Evolving US Safety Regulations and Risk Management Programmes The US Risk Evaluation and Mitigation Strategies (REMS) entered into the iPLEDGE system before a script can be filled. requirements for a drug or drug class are continuously Components include: evolving. The FDA solicits feedback and collaborates with • Applications development and hosting pharmaceutical companies in an effort to find the right • Adverse event management balance between patient risks and benefits. Much of the REMS • Data analysis and reporting design has evolved from earlier work on risk management • Document production and fulfilment programmes and RiskMAPs.
• Patient surveys via web and IVR• Call centre management
A. Roche/Genentech – Accutane Risk Management
Roche and Genentech (recently acquired by Roche), have • Education materials design & update had extensive experience with the FDA’s changing risk • Assessmentsmanagement requirements. Nine Roche medicines have risk • Performance-linked access system requiring programmes with mature drugs, across several therapeutic
pregnancy test results and contraception choices
areas. Two of these products, Accutane® for acne and
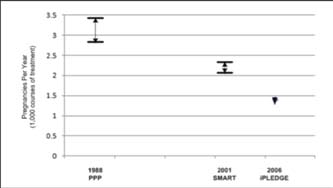
Chart 1 Impact of Isotretinoin Risk Management on Pregnancy Rates
Cellcept® for transplants, require ETASU, registries, and implementation systems, in addition to medication guides and communication plans, in an effort to avoid birth defects.
Roche launched its first voluntary Accutane risk
management programme in May 1988, called the Pregnancy Prevention Program (PPP). The PPP was a voluntary programme for both the prescriber and the patient. Its second programme, System to Manage Accutane Related Teratogenicity (SMART) was launched in April 2000, responding to new FDA restrictions. It required mandatory participation by both the prescriber and female patients.
In February 2002, Roche’s patents for the drug isotretinoin
expired. There are now many other companies selling less expensive, generic versions of the drug. Once generic As can be seen in Chart 1, each new risk management manufacturers entered the market, risk management was no programme decreased the frequencies of pregnancy while longer centralised.
patients were treated with isotretinoin. With the PPP
Since March 2006, the dispensing of isotretinoin in the programme, there were 2.8 to 3.4 pregnancies per 1000
United States has been controlled by an FDA-mandated courses of treatment. The SMART programme resulted in website called iPLEDGE. iPLEDGE requires dermatologists 2.1 to 2.3 pregnancies per 1000 courses of treatment. And to register their patients before prescribing the medication. iPLEDGE produced the least number of pregnancies, 1.3 Pharmacists are then required to check the website or call a pregnancies per 1000 female users of the programme.2,3 call centre to determine if the patient has registered before dispensing the drug. Additionally, doctors and pharmacists B. Amgen and Johnson & Johnson (ESA Class REMS) must verify written prescriptions in the iPLEDGE system In 2008, the FDA required Amgen to provide an ESA class- before patients may fill the prescription. And, women must wide REMS programme for cancer patients. Amgen is currently be on a form of birth control.1 The prescription may not be the sole manufacturer of FDA-approved ESAs, and Johnson & dispensed until both parties have complied.
Johnson’s Janssen is a marketing and distribution partner on
On June 29, 2009, Roche Pharmaceuticals, the original Procrit. The risks to be managed in this class were based on
creator and distributor of isotretinoin, officially discontinued studies that found ESAs caused tumours to grow faster and both the manufacture and distribution of their Accutane brand resulted in earlier deaths in certain cancer patients. in the United States. Generic isotretinoin remains available in To meet the FDA requirements, Amgen and Johnson & the United States through Teva, Ranbaxy and Mylan.
Johnson’s Janssen jointly co-developed a programme called
Since the iPLEDGE programme pre-dates REMS, which APPRISE (Assisting Providers and Cancer Patients with Risk
assigns responsibility for the REMS programme to the NDA Information for the Safe Use of ESAs). holder, iPLEDGE was and continues to be sponsored by all isotretinoin manufacturers. It is a mandatory programme for The programme includes the following components. prescribers, all patients (male and female), dispensers and wholesalers. IPLEDGE is a technology-based system, using Physician Tracking both a phone and a web interface (www.ipledgeprogram.
• Physician registrations faxed or mailed to a third-party call
com) that tracks all registrations. ETASU requires a monthly
centre that oversees and monitors compliance
pregnancy test by a CLIA-certified lab, and results need to be • Documentation of HCP’s completion of training on ESA usage
22 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
• Discussion of the risks, benefits, and approved usage of CarePoints® and Catalina’s PatientLink®. HCP on-demand
ESAs with each patient before they begin treatment
printing is gaining acceptance with systems such as LDM
• Written acknowledgment from both the doctor and patient Group’s ScriptGuide®.
that the discussion took place, which are then faxed or
Also, systems for reporting adverse events have a long-
established track record, with available solutions such as
• Re-enrolment in the programme every three years
the FDA’s MedWatch website, the Relsys Argus Safety data management and regulatory reporting system, Oracle AERS,
Hospital Tracking
• Dispensing hospitals designate who “assumes the authority
and responsibility” to internally coordinate and oversee the
The Missing Link
institution’s programme (often the pharmacy manager)
The missing link in REMS ETASU programmes is the feedback
• Documentation of hospital’s designee’s completion of loop among the prescriber, the lab (when required), and
the pharmacy, which is still paper-based, taxing HCPs and
• Compilation of lists of everyone at the hospital who pharmacies with overly burdensome administrative processes.
Fortunately, technologies such as iReminder’s MedTriggerSM
• Proof that each one has enrolled in APPRISE
can automate communications among these stakeholders.
• Archive of the written acknowledgments from every cancer
Help Patients Comply with Scheduled Tests Patients need to complete lab tests in a timely manner to Pharmacy Tracking
avoid lapses in their prescription refills. To help patients stay
• Validating the prescriber is an approved APPRISE on schedule, MedTrigger schedules automated reminders.
Reminders are scheduled to be delivered to patients prior
• Receipt of acknowledgement of patient discussion with to their anticipated lab dates (e.g. two weeks, one week and
two days before) and to confirm that patients will keep their scheduled appointment. When patients report that they will
APPRISE Website
not go, MedTrigger automatically generates alerts to the
The APPRISE website, www.esa-apprise.com, provides online HCP and the pharmacy. To accommodate different patient access to physicians and hospitals to the following literature lifestyles, MedTrigger contacts the patient according to their and forms:
preferred method of communication (email, phone, SMS text,
iPhone app). If a patient is not reached at one destination,
the system then escalates to the patient’s next preferred
location. Furthermore, multiple attempts are made at each
• Dear Healthcare Provider (DHCP) Letters to HCPs
location until the patient has been reached. This technology
• REMS Flashcard (prescriber checklists)
ensures that every effort is made to reach the patient.
• Provider Flashcards (prescriber process flowchart)• HCP Training Module
Best Practices and Recommendations
We propose a list of best practices and recommendations
(HCP) for implementing REMS. These programmes are still in
their infancy and we see opportunities to create effective
programmes that will benefit all stakeholders.
• Dear Healthcare Provider (DHCP) Letter to Hospital
Facilitate Communications
While elements may differ, the foundation of a REMS
programme is communications among healthcare providers,
pharmacists and patients, as mandated by the FDA. Currently,
most of these communications are pre-printed and paper-
• Patient Instructions for Use (for self-administration)
based. Furthermore, HCPs and pharmacists have to deal with multiple suppliers rather than a single electronic source for
C. Amgen Nplate (romiplostim) and GlaxoSmithkline’s generating print materials. Even worse, when documents are ProMacta (eltrombopag)
The REMS programme for Nplate and ProMacta, both drugs used to stimulate the production of blood platelets, but We recommend automating these communications manufactured by different companies, have very similar whenever possible, replacing them with online systems to REMS implementations. The FDA may have worked with both improve efficiencies and reduce administrative work for all manufacturers to achieve this level of harmonisation.
• There will be a single electronic source for generating
Current Trends
On-demand printing of medication guides and patient
• Adequate documents will always be available
package inserts (PPIs) has become part of standard pharmacy
• Storage and retrieval of documents will be efficient
operating procedures with systems such as LDM Group’s
24 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Improve Patient, HCP and Pharmacy Compliance
Following the model established by Roche, we recommend
Compliance levels with REMS programmes are low because that NDA and ANDA holders share REMS programme they interrupt the workflow4 of HCPs and pharmacists and development costs. Ongoing maintenance costs should be because the implementation of REMS elements is a manual adjusted based on relative market share. process5. Even the most efficient HCP offices and pharmacies Furthermore, efficiencies are extremely critical when generic find adherence to these programmes challenging. HCP sponsors join the REMS programme, since they do not have offices and pharmacies would, therefore, benefit greatly the same depth of relationships with stakeholders, nor do from automation. Examples include:
they have comparable internal infrastructure systems.
• IVR, email and SMS text reminders to patients to remind
them of upcoming laboratory testing and refill dates
Automate Reporting Systems
• Alerts to HCP and pharmacies when patients report that Every REMS programme includes an assessment timeline that
they will not comply with laboratory testing or refill pick-
typically involves a public review of the programme’s impact
at 18 months, or after 10,000 patient exposures. Under
• Distribution and printing of medication guides at the FDAAA, the agency is required to “prepare…a summary
analysis of the adverse drug reaction reports received for the
They also would benefit from online access for:
drug, including identification of any new risks not previously
• Pharmacies to determine certification status of HCPs
identified, potential new risks, or known risks reported in
• Prescribers and wholesalers to determine certification an unusual number.” Improved automation will provide the
metrics and improve the reporting necessary to evaluate and
• HCP and pharmacist training and certification
continuously advance REMS programmes.
• Storage of HCP and patient agreement documents
Standardise Requirements Integrate REMS Programme with Pharmacy Management The key to success for REMS programmes is the Systems and HCP Systems
standardisation of requirements and uniform methods in
The FDA requirement that medication guides be printable design and implementation. And even more importantly, to from PDF formats has slowed the adoption of electronic link REMS to electronic medical records, health plans, and medication guides in mainstream pharmacy practice to other adverse event programmes, so that the healthcare management systems. However, new solutions, such as on-
system will have the information it needs to effectively treat
demand printing of medication guides, are being integrated diverse patient populations. into systems such as QS/1 and SpeedScript using LDM’s CarePoints®. Similar on-demand printing for HCPs office is Referencesbeginning to emerge as well.
1. iPLEDGE Year 1 Review. http://www.fda.gov/ohrms/dockets/ac/07/slides/2007-4311s1-04-sponsor-group.pdf Accessed Prepare for the Growth of the Generic Drugs Market
When new drug applications (NDAs) are filed with the FDA, 2. Abroms L, Maibach E, Lyon-Daniel K, Feldman SR (2006). What the REMS accountability remains with the NDA holder and
is the best approach to reducing birth defects associated with
leads coordination among all new sponsors. Therefore,
isotretinoin? PLoS Med. 2006;3:e483.
pharmaceutical sponsors facing generic competition down 3. U.S. Food and Drug Administration Briefing document for the road should automate for efficiency so that their workload
is abbreviated when new drug applications (ANDAs) are 4. “Use of Medication Guides to Distribute Drug Risk Information approved.
to Patients”, Gerald K. McEvoy, Pharm. D., FDA Public Hearing, June 12 and 13, 2007 http://www.fda.gov/downloads/Drugs/
We recommend that NDA holders draft a memorandum of
DrugSafety/UCM173475.pdf Accessed 23 May 2010.
understanding (MOU) for all ANDAs and sponsors to sign, 5. Nourjah P, Lee L, Kortepeter C, Avigan M, FDA Office of Drug which contains:
Safety. National Survey of Pharmacists to Assess Awareness of Drug Risk Communication Tools; 2005.
• Ownership rights of intellectual properties
6. www.fdli.org/conf/handouts/Reshef.pdf
• Cost-sharing structure• Contracts regarding cost-sharing and third-party call
Jean Steckler is the Senior Vice President
• Share of voice and escalation process
• The roles and responsibilities of each company’s
dosing, appointment reminders and refill
• Governance (how programme is governed among
reminders; Global e-Trials™ for patient
recruitment to and retention in clinical
trials; and MedTrigger™ a REMS program that reminds patients to comply with al events required by their risk management plan. Email: [email protected]
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 25
Technisches Merkblatt Holzschutzsysteme profilan®-prevent Wasserbasierende, farblose Grundierung mit bioziden Wirkstoffen zum vorbeugenden Schutz gegen Bläue, Schimmel, Pilze und Insekten. RAL-Gütesiegel, Verleihungsurkunde Nr. 871 Anwendungs- profilan®-prevent dient dem Schutz statisch nicht beanspruchter Hölzer ohne Erdkontakt im Außenbereich vor Insekten
Curriculum Vita ALAN P. SIEGAL, M.D. EDUCATION: 1975, B.A., Magna Cum Laude, Adelphi University, Garden City, New York: Biology 1979, M.D., University of Louisville School of Medicine, Louisville, Kentucky BOARD CERTIFIED IN GERIATRIC AND ADULT PSYCHIATRY POST GRADUATE TRAINING: 1979-80 Intern in Medicare, Norwalk Hospital, Norwalk, CT Resident Psychiatry, Yale University S
 Evolving US Safety Regulations and
Evolving US Safety Regulations and  Improve Patient, HCP and Pharmacy Compliance
Improve Patient, HCP and Pharmacy Compliance