 European Journal of Echocardiography (2008) 9, 426–427doi:10.1093/ejechocard/jen022
Cardiac complications in Whipple’s disease
Department of Cardiology, Klinik Koesching, University Heidelberg, Krankenhausstr. 19, D-85092 Koesching, Germany
Received 2 November 2007; accepted after revision 23 December 2007; online publish-ahead-of-print 30 March 2008
Whipple’s disease or intestinal lipodystrophy is an infection induced by Tropheryma whipplei. It is rare
with an estimated incidence of 0.4 per million. Symptoms are arthropathy, weight loss, and diarrhoea,
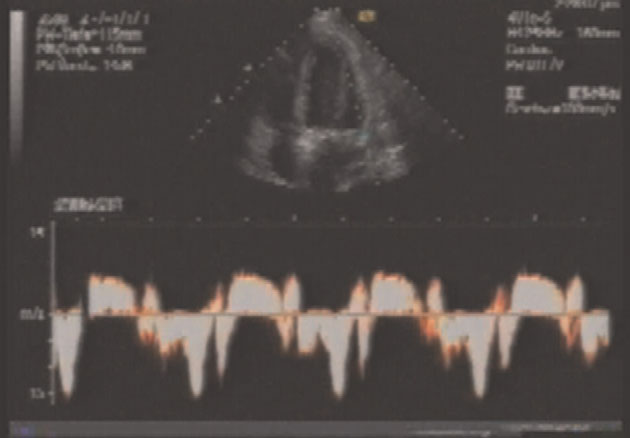
but other organs notably the central nervous system may be affected. We demonstrate a case of cardiac
complications in Whipple’s disease. The patient presented with endocardial infiltrations on TEE exam-inations and heart failure and improved after antibiotic treatment.
European Journal of Echocardiography (2008) 9, 426–427doi:10.1093/ejechocard/jen022
Cardiac complications in Whipple’s disease
Department of Cardiology, Klinik Koesching, University Heidelberg, Krankenhausstr. 19, D-85092 Koesching, Germany
Received 2 November 2007; accepted after revision 23 December 2007; online publish-ahead-of-print 30 March 2008
Whipple’s disease or intestinal lipodystrophy is an infection induced by Tropheryma whipplei. It is rare
with an estimated incidence of 0.4 per million. Symptoms are arthropathy, weight loss, and diarrhoea,
but other organs notably the central nervous system may be affected. We demonstrate a case of cardiac
complications in Whipple’s disease. The patient presented with endocardial infiltrations on TEE exam-inations and heart failure and improved after antibiotic treatment.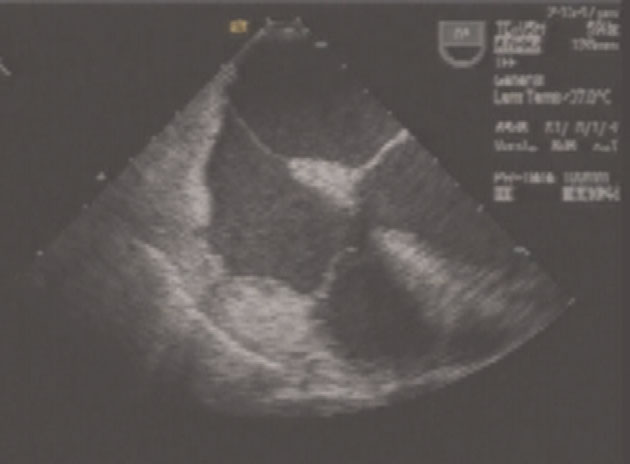
 Cardiac complications in Whipple’s disease
Differential diagnosis of these intracardiac abnormalitieswould include congestive heart failure, ischaemic cardio-myopathy, hypertrophy due to hypertension or aortic steno-sis, viral myocarditis, nutritive or toxic cardiomyopathy, orFabry disease. However, the reaction on antibiotic therapysupports our view of a cardiac complication of Whipple’sdisease in this case.
Cardiac complications in Whipple’s disease
Differential diagnosis of these intracardiac abnormalitieswould include congestive heart failure, ischaemic cardio-myopathy, hypertrophy due to hypertension or aortic steno-sis, viral myocarditis, nutritive or toxic cardiomyopathy, orFabry disease. However, the reaction on antibiotic therapysupports our view of a cardiac complication of Whipple’sdisease in this case.aups.org.au
Membrane transporters regulating inhibitory neurotransmitter signaling in health and disease A.J. Moorhouse,1,2 M. Watanabe2 and J. Nabekura,2 1School of Medical Sciences, The University of New South Wales, NSW 2052, Australia and 2National Institute for Physiological Sciences (NIPS), Okazaki 444-8585, Japan. The efficacy of inhibitory signalling at GABA and glycinergic synapses depends on a