Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Doi:10.1016/j.maturitas.2003.12.012
Patients with osteoporosis prefer once weekly to
David Kendler , Annie Wai Chee Kung , Ghada El-Hajj Fuleihan ,
José Gerardo González González , Keavy A. Gaines ,
a St. Vincent’s Hospital, 120-809 W 41 Avenue, Vancouver, BC, Canada V5Z 2N6
b Queen Mary Hospital, Hong Kong, PR China
c American University of Beirut Medical Center, Beirut, Lebanon
d Universidad Autónoma de Nuevo León, Monterey, Nuevo León, Mexico
e Merck and Co. Inc., Whitehouse Station, NJ, USA
f Merck Sharp and Dohme Inc. (Europe), Brussels, Belgium
Received 17 July 2003; received in revised form 17 December 2003; accepted 17 December 2003
Abstract Objectives: Once weekly dosing of alendronate has been shown to provide equivalent efficacy to once daily dosing for
treatment of osteoporosis in postmenopausal women. Whether patients will prefer weekly dosing to daily dosing for a chroniccondition such as osteoporosis has not been studied. The aim of this international study was to assess preference for the weeklyor daily dosing regimen of alendronate among postmenopausal women with osteoporosis. Methods: This randomised open-labelcrossover study was conducted at 45 study sites in 19 countries. Four hundred and six postmenopausal women with osteoporosiswere assigned randomly to treatment with either alendronate 70 mg once weekly for 4 weeks followed by alendronate 10 mg oncedaily for 4 weeks or vice versa. The main outcome was the responses of the participants to the Dosing Regimen Questionnaireadministered at the end of the study. Results: Of the participants expressing a preference, 84% preferred the once weekly dosingregimen with alendronate to the once daily dosing regimen. In addition, the once weekly regimen was considered by 87% ofthe participants to be more convenient and was the regimen most of the participants (84%) would be more willing to take for along period of time (P < 0.001 for each parameter). Conclusions: The majority of postmenopausal women with osteoporosispreferred the once weekly to the once daily dosing regimen of alendronate. Physicians should consider patient preference fordosing regimen when selecting the appropriate treatment for osteoporosis. 2004 Elsevier Ireland Ltd. All rights reserved. Keywords: Alendronate; Weekly; Preference; Osteoporosis
ଝ This data has been presented in abstract form at the International Society of Clinical Densitometry Annual Meeting, Atlanta, GA,
February 2002; the Fifth International Symposium: Clinical Advances in Osteoporosis, Honolulu, Hawaii, March 2002; The IOF WorldCongress on Osteoporosis, Lisbon, Portugal May 2002; the European League Against Rheumatism Annual Congress, Stockholm, Sweden,June 2002.
∗ Corresponding author. Tel.: +1-604-263-3644; fax: +1-604-263-3744. E-mail address: [email protected] (D. Kendler).
0378-5122/$ – see front matter 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.maturitas.2003.12.012
D. Kendler et al. / Maturitas 48 (2004) 243–2511. Introduction 2. Methods
Low adherence and compliance with medications
for chronic diseases is a well known problem. It hasbeen recognized that the full benefits of medications
This was an open-label, randomised, crossover
cannot be reached at current levels of compliance.
study of preference. This study was conducted at 45
Compliance with medical therapy for chronic diseases
sites across 19 countries representative of Europe,
is a complex and multifactorial problem, and requires
Middle East, the Americas, and Asia-Pacific. Par-
innovative solutions. Many attempts have been made
ticipants were randomly assigned to treatment with
to institute interventions to improve medication com-
either alendronate (Fosamax®, Merck & Co. Inc.,
pliance. These interventions have been only modestly
Whitehouse Station, NJ, USA) 10 mg once daily
successful at best One of the most successful in-
followed by treatment with alendronate 70 mg once
terventions demonstrated to improve compliance is a
weekly, or treatment with alendronate once weekly
simplified dosing regimen. For example, it has been
followed by alendronate once daily. Each dosing reg-
shown that compliance improves as the number of
imen was administered for 4 weeks, with a 1 week
doses taken each day decreases Whether even
off therapy period between dosing regimens. After
less frequent dosing regimens, such as weekly dosing,
experiencing both regimens, the participants com-
would further improve compliance for chronic therapy
is not known. Few medications for a treatment of a
Ethics review committee approval was obtained for
chronic disease are available in a once weekly formu-
each site. Informed consent was obtained from all
lation, and therefore little information is available on
participants prior to performance of any study-related
patient acceptance of a medication administered once
Recently, taking advantage of pharmacokinetic
properties, alendronate was developed for once weeklydosing for treatment and prevention of osteoporosis.
Postmenopausal women with osteoporosis (as
The once weekly dosing regimen for alendronate
determined by the investigator) were recruited
was developed in an attempt to simplify the dosing
from investigators’ practices and from media ad-
regimen and potentially enhance compliance. Once
vertisements. Participants were na¨ıve to thera-
weekly dosing with alendronate has been shown to
pies for osteoporosis, including bisphosphonates,
provide equivalent efficacy to once daily dosing for
calcitonin, and selective estrogen receptor mod-
treatment of osteoporosis in postmenopausal women
Patients are used to establishing a daily regimen
and Vitamin D were allowed. Reasons to ex-
to encourage them to remember to take their medi-
clude women from the study included inability
cations. Whether a once weekly regimen would be
to follow alendronate dosing instructions, condi-
easier to follow, or potentially more complicated and
tions which delay esophageal emptying such as
subject to greater inconvenience or missed doses, was
stricture or achalasia, or a history of hypocal-
cemia, hypoparathyroidism, osteomalacia, Paget’s
In this study, we investigated the dosing prefer-
disease or renal osteodystrophy. Other exclusions
ence for alendronate given once daily or once weekly
included uncontrolled moderate or severe hyper-
among postmenopausal women with osteoporosis in a
tension, new onset angina or myocardial infarc-
randomized, open-label, cross-over designed, interna-
tion within 6 months, impaired renal function,
tional clinical trial. The participants were given the op-
other significant end organ diseases, or cancer.
portunity to experience both once weekly alendronate
Use of nonsteroidal antiinflammatory agents, H2
and once daily alendronate prior to saying which they
antagonists, proton pump inhibitors, or a history
prefer, which they think is more convenient, and which
they would be more willing to continue over a long
ders of esophageal motility) were not reasons for
D. Kendler et al. / Maturitas 48 (2004) 243–251DOSING REGIMEN QUESTIONNAIRE
You have just completed this study and have followed two different osteoporosis treatment routines: you have taken the osteoporosis medication once a week and you have taken it once a day. It is important to remember that the osteoporosis medications you took during these two treatment routines have the same beneficial effect for your bones. Please answer the three questions below. We encourage you to choose the answer that best describes your experience. For each question, please check one box only 1. Which treatment routine do you prefer?
I prefer the once a week treatment routine
I prefer the once a day treatment routine
2. Which treatment routine is more convenient?
The once a week treatment routine is more convenient
The once a day treatment routine is more convenient
The once a week treatment routine and the once a day treatment routine are equally convenient
3. Which treatment would you be more willing to take for a long period of time?
I would be more willing to take the once a week treatment for a long period of time
I would be more willing to take the once a day treatment for a long period of time
I would be equally willing to take either the once a week or the once a day treatment for a long period of time
Fig. 1. Dosing Regimen Questionnaire. 2.3. Treatment assignment and randomisation
calcium and Vitamin D supplements according to thestandard of care in their communities. In addition,
Allocation to treatment sequence was assigned ran-
counseling for modification of lifestyle habits related
domly using a computer-generated allocation sched-
to osteoporosis, such as exercise, smoking cessation,
ule. Open-label drug was provided for 4 weeks for
and fall prevention, was encouraged.
each regimen (4 tablets of alendronate 70 mg onceweekly and 28 tablets of alendronate 10 mg once
daily). For each regimen, the participants receivedthe standard dosing instructions for alendronate. For
Participants returned for a randomisation visit for
the once weekly regimen, the participants chose 1
initiation of the first treatment period and again when
day of the week for the weekly dosing. Throughout
switching to the second treatment period. All partic-
the study, all participants were encouraged to take
ipants were phoned on the day of initiation of study
D. Kendler et al. / Maturitas 48 (2004) 243–251
drug (or up to 3 days after, in case of intervening hol-
naire. The Mainland–Gart test for binary response in
iday or weekend days) in each treatment period to en-
a two-treatment, two-period crossover trial was used
sure proper compliance to dosing instructions. After
for this analysis The analyses of the responses
experiencing both treatment regimens, participants re-
to the other two questions on the questionnaire were
turned for a final visit for completion of the Dosing
handled in a similar fashion. As there was only one
Regimen Questionnaire and collection of information
primary endpoint (preference), there was no need for
a multiplicity adjustment. The sample size estimationwas based on 90% power to detect a 20% difference
2.5. Questionnaire development and testing
in preference with a 2-tailed test at a 5% significancelevel. At least 260 participants (130 per group) were
The Dosing Regimen Questionnaire was designed
required; additional participants were enrolled to al-
to include the parameters of preference, convenience,
low for those who would not complete the trial.
and willingness to continue taking the regimen long
To assess the sequence effect of treatments, that
term. In development of the questionnaire, in-depth
is, to test whether the percentage of participants who
interviews were conducted with women previously di-
preferred alendronate 70 mg once weekly was the
agnosed with osteoporosis, including those receiving
same irrespective of the order in which the two treat-
alendronate and those receiving other therapies for
ment regimens have been given, the Mainland–Gart
osteoporosis. These interviews were used to modify
test was used, with a two-sided test at the 10% sig-
the wording of the questions to ensure concept con-
nificance level. To investigate the influence of various
veyance and clarity before the questionnaire in English
factors on preference for dosing regimen, analyses
was finalised. Translation of the questionnaire into lo-
by subgroup was performed. These analyses used a
cal languages required at least two translations for
logistic model on the preference of alendronate once
each language, back-translations for each translation,
weekly including the factor under consideration as
a committee review, and pre-testing of the translated
main effect to assess the consistency across the differ-
questionnaire with non-study participants in the target
ent subgroups. The following factors were considered:
population of women with osteoporosis. This rigorous
country of residence, age group (≤65, >65 years),
procedure for translations was instituted to ensure that
number of concomitant chronic medications (defined
the original meaning and intent of the questionnaire
as a medication taken for more than 75% of the time
was preserved when a translation was required.
during the study), intake of at least one concomitant
At the completion of the study, a short script was
medication on more than 75% of the days in the study,
read to each participant to introduce the questionnaire
and number of active medical conditions at baseline.
and to explain that the participant is to complete the
The adverse experiences were analysed for all par-
questionnaire on her own, to the best of her ability,
ticipants who took at least one dose of study med-
without assistance from the investigator site staff. Par-
ication for the treatment phase under consideration.
ticipants were informed that the two treatment regi-
Also, a comparison of the overall adverse experience
mens (alendronate 70 mg once weekly and alendronate
reporting of the two treatment regimens was done us-
10 mg once daily) have equal benefit to bone so that
ing the McNemar’s Test, which included only partici-
their choice of regimen was not influenced by any
pants who received at least one dose of each regimen.
perception of relative efficacy. Each participant com-pleted the questionnaire herself. 3. Results 3.1. Participants’ characteristics
The primary analysis was the preference of partici-
pants towards either of the two regimens. The analysis
A total of 406 postmenopausal women with osteo-
included all participants who took at least one dose
porosis from 19 countries participated in the study.
from each regimen and expressed a preference based
Sixty-five percent of the women reported their race
on the first question of the Dosing Regimen Question-
as Caucasian, 22% Asian, and 8% Hispanic. Regional
D. Kendler et al. / Maturitas 48 (2004) 243–251
Number (%) with family history of osteoporosis
Number (%) with caffeine use ≥3 cups per day
diversity was also achieved with 92 (23%) of the par-
the Asia-Pacific region. The baseline characteristics
ticipants from North America, 57 (14%) from Central
of the two treatment sequence groups were similar
or South America, 104 (26%) from Europe, 54 (13%)
(The most common active medical conditions
from the Middle East and Africa and 99 (24%) from
reported at baseline (other than osteoporosis) were
Excluded, n=58 Entry criteria not met, n=30 Withdrew consent, n=22 Lost to followup, n=5 Protocol deviation, n=1
*Patients who discontinued therapy but had experienced both regimens and completed the Dosing Regimen Questionnaire were included in the final results.
Fig. 2. Participant assessment and followup throughout the study. D. Kendler et al. / Maturitas 48 (2004) 243–251
hypertension (114, 28%), osteoarthritis (46, 11%), hy-
imen first preferring the once weekly regimen. There-
percholesterolemia (36, 9%) and hypothyroidism (32,
fore, no effect by sequence was seen (P = 1.000).
Of the 360 (91%) participants who expressed that
All participants randomised received at least one
one regimen is more convenient, 314 (87%) consid-
dose of study medication. A total of 390 (97%) par-
ered the once weekly regimen to be more convenient
ticipants took all 4 of their weekly tablets and 344
(P < 0.001). For the question asking which regimen
(86%) participants took all 28 of their daily tablets.
they would be more willing to take for a long period
Three hundred and ninety-six took at least one dose
of time, 369 (93%) indicated a choice between reg-
from each regimen and all of these completed the ques-
imens. Of those, 311 (84%) indicated that the once
tionnaire. Three hundred and eighty-four participants
weekly regimen is the one they would be more willing
(95%) completed the study. The most common reason
to take long term (P < 0.001).
for early discontinuation was a clinical adverse expe-rience (15, 4%)
There was no apparent effect of any of the sub-
groups studied on preference for dosing regimen
Of the 396 participants who completed the ques-
(Also, responses were similar regardless of
tionnaire and experienced both regimens, 364 (92%)
expressed a preference for one of the two treatmentregimens. Of these, 305 (84%) preferred the once
weekly regimen and 59 (16%) preferred the once dailytreatment regimen The preference for the
Of the 406 randomised participants who took at
once weekly regimen was statistically significant (P <
least one dose of study medication, 403 participants
0.001). The preference for the once weekly regimen
took at least one weekly dose and 399 took at least one
was similar in the two sequence groups, with 149
daily dose. Of these participants, 99 (25%) had an ad-
(84%) of those who took the once weekly regimen
verse experience during the weekly regimen and 110
first expressing a preference for once weekly, and 156
(28%) during the daily regimen. The most frequently
(84%) of the participants who took the once daily reg-
occurring adverse experiences were in the categories
Fig. 3. Participant responses to questionnaire on parameters of preference, convenience and willingness to take long term after experiencingboth alendronate once weekly and once daily regimens. P < 0.001 for each parameter. D. Kendler et al. / Maturitas 48 (2004) 243–251
A similar study of alendronate conducted in a US
population demonstrated similar results to our inter-
national study indicating a preference for once
weekly dosing regardless of country of residence.
These two studies are the first to investigate patientpreference for weekly dosing as compared to daily
dosing for a chronic condition. Other oral medica-
tions are dosed weekly, including chloroquine and
More than 75% of time with a concomitant medication
arthritis cabergoline for prolactinoma anti-
fungals such as fluconazole and fluoxetine
for continuation therapy for depression Whether
patients would also prefer weekly therapy to daily for
these other medications is not known.
Information about patient preference for dosing reg-
imens also can be obtained from anecdotal experiences
and from surveys of a target patient population. How-ever, each of these approaches has drawbacks. There
Number of concomitant chronic medications
are few reports of preference in dosing regimen after
allowing volunteers to experience different regimens,
and none that have addressed this issue for weekly dos-
Preference for once weekly dosing with alendronate was sim-
ilar regardless of subgroup tested, including country of residence
ing for osteoporosis. This trial was designed to mimic
clinical practice as much as possible in the clinical trialsetting. The randomised, open-label, crossover design,with 4 weeks allotted for each regimen, was chosen to
of body as a whole (10% and 8% for once weekly and
allow the participants an adequate amount of time on
once daily respectively) and digestive system (7% and
each regimen to assess their preference. Four weeks
10%, respectively). The occurrence of adverse expe-
was chosen as an adequate amount of time to assess
riences (among participants who received at least one
how well the regimen is received by the participant in
dose of both regimens) was not statistically different
relation to her usual daily and weekly activities. The
between the two treatment regimens (P = 0.158).
4-week treatment period for each regimen was cho-sen to be short enough to minimize recall bias. Thestrength of the results of this study was confirmed by
4. Discussion
the lack of sequence effect on the results, suggestingthat recall bias did not occur in this trial.
In this study, we investigated the attitudes among
Patient preference for a therapy may also be deter-
postmenopausal women from 19 countries toward two
mined by factors other than dosing regimen. Efficacy,
alendronate dosing regimens, once weekly or once
safety, and tolerability (whether perceived or real) will
daily dosing, for treatment of osteoporosis. For the ma-
also be important factors in preference for one therapy
jority of the women, the once weekly regimen was the
or regimen over others. In this study, attempts were
one they preferred, found more convenient, and would
made to design the trial to focus solely on the treat-
be more willing to take for a long period of time (84,
ment regimen itself. We attempted to minimise any
87, and 84%, respectively). Understanding patient at-
perceptions of differential effects on efficacy by stating
titudes toward various dosing regimens is an impor-
to the participants, consistent with controlled clinical
tant aspect of understanding which regimens are likely
trial data that the once weekly and the once daily
to enhance compliance to therapy, especially for dis-
regimens had similar efficacy. Also, no efficacy param-
orders such as osteoporosis which require long-term
eters were tested during the study. No such statements
were made about tolerability and therefore perceived
D. Kendler et al. / Maturitas 48 (2004) 243–251
tolerability, at least for some participants, may have
nant women led to higher compliance than did daily
been a factor that influenced their preference for one
regimen over the other. Patient preference may also be
100% compliance with the once weekly regimen than
influenced by the perceptions of the investigators and
with the daily regimen (97% versus 86%). Effective-
study site personnel. We believe this potential bias is
ness in reducing fractures in osteoporotic patients in-
minimal in this study because the study was performed
volves not only administration of an effective therapy
prior to the availability of the once weekly alendronate
but also administration of a therapy that the patient is
regimen in the marketplace, because physicians had
willing to take. Whether better long term compliance
minimal prior experience with once weekly oral reg-
with treatment for osteoporosis can be achieved with
imens for chronic conditions, and because of the ini-
regimens designed to enhance patient convenience and
tial skepticism expressed by many physicians about
preference deserves additional investigation.
patients’ willingness to take a weekly rather than the
In determining the best therapy for a particular pa-
tient, efficacy and tolerability are important considera-
To allow for adequate absorption, very specific dos-
tions. In addition, ease of use and dosing convenience
ing instructions are recommended for the bisphospho-
are important features to consider to encourage long
nates, including alendronate. These instructions may
term compliance to therapy for chronic conditions
be restrictive for some, especially for daily adminis-
such as osteoporosis. This study demonstrated that,
tration. The need to follow these strict dosing instruc-
compared to once daily dosing, the once weekly dos-
tions only once a week may have been a substantial
ing regimen with alendronate was preferred, was more
factor in the preference for weekly over daily dosing.
convenient, and was the regimen patients were more
Whether similar preference for weekly over daily dos-
willing to take for a long period of time. For chronic
ing would be seen for a therapy with fewer dosing
therapy such as is required for osteoporosis, it is im-
restrictions cannot be determined from this study.
portant for physicians to consider patient preferences
The participants’ assessment of the dosing regimens
in order to help optimise compliance to therapy.
in this study was limited to the three questions in theDosing Regimen Questionnaire. Qualitative informa-tion about reason for the preferred regimen was not
Acknowledgements
collected. In the subgroup analysis we investigated
We would like to thank Larry Radican and Julie
factors that may be associated with a preference for
Chandler for contributing their expertise to the de-
one regimen over the other, including age, country of
velopment of the Dosing Regimen Questionnaire. We
residence, and complexity of coexisting medical care
would like to acknowledge both the women partici-
as measured by presence of concomitant medication
pants, without whom this investigation would not have
use, number of active medical conditions (other than
been possible, as well as the contributions of the per-
osteoporosis), and number of concomitant medica-
sonnel at the study sites. Funding as well as study
tions. In addition, we evaluated the preference in sub-
medication, monitoring, and statistical support were
groups with common active medical conditions. All
of the subgroups investigated not only preferred theonce weekly regimen, but also had a similar prefer-ence for the once weekly regimen to that of the overall
References
cohort. We were unable to identify any characteristicsthat might suggest a group of patients more likely to
[1] McDonald HP, Garg AX, Haynes RB. Interventions to
enhance patient adherence to medication prescriptions:
Compliance with medications for chronic diseases
scientific review. JAMA 2002;288:2868–79.
is low and methods to improve compliance have been
[2] Claxton AJ, Cramer J, Pierce C. A systematic review of
a subject of interest for many years It is
the associations between dose regimens and medicationcompliance. Clin Ther 2001;23:1296–310.
well established that once daily dosing as compared
[3] Schnitzer T, Bone HG, Crepaldi G, et al. Therapeutic
to more frequent dosing regimens leads to enhanced
compliance Weekly iron supplementation in preg-
alendronate 10 mg daily in the treatment of osteoporosis. D. Kendler et al. / Maturitas 48 (2004) 243–251
Alendronate Once-Weekly Study Group. Aging (Milano)
[10] Nolting SK, Sanchez Carazo S, De Bouille K, Lambert
JR. Oral treatment schedules for onychomycosis: a study of
[4] Senn S. Cross-over trials in clinical research. Chichester:
patient preference. Int J Dermatol 1998;37:454–6.
[11] Gupta AK, Dlova N, Taborda P, et al. Once weekly
[5] Simon JA, Lewiecki EM, Smith ME, Petruschke RA,
fluconazole is effective in children in the treatment of Tinea
Wang L, Palmisano JJ. Patient preference for once-weekly
capitis: a prospective, multicentre study. Br J Dermatol 2000;
alendronate 70 mg versus once-daily alendronate 10 mg:
a multicenter, randomized, open-label, crossover study. Clin
[12] Burke WJ, Hendricks SE, McArthur-Miller D. Weekly
dosing of fluoxetine for the continuation phase of treatment
[6] Lobel HO, Bernard KW, Williams SL, Hightower AW,
of major depression: results of a placebo-controlled rando-
Patchen LC, Campbell CC. Effectiveness and tolerance of
mized clinical trial. J Clin Psychopharmacol 2000;20:423–
long-term malaria prophylaxis with mefloquine. Need for a
better dosing regimen. JAMA 1991;265:361–4.
[13] Rudd P. Clinicians and patients with hypertension: unset-
[7] Lobel HO, Miani M, Eng T, Bernard KW, Hightower AW,
tled issues about compliance. Am Heart J 1995;130:572–
Campbell CC. Long-term malaria prophylaxis with weekly
mefloquine. Lancet 1993;341:848–51.
[14] Eraker SA, Kirscht JP, Becker MH. Understanding and
[8] Bannwarth B, Labat L, Moride Y, Schaeverbeke T. Metho-
improving patient compliance. Ann Intern Med 1984;100:
trexate in rheumatoid arthritis. An update. Drugs 1994;47:
[15] Ridwan E, Schultink W, Dillon D, Gross R. Effects of weekly
[9] Biller BM, Luciano A, Crosignani PG, et al. Guidelines for
iron supplementation on pregnant Indonesian women are
the diagnosis and treatment of hyperprolactinemia. J Reprod
similar to those of daily supplementation. Am J Clin Nutr
PRESS RELEASE -/ ACTIVE AGAINST CANCER immatics ’ renal cancer vaccine IMA901 completes phase 3 patient recruitment and is granted US orphan drug designation by the FDA Tuebingen, 08. November 2012 - immatics biotechnologies GmbH, a biopharmaceutical company developing rationally designed therapeutic vaccines that are active against cancer, announced today that it has completed patient
Session II- Clinical Overview of PNDs , Andrea Gropman-Chair The disorders known collectively as "pediatric neurotransmitter disorders" consists of several possibly under-recognized, recently identified errors of metabolism that affect the production of neurotransmitters. Neurotransmitters have vast CNS effects, controlling aspects of memory and cognition, temperature regulation, pain

 Patients with osteoporosis prefer once weekly to
David Kendler , Annie Wai Chee Kung , Ghada El-Hajj Fuleihan ,
José Gerardo González González , Keavy A. Gaines ,
a St. Vincent’s Hospital, 120-809 W 41 Avenue, Vancouver, BC, Canada V5Z 2N6
b Queen Mary Hospital, Hong Kong, PR China
c American University of Beirut Medical Center, Beirut, Lebanon
d Universidad Autónoma de Nuevo León, Monterey, Nuevo León, Mexico
e Merck and Co. Inc., Whitehouse Station, NJ, USA
f Merck Sharp and Dohme Inc. (Europe), Brussels, Belgium
Received 17 July 2003; received in revised form 17 December 2003; accepted 17 December 2003
Abstract
Patients with osteoporosis prefer once weekly to
David Kendler , Annie Wai Chee Kung , Ghada El-Hajj Fuleihan ,
José Gerardo González González , Keavy A. Gaines ,
a St. Vincent’s Hospital, 120-809 W 41 Avenue, Vancouver, BC, Canada V5Z 2N6
b Queen Mary Hospital, Hong Kong, PR China
c American University of Beirut Medical Center, Beirut, Lebanon
d Universidad Autónoma de Nuevo León, Monterey, Nuevo León, Mexico
e Merck and Co. Inc., Whitehouse Station, NJ, USA
f Merck Sharp and Dohme Inc. (Europe), Brussels, Belgium
Received 17 July 2003; received in revised form 17 December 2003; accepted 17 December 2003
Abstract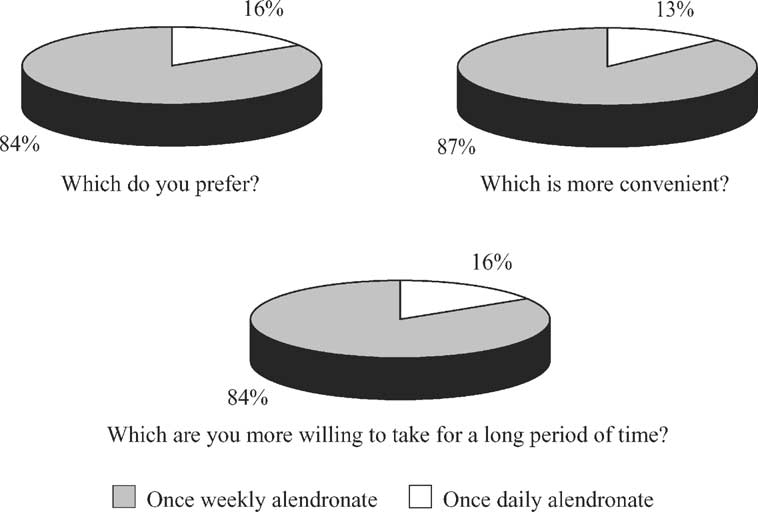 D. Kendler et al. / Maturitas 48 (2004) 243–251
hypertension (114, 28%), osteoarthritis (46, 11%), hy-
imen first preferring the once weekly regimen. There-
percholesterolemia (36, 9%) and hypothyroidism (32,
fore, no effect by sequence was seen (P = 1.000).
D. Kendler et al. / Maturitas 48 (2004) 243–251
hypertension (114, 28%), osteoarthritis (46, 11%), hy-
imen first preferring the once weekly regimen. There-
percholesterolemia (36, 9%) and hypothyroidism (32,
fore, no effect by sequence was seen (P = 1.000).