución a hipertensión sostenida fue mayor en los
WCH. In this way, we ensured that patients with SH hipertensos de guardapolvo blanco que en los normotensos.
Left ventricular mass index, a well-known predictor
Palabras clave > Hipertensión de guardapolvo blanco -
of target organ damage (19, 20), was estimated in the Pronóstico
population and results were similar to those reported
by similar studies. (21, 22) In subjects with WCH, REFERENCES
LVMI was greater compared to normotensive patients 1. Pickering TG, James GD, Boddie C, Harshfield G, Blank S, Laragh
in both baseline and at 10 year determinations, J. How common is white coat hypertension? JAMA 1988;259:225-8.
suggesting greater risk in this population. However, 2. Drayer JI, Weber MA, Nakamura DK. Automated ambulatory
blood pressure monitoring: A study in age-matched normotensive
this variable was not associated with the development and hypertensive men. Am Heart J 1985;109:1334-8.
PROGRESSION OF WHITE COAT HYPERTENSION TO SUSTAINED HYPERTENSION AFTER 10 YEARS / Olga B. Paez et col. 3. 2007 Guidelines for the Management of Arterial Hypertension; 14. Pierdomenico SD, Lapenna D, Di Mascio R, Cuccurullo F.
The Task Force for the Management of Arterial Hypertension of
Short- and long-term risk of cardiovascular events in white coat
the European Society of Hypertension (ESH) and of the European
hypertension. J Hum Hypertens 2008;22:408-14.
Society of Cardiology (ESC). J Hypertens 2007;25:1105-87. 15. Palatini P, Mormino P, Santonastaso M, Mos L, Dal Follo M, 4. Perloff D, Grim C, Flack J, Frohlich E, Hill M, McDonald M,
Zanata G, et al. Target-organ damage in stage I hypertensive
et al. The prognostic value of ambulatory blood pressures. JAMA
subjects with white coat and sustained hypertension. Results from
the HARVEST Study. Hypertension 1998;31:57-63. 5. Pierdomenico SD, Cuccurullo F. Prognostic value of white-coat 16. Mulè G, Nardi E, Cottone S, Cusimano P, Incalcaterra F,
and masked hypertension diagnosed by ambulatory monitoring Palermo A, et al. Metabolic syndrome in subjects with white-coat
in initially untreated subjects: an updated meta-analysis. Am J
hypertension: Impact on left ventricular structure and function. J
6. Kario K, Shimada K, Schwartz JE, Matsuo T, Hoshide S, Pickering
17. Björklund K, Lind L, Vessby B, Andrén B, Lithell H. Different
TG. Silent and clinically overt stroke in older Japanese subjects
metabolic predictors of white-coat and sustained hypertension over
with white-coat and sustained hypertension. J Am Coll Cardiol
a 20-year follow-up period: a population-based study of elderly men.
7. Ohkubo T, Kikuya M, Metoki H, Asayama K, Obara T, Hashimoto 18. Staessen JA, Fagard RH, Lijnen PJ, Thijs L, Van Hoof R, Amery A.
J, et al. Prognosis of “masked” hypertension and “white-coat” Mean and range of the ambulatory pressure in normotensive subjects
hypertension detected by 24-h ambulatory blood pressure from a meta-analysis of 23 studies. Am J Cardiol 1991;67:723-7.
monitoring 10-year follow-up from the Ohasama study. J Am Coll
19. Koren MJ, Savage DD, Casale PN, Laragh JH, Devereux
RB. Changes in left ventricular mass predict risk in essential
8. Majul C, Páez O, De María M, Cragnolino R, López A, Gorosito
hypertension. Circulation 1990;82:29-32.
A y col. Hipertensión por guardapolvo blanco: ¿es una entidad 20. De Simone G, Devereux RB, Koren MJ, Mensah GA, Casale PN,
intermedia entre normotensos e hipertensos sostenidos? Rev Argent
Laragh JH. Midwall left ventricular mechanics. An independent
predictor of cardiovascular risk in arterial hypertension. Circulation
9. Consenso de Hipertensión Arterial. Consejo Argentino de 1996;93:259-65.
Hipertensión Arterial “Dr. Eduardo Braun Menéndez”. Rev Argent
21. Verdecchia P, Carini G, Circo A, Dovellini E, Giovannini E,
Lombardo M, et al. The MAVI Study Group. Left ventricular mass
10. Perloff D, Grim C, Flack J, Frohlich ED, Hill M, McDonald M.
and cardiovascular morbidity in essential hypertension: the MAVI
Human blood pressure determination by sphygmomanometry. study. J Am Coll Cardiol 2001;38:1829-35. 22. Sega R, Trocino G, Lanzarotti A, Carugo S, Cesana G, Schiavina 11. Mancia G, Bombelli M, Facchetti R, Madotto F, Quarti-Trevano
R, et al. Alterations of cardiac structure in patients with isolated
F, Polo Friz H, et al. Long-term risk of sustained hypertension in
office, ambulatory, or home hypertension: data from the general
white-coat or masked hypertension. Hypertension 2009;54:226-32.
population (Pressione Arteriose Monitorate E Loro Associazioni
12. Gustavsen PH, Høegholm A, Bang LE. Kristensen KS. White
[PAMELA] Study). Circulation 2001;104:1385-92.
coat hypertension is a cardiovascular risk factor: a 10-year follow-up
study. J Hum Hypertens 2003;17:811-7. 13. Fagard RH, Cornelissen VA. Incidence of cardiovascular events
in white-coat, masked and sustained hypertension versus true Disclosure
normotension: a meta-analysis. J Hypertens 2007;25:2193-8.
CONCENTRATION AND COMPETITION IN THE CHEMOTHERAPY DRUG MARKET Introduction The pharmaceutical industry is comprised of companies that discover andsell drugs that require a doctor’s prescription. The pharmaceutical industryranks among the top industries in the United States in sales and research anddevelopment. This chapter considers competition in this industry and investi-gates the relat
Product Data Sheet EUMULGIN® B 1 PH General characterisation Chemical description Cetyl stearyl alcohol with 12 mol EO Labeling information INCI name(s) Ceteareth-12 Composition hints for finished product label Ceteareth-12 Registrations Ingredient CASR-No. EINECS/ELINCS-No . Officially listed in / Quality conforms to Ph. Eur.: Conforms to the current a
 PROGRESSION OF WHITE COAT HYPERTENSION TO SUSTAINED HYPERTENSION AFTER 10 YEARS / Olga B. Paez et col.
PROGRESSION OF WHITE COAT HYPERTENSION TO SUSTAINED HYPERTENSION AFTER 10 YEARS / Olga B. Paez et col.