Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
704 340.349
Antiepileptic Treatment in Paediatric Oncology –
Antiepileptische Therapie in der pädiatrischen Onkologie –
Epileptic seizures are a common and clinically relevant problem
Epileptische Anfälle stellen in der pädiatrischen Onkologie ein
in paediatric oncology. Attributable to the heterogeneity of this
häufiges und klinisch relevantes Problem dar. Bedingt durch die
group of patients and a number of possible comorbidities anti-
Heterogenität der betroffenen Patientengruppe und einer Viel-
epileptic treatment in paediatric oncology poses a number of di-
zahl von möglichen Komorbiditäten sind sowohl das diagnos-
agnostic and therapeutic challenges. This requires a close inter-
tische Vorgehen als auch die antikonvulsive Therapie eine be-
disciplinary approach to the seizing child or adolescent. A
sondere Herausforderung, die ein interdisziplinäres Vorgehen
prompt and detailed diagnostic work-up is needed in every case
erfordert. Diagnostisch sind neben einer Vielzahl von potenziell
in order to establish the diagnosis and, equally important, to de-
epileptogenen Medikamenten vor allem akute Begleiterkran-
tect secondary aetiological factors, e. g. epileptogenic drugs or
kungen im Verlauf der Krebstherapie zu berücksichtigen, die ur-
any acute underlying pathology, such as metabolic or toxic ence-
sächlich für das Auftreten von Anfällen sein können. Beispiele
phalopathies, CNS-infections or cerebrovascular events. This
sind metabolische oder toxische Encephalopathien, ZNS-Infek-
might offer the opportunity for a specific causative treatment
tionen oder auch zerebrovaskuläre Ereignisse. Da diese zum Teil
and thus prevent unnecessary long-term antiepileptic drug
lebensbedrohlichen Erkrankungen zum Teil kausal behandelbar
(AED) treatment. If AED treatment is initiated several aspects
sind, erfordert jedes anfallsverdächtige Ereignisses eine rasche
have to be taken into account. Most importantly, AEDs and che-
und umfassende Abklärung. So können spezifische Ursachen er-
motherapeutic drugs (CTDs) may interact. Depending on the co-
kannt und behandelt sowie unnötige antikonvulsive Langzeit-
medication this may result in reduced tumour or seizure control
therapien vermieden werden. Besteht eine Therapieindikation
or unexpected toxicity of AEDs or CTDs. Understanding these in-
zur antikonvulsiven Dauertherapie so liegt die Schwierigkeit pri-
teractions will allow to anticipate clinically relevant adverse ef-
mär in einer Vielzahl von Komedikationen und damit der Gefahr
fects. AED may be further complicated by side-effects, some of
von Wechselwirkungen insbesondere zwischen Antikonvulsiva
them of particular concern for children or adolescents, such as
und Chemotherapeutika. Das Wissen um diese Wechselwirkun-
cognitive effects, myelotoxicity, serious rashes, endocrinological
gen ist wichtig, da sowohl die Prognose der Krebserkrankung, als
disturbances, and many more. Beside critically questioning the
auch die der Epilepsie hierdurch nennenswert beeinflusst wer-
need for AED treatment it is therefore important to prefer AED
den kann. Zusätzlich erschweren eine Reihe onkologisch rele-
with a good safety-profile in this population. Enzyme-inducing
vanter Nebenwirkungen die Entscheidungsfindung bei der Aus-
and inhibiting AED should be avoided if possible. Preliminary
wahl der Antiepileptika. Dies betrifft z. B. kognitive Nebenwir-
studies indicate that gabapentin and levetiracetam may provide
kungen, myelotoxische Wirkungen, Dermatosen, endokrinolo-
Affiliation1 Department of General Paediatrics, University Children’s Hospital, Düsseldorf, Germany2 Clinic for Paediatric Oncology, Haematology and Immunology, University Children’s Hospital, Düsseldorf,
CorrespondenceDr. Daniel Tibussek · Department of General Paediatrics · University Children’s Hospital · Moorenstrasse 5 ·40225 Düsseldorf · Germany · Tel.: +49/211/8 1176 87 · Fax: +49/211/8 1187 57 ·E-mail: [email protected]
BibliographyKlin Pädiatr 2006; 218: 340–349 Georg Thieme Verlag KG Stuttgart · New YorkDOI 10.1055/s-2006-942257ISSN 0300-8630
good options in terms of efficacy and safety. However, more
gische Effekte und andere mehr. Neben der kritischen Indika-
properly designed clinical studies are warranted to raise the lev-
tionsstellung einer antikonvulsiven Therapie gilt es daher bevor-
el of evidence for robust clinical recommendations. Until that
zugt Antikonvulsiva einzusetzen, die ein günstiges Nebenwir-
time, clinicians will need to continue to question current policies
kungsprofil in dieser Patientengruppe haben und zusätzlich
and adapt their daily practice to evolving scientific data.
durch fehlende Enzyminduktion bzw. Inhibition gekennzeichnet
sind. Nach aktuellem Kenntnisstand scheinen hier vor allem Ga-
bapentin und Levetiracetam günstige Optionen darzustellen. An-
gesichts einer sehr schlechten Studienlage sind jedoch weitere
klinische Studien zu diesen wichtigen Fragestellungen dringendzu fordern, aktuelle Therapieregime kritisch zu hinterfragen und
gegebenenfalls der aktuellen Datenlage anzupassen.
Cancer · seizures · antiepileptic drugs · drug interaction
Krebs · Krampfanfälle · Antiepileptika · Wechselwirkungen
The current review aims to summarize some key aspects of antic-
onvulsive treatment in paediatric oncology. We also intend to criti-
cally question some current clinical policies and point out areas
suitable for future interdisciplinary research in this field.
Aetiology of seizures in paediatric oncology
The exact pathophysiology of seizures during the course of ma-
lignant diseases is often multifactorial and not well understood.
Seizures in patients with brain tumours are usually directly re-
lated to focal cerebral damages and effects on the surrounding
non-tumoural, cerebral tissue. This may be due to the tumour it-
self or to anti-cancer treatment (neurosurgery, irradiation, che-
motherapy). Etiological mechanisms include theories of altered
peritumoural amino acids, changes in regional metabolism in-
volving pH, neuronal or glial enzyme and protein expression,
and localized immunological changes. Distribution and function
of the NMDA subclass of glutamate receptors may also play a
role [3]. Certain tumours (e. g., oligodendroglioma, DNET, gang-
lioglioma) and tumour localisations appear to be associated
with a higher seizure risk (see Table 1 and 2). However, there is
some variation in seizure incidence even within a single histolo-
gical tumour subtype. Therefore, reliable risk factors are cur-rently difficult to define particularly in the paediatric age group,
Seizures are a common complication in paediatric oncology and
where only limited data are available [36].
often significantly impact the quality of life of patients and rela-
tives. This applies not only to children with brain tumours, where
an incidence of up to 70 % depending on the type of tumour has
been reported [30], but also to systemic malignancies. A sizable
Possible risk factors for seizure occurrence in patients with
proportion of patients with systemic cancer present with at least
one seizure during the course of the disease. As an example, in
possible risk factors for seizures in brain tumours
children and adolescents with acute lymphoblastic leukaemia a
seizure prevalence between 8 and 13 % has been reported [45,
lower-grade, slower growing tumours (epilepsy)
52, 76]. Aetiology includes a number of possibly preventable or
higher-grade rapidly progressive tumours (seizures at presentation)
treatable conditions, which may be directly related to secondary
effects of anti-cancer treatment. Moreover, anticonvulsive drug
treatment in this particular group of patients comprises a num-
ber of difficulties, making seizures an interdisciplinary challenge.
Apart from the potential for serious side effects of antiepileptic
drugs (AEDs), some of them of particular concern for children, re-
cent years have seen new appreciation of drug interactions with
AEDs that are important in neoplastic disorders.
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
Example of seizure incidence in paediatric brain tumours
In general, acute neurological symptoms under certain CTDs are
not uncommon [35, 55, 75]. The toxicity of CTDs to the central ner-
vous system is directly related to their ability to cross the BBB.
Clinical signs suggestive of neurotoxicity are usually non-specific:
altered level of consciousness, behavioural disorders and/or motor
deficits. Seizures are often part of the acute presentation [53].
The diagnosis of chemotherapy-induced seizures is made clini-
cally, and is based on the temporal relationship between drug
administration and neurological complication and, equally im-
portant, knowledge of side effects of specific agents. Therefore,
some clinically important CTDs associated with seizures are dis-
MTX has the potential to cause both acute and delayed neuro-
toxicity, particularly after intrathecal (i. t.) or high dose intrave-
nous (i. v.) administration [52, 58] The mechanism of MTX-re-
lated neurotoxicity is still unclear. An excess of homocystein
and consecutively of excitatory neurotransmitters has been
found in some children [57]. Neurotoxicity usually manifests as
seizures, occurring a median of 10–11 days after i. t. MTX. The
frequency of seizures or other acute CNS effects during ALL ther-apy in childhood has been reported at 3 to 13 % [17, 45]. Neuro-
toxicity is usually self-limited and the risk of recurrence appears
ASP has been repeatedly related to cerebrovascular complica-
tions, which may be related to deficiencies of antithrombin III,
plasminogen, and fibrinogen [55]. In a recent case series Kieslich
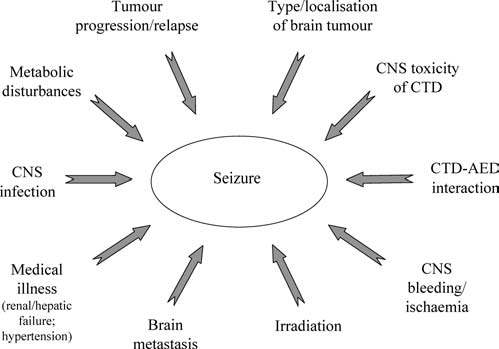
Possible aetiological factors of seizures in oncological patients.
et al. [38] reported five children with neurological complications
presenting with headache and seizures during the first three
In systemic cancer the aetiology may be even more complex (see
weeks of ASP treatment. Three patients had venous thrombosis,
Fig. 1). Indirect effects of the cancer or its treatment such as brain
one presented a parenchymal haemorrhage.
metastasis or leptomeningeal disease, hypertension, fever, CNS
infections, cerebral infarction or bleeding, electrolyte distur-
A study of DiMario and Packer [17] found that almost half of the
bances (hyponatraemia, hypocalaemia, hypomagnesaemia), me-
seizures occurring in children with systemic cancers were attri-
tabolic or toxic encephalopathies are possible reasons for epilep-
butable to complications of ASP treatment. The epileptogenic ef-
tic seizures. Chemotherapy and certain other drugs used for sup-
fect of L-asparaginase may result from cleaving asparagine and
portive care in oncology are epileptogenic, especially in patients
glutamine into aspartic acid, ammonia, and glutamate, an excita-
with an altered blood-brain barrier (BBB) (see Table 3). These
secondary effects are often associated with the type and time-
course of the underlying malignancy, type of CTD, comedica-
tions, and acute illnesses related to tumour treatment. From the
Encephalopathy is a known adverse effect of IFO. The pathophy-
clinical perspective it has to be stressed that a number of these
siology seems to be related to intoxication with chloracetalde-
aetiological factors are treatable and/or preventable [17].
hyde, a metabolic product of IFO [55]. The presentation and se-verity varies greatly and involves a clinical spectrum ranging
from subclinical electroencephalographic changes, complicated
seizures to coma. Nonconvulsive status epilepticus has been de-
Cancer treatment associated with seizure occurrence
scribed in children and adults under IFO with reduced level of
consciousness [39, 56]. Onset of symptoms may be within hours
of administration without evidence of a dose-response curve. It
asparaginase, etoposide (IA), interleukin-2, busulphan (HD), erythropoietin,levamisole, BCNU, 5-Fluorouracil, mechloramine, carboplatin (IA),
is generally self-limiting and reversible between 48 and 72 h after
fludarabine, methotrexate, chorambucil (HD), GM-CSF, mitotane, cytosine
discontinuation of IFO. However, severe and even fatal cases have
arabinoside (HD or IT), hexamethylmelamine, pentostatin, dacarbazine,
been reported [20]. Therefore, as effective therapy is available
ifosfamide, thalidomide, interferon (IT), vinca alkaloids
especially for patients with severe symptoms of toxicity early di-
HD: high-dose; IT: intra-thecal; IA: intra-arterial.
agnosis is essential (see Table 4; references [50, 54]. Whether re-
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
tial diagnosis of paroxysmal events in infancy and childhood andmisdiagnosis as epilepsy is common [35, 72] Conversely, more
Methylene blue in IFO-encephalopathy [54]
subtle ictal events such as confusion, sensory or autonomic
symptoms might be misinterpreted as non-epileptic. Therefore,
the most important help to diagnosis is the clinical history sup-
ported by detailed seizure description from a witness to the epi-
sode [9]. Further information can sometimes be obtained from
an EEG. However, a normal interictal EEG does not exclude epi-
lepsy and vice versa. The gold standard for diagnosis would be
administration should be performed under prophylactic treat-
video-EEG-monitoring in order to document an ictal event. How-
ment with methylen blue remains controversial. However, in
ever, in clinical practice this is often not feasible. In patients with
paediatric oncology, instead of re-administration replacement of
reduced consciousness a non-convulsive status epilepticus has
IFO by cyclophosphamide will usually be preferred.
to be strongly considered and early EEG should become a general
routine in such cases, particularly under certain CTDs, such as
CIS has principally been related to peripheral neurotoxicity.
However, CNS disorders such as the posterior reversible ence-
If a clear seizure has been documented it has to be differentiated
phalopathy syndrome (cortical blindness, hemiparesis, aphasia,
between a single seizure, which may be situation-related, and
and coma) and isolated seizures have also been reported. CIS-re-
epilepsy. Strong efforts have to be made to classify the patients
lated seizures may start within a few hours of the last CIS expo-
seizure, or less likely in oncology, place seizures in the context
sure, and are not related to the cumulative CIS dose. Usually
of an epilepsy syndrome. Seizures may be febrile or non-febrile.
these effects are completely reversible. Metabolic changes (e. g.
They might include a single symptom or have complex sympto-
hypocalcaemia, hypomagnesaemia, and hyponatraemia) may
matology. Description of seizures should be focused on precipi-
contribute to seizure susceptibility [75].
tating factors, the very initial ictal manifestations (aura? focal
onset?), and include the whole sequence of ictal symptoms as
well as postictal abnormalities. The initial symptomatology
BUS is a common component of conditioning regimens for haema-
may have localising value pointing to a specific seizure onset
topoietic stem cell transplantation. It rapidly crosses the BBB.
zone [60]. Seizures may be generalised (e. g. absences, tonic-clo-
Neurotoxicity is a widely known complication of high-dose BU,
nic, myoclonic) or partial (focal onset) with or without second-
with seizures occurring in up to 7.5 % of children without AED pro-
ary generalisation. Classification will often be essential for indi-
phylaxis [29]. Seizures may occur during BUS administration or
cation and selection of appropriate AEDs [27]. Brain tumour-re-
within 24 hours after the last dose, but seem to rarely happen be-
lated epileptic seizures are mostly focal, although generalization
fore the seventh dose [16, 29]. It is now common practice to give
is common and may occur so quickly that the focal phase re-
anticonvulsant prophylaxis along with high-dose BUS (see below).
mains unnoticed. Generalized seizures are more common in
children with systemic malignancies. It can be assumed that
most seizures in oncology will be symptomatic. However, there
Although not a classical CTD, CSA is often part of the therapeutic
may be cases where a genetic seizure susceptibility is unmasked
regime in oncology. Neurotoxicity is one of the most significant
by an acute illness and/or epileptogenic drugs.
clinical side effects of the CSA, occurring in up to 60 % of trans-
plant patients [66]. It is considered a drug with high epilepto-
Secondly, strong efforts have to be made to identify specific sec-
genic potential [62]. However, the mechanism is poorly under-
ondary effects that may have lead to increased seizure suscept-
stood. There might be some interference of CSA with mitochon-
ibility. In oncology some of these may even pose potentially life-
drial energy metabolism [66]. Neurotoxicity may occur during
threatening conditions, such as CNS infections or cerebral bleed-
long-term treatment even when blood concentrations of CSA are
ings, intoxications or metabolic encephalopathies. Importantly,
within the therapeutic range. Single seizures, status epilepticus
causal treatment of the underlying condition may be possible in
and development of the posterior reversible encephalopathy syn-
a relevant proportion of patients. Therefore, an aggressive diag-
drome have frequently been published. Dose reduction or with-
nostic work-up should be initiated promptly if a seizure occurs
drawal of CSA usually results in resolution of clinical symptoms.
during the course of a malignancy (see Fig. 2). Although cur-
rently not routinely performed, we propose to include detectionof drug levels of CTDs and/or their toxic metabolites (blood, CSF)
Diagnostic approach after first seizure in paediatric oncology
if possible. Toxic drug levels may be identified resulting in mod-
ification of therapy regimes. In addition, pooling these data with-
Due to the complexity and variability of the paediatric oncologi-
in clinical trials may enable clinicians to better understand the
cal population it is not possible to provide universal recommen-
pathophysiology of neurotoxicity of certain CTDs.
dations how to approach seizures in these children. However,
some general aspects of the diagnostic work-up of a child after
a first seizure have to be considered.
Treatment of seizures and epilepsy in paediatric oncology
Firstly, the importance of the correct diagnosis before initiation
In general, the clinical decision to initiate an AED is based on the
of AED treatment cannot be overstated. There is a wide differen-
judgement that the risk of seizure occurrence outweighs the risk
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
of AEDs and their possible toxic effects [21]. Predicting the risk of
age and sex of the patient, comorbidities, and comedications.
seizure recurrence forms another essential part of the decision for
An individualized approach is therefore required in any such
or against AED treatment. However, this may be particularly diffi-
case. We strongly suggest that a paediatrician with expertise in
cult in paediatric oncology. In general, seizure recurrence in chil-
epilepsies in children should always be involved in this complex
dren who suffered the first seizure during the intensive CTD treat-
decision process, the regular review of antiepileptic manage-
ment phase tends to be infrequent, usually occurring within three
to six months of the first seizure. Often, AED may be discontinued
shortly after the causative abnormality has been corrected, thus
preventing unnecessary initiation of long-term AED treatment
[30, 37]. Options may be treatment of CNS infections, correctionof electrolyte disturbances including the critical review of the cur-
A main challenge of AED treatment in paediatric oncology is the
rent hydration regime and/or diuretic treatment, correction of
high number of comedications to be expected in the majority of
blood sugar, discontinuation of potentially causal CTD, and, if
patients [43, 74]. This will inevitably imply the potential for
available, antagonistic treatment (e. g. IFO). If a CTD is likely causal
pharmacokinetic and pharmacodynamic drug interactions and
for seizure occurrence its indication, dosage, and infusion rate
it may be almost impossible to predict every pharmacological
should be critically questioned. In addition, the patient should be
modification caused by the variety of drugs given at the same
immediately reported to the clinical trial office. Alternative treat-
time. Pharmacokinetic drug interactions may result in changes
ment should be considered before re-exposure for those patients
of absorption, elimination, protein binding, or distribution of a
who developed seizures attributable to a certain CTD.
drug. Drug metabolism accounts for most clinically relevant
pharmacokinetic drug interactions between AEDs and CTDs, par-
However, the recurrence risk may be significantly higher in chil-
ticularly those involving cytochrome P450 (CYP) isoenzymes in
dren with fixed neurological abnormalities and certain cerebral
hepatic metabolism. Many of the drugs in use in paediatric on-
defects [45]. In adults with brain tumours it appeared that the
cology are metabolised by the CYP isoenzyme system and thus
earlier seizures occurred in the course of illness, the more likely
interactions mainly derive from inhibition or induction of these
they are to recur [69]. Brain imaging might sometimes offer im-
isoenzymes. The main isoenzymes in AED metabolism are
portant information contributing to the treatment decision.
CYP3A4, CYP2C9, and CYP2C19. For CTD metabolism, CYP3A4 isthe most important. In addition, UDP-glucoronosyltransferase
If initiation of AED treatment is indicated, the choice of AED in
(UGT) enzymes can also play a role. The potential of enzyme in-
paediatric oncology is based on the classification of seizures,
duction and inhibition varies widely among AED (see Table 5).
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
cutive children treated for acute lymphoblastic leukaemia re-ceived treatment for 30 days or longer with enzyme-inducing
Enzyme-inducing or inhibiting characteristics of different
anticonvulsants (PHT, PBT, CBZ, or a combination) at the same
time as antileukaemic therapy. In this study anticonvulsant ther-
apy was significantly related to worse event-free survival with
occurrence of more haematological, and CNS relapses among
the 566 patients with B-lineage leukaemia. A faster clearance of
teniposide and methotrexate was found among patients receiv-
A very recent retrospective study by Oberndorfer et al. [51] eval-
uated the effects of coadministration of AED on survival rates of
patients with glioblastoma multiforme, who underwent surgery,
radiotherapy and chemotherapy. A significant decline of survival
rates in the group of patients who received enzyme-inducing
Another clinically important example refers to data provided
from Hassan et al. [29] who were first to systematically study
the influence of PHT as preventative AED on BUS pharmacoki-
netics and pharamcodynamics in patients during conditioning
prior to bone marrow transplantation using BUS. They reported
a significantly faster clearance, a lower area under the concen-
According to the systematic approach by Vecht et al. [74] the most
tration-time curve and a shorter half-life if the BUS regime was
relevant clinical consequences of drug interactions or altered
pharmacodynamics, respectively, can be summarized as follows:
a) reduced efficacy of antiepileptic drugs, b) reduced efficacy of
CTD, c) increased toxicity of AED, d) increased toxicity of CTD.
Very little data are available on this possible effect of interaction.
Fluorouracil, an inhibitor of the CPY2C9 isoezyme, has been re-
Although only very few clinical studies have focussed on these
ported to induce toxic plasma concentrations of PHT leading to
special issues, case reports provide alarming evidence that this
severe neurological deficits mainly attributed to cerebellar dis-
is by no means only a theoretical matter, but has strong impact
turbances (Brickel et al. 2003). It can be speculated that in-
on clinical routine and decision making. This is illustrated by
creased toxicity of AEDs under certain enzyme-inhibiting CTDs
some exemplary data provided by current literature.
is underrepresented in current literature.
A number of case-reports of adult patients demonstrated a
VPA is a potent inhibitor of the CYP isoenzymes, mainly of CYP2C9.
marked drop of phenytoin (PHT) concentrations of up to 50 %
As VPA has very recently been studied as an adjunctive therapy for
after CTD administration. This was mainly attributed to cisplatin
acute myeloid leukaemia and myelodysplastic syndrome [10], in-
[22]. In a retrospective study by Grossmann et al. [26] all pa-
teractions with certain CTDs might become more relevant in fu-
tients who received three or more cycles of cisplatin and car-
ture. In a follow-up study of 70 adults with high-grade gliomas
mustine chemotherapy for primary brain tumours required an
an association of VPA with a fotemustine-cisplatin regimen re-
average increase in their maintenance PHT dose of 41 % to
sulted in a three-fold higher incidence of reversible thrombopenia,
neutropenia or both. Haematological side-effects decreased after
AED modification during the continued chemotherapy [7].
Valproic acid (VPA) has also been reported to be influenced by
cisplatin. In a patient receiving daily VPA, severe seizures were
Increased toxicity of IFO has been reported in a paediatric patient
observed 7 weeks after the first cisplatin-based chemotherapy
who received PBT as comedication. He developed IFO-encephalo-
cycle, when the serum VPA concentration was found to be re-
pathy, which was attributed to the enzyme inducing activity of
duced by approximately 50 % of the initial level [32]. Another
PBT leading to a higher amount of toxic IFO-metabolites [23].
case report described the recurrence of tonic-clonic seizure in a
child with acute lymphoblastic leukaemia under VPA therapy a
few hours after high-dose MTX. An acute decline of the serum
Interactions between corticosteroids and PHT and/or PBT may be
VPA concentration to about 25 % of the pre-MTX value could be
almost unpredictable. A variety of effects have been observed.
PHT and PBT have the potential to shorten the half-life and in-
crease total body clearance of dexamethasone and prednisone
[11]. On the other hand, both increased and lowered levels of
The potential of drug interactions to significantly worsen the
PHT were seen under comedication with dexamethasone. Lack-
outcome of malignant diseases under CTD was impressively illu-
ner [40] reported a patient receiving dexamethasone who re-
strated by a study of Relling et al. [59]. Forty of 716 (5.6 %) conse-
quired a daily PHT dose of greater than 10 mg/kg to maintain
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
therapeutic serum concentration. The concentration increased
AED related haematological side effects are particularly un-
by nearly 300 % after dexamethasone was discontinued. Con-
wanted in paediatric oncology. Although the overall incidence
trary, Lawson et al. [42] reported increased levels of PHT in pa-
in non-oncological patients seems to be low [6], it has been re-
tients receiving PHT and dexamethasone. This may be attributed
ported that, when AEDs are used in combination with antineo-
to competition on protein binding leading to intoxications,
plastic agents, these effects can be pronounced [7]. Aplastic
which also might mimic tumour progression. It has been hy-
anaemia (CBZ, PBT, PHT, ETX) and thrombopenia (VPA) are most
pothesized that decreased levels may be caused by induction of
hepatic metabolism causing a loss of seizure control [61]. How-
ever, the real pathophysiology of these contradictory effects is
Serious rashes, including Stevens-Johnson syndrome and anti-
convulsant hypersensitivity syndrome are rare, but potentially
fatal adverse effects that can occur and are more common when
Summarizing these results it can be stated that drug interactions
certain AEDs (PHT, PBT, CBZ) are used in combination with irra-
between AEDs and CTDs can have substantial effects on clinical
outcome. We therefore propose that therapeutic drug monitor-
ing may contribute to improving cancer chemotherapy and
One of the most severe long-term sequelae of childhood cancer
should therefore be further investigated particularly in view of
treatment may be neurocognitive disorders [4]. In this context
a variety of possible drug interactions between AEDs and CTDs.
CNS side-effects of AEDs are particularly worrying. No AED ap-
pears to be completely exempt from unfavourable cognitive
and/or behavioural effects [2]. Previous clinical studies indicate
Adverse effects of AED relevant in paediatric oncology
that older AEDs have the most negative cognitive profile, mainly
PB and PHT [18, 49]. However, even the “new” AEDs, e. g., topira-
Newer and more aggressive treatments of malignancies in child-
mate or levetiracetam, have been associated with adverse cogni-
hood have lead to significantly longer survival rates of affected
tive or neurobehavioral effects. Lamotrigine seems to have a fa-
children. Therefore, adverse effects of long-term anticonvulsive
vourable cognitive profile [1, 46, 67].
treatment have to be considered. It is beyond the scope of thisreview to cover all these aspects of AED treatment in detail. A
Appetite regulation can be a relevant clinical problem in oncol-
summary of the most relevant side effects of frequently used
ogy in both terms, uncontrolled eating, mainly in cerebral malig-
AED in paediatrics is given in Table 6. Some aspects are of special
nancies or anorexia, either due to CTDs or the malignancy itself.
These effects may be worsen by certain AED (see Table 6).
Commonly prescribed AED in childhood, dosage, side-effects [2, 5, 13, 27]
rash, aplastic anaemia (rare), ataxia,diplopia
cardiac arrythmia, purple glove syn-drome
nephrolithiasis, glaucoma, hypohydro-sis, metabolic acidosis
thrombopenia, hepatic failure, hyper-ammonemia, pancreatic failure, tre-mor
* add-on enzyme-inducers: 5–15 mg/kg; add-on VPA: 1–3 mg/kg
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
Effects of long-term AED treatment on hormonal function, con-
CTDs and AEDs is essential. If possible, therapy should rapidly
traception, sexuality, and pregnancy is an important issue for
be changed to non-enzyme inducing or inhibiting AED once the
adolescents [33]. Early counselling on effective contraception is
patient’s status has stabilized. It needs to be stressed that this
essential in female teenagers with cancer in order to prevent un-
may again lead to significant alterations of CTD levels.
wanted pregnancies particularly in view of potentially terato-
genic and mutagenic drugs during cancer treatment [41]. The in-
Patients with progressive tumours or severe mucositis might lose
fluence of AED selection on current or future choices of contra-
the ability to swallow even suspensions. Beside i. v.- and i. m.-
ceptive methods needs to be considered when choosing an AED
preparations (e. g. PB; [34]), buccal application might be consid-
for those patients who are likely to continue treatment into their
ered on this occasion. This is an option for lorazepam and mida-
childbearing years. Nonenzyme-inducing AEDs do not show any
zolam. Sedative side-effects of these AED may even be desirable.
interactions with the oral contraceptive pill and should therefore
In addition, lorazepam has antiemetic and anxiolytic properties.
be preferred in these patients [14, 78]. Reduced fertility in wom-
en with epilepsy and foetal damages due to AEDs used during
As mentioned above, epilepsy treatment in female teenagers
pregnancy are additional concerns [71].
pose a number of additional difficulties. Treatment decisions
should follow currently existing guidelines for the management
Different regimens have been suggested as preventative AED
The primary concern of AED treatment is maintaining adequate
treatment in patients undergoing high-dose busulfan therapy
seizure control. Although exact epidemiological data are missing
(see Table 7). PHT should no longer be used for its potential for
it can be presumed that the majority of seizures in paediatric on-
drug interaction and a unfavourable profile of adverse effects [29].
cology will be partial or secondary generalized. A variety of older
and newer AED have been shown good effectiveness in children
Last but not least it is noteworthy to mention that especially in
with focal epilepsy [27]. However, the use of enzyme-inducing
brain tumour patients seizures may be refractory to medical man-
AED as drugs of first choice is still wide routine in paediatric on-
agement and epilepsy surgery can sometimes be performed [69].
cology departments, mainly PHT, PBT, and CBZ. VPA has also
been recommended [30]. However, having in mind the above de-
scribed potentially fatal effects of drug interactions between
Seizure prophylaxis in children with brain tumours
AED and CTD it seems reasonable to propose that AEDs not in-
ducing or inhibiting the cytochrome P450 system should be pre-
Because a substantial number of patients with brain tumours may
ferred. As rapid titration is often required, gabapentin or levetir-
develop seizures, it remains common practice among neurooncol-
acetam have been suggested as possible candidates with good
ogists and neurosurgeons to initiate preventive AED treatment
efficacy and a favourable safety profile [34, 36, 74]. Gabapentin
even in the absence of seizures. Many patients who have experi-
has been proven effective in partial seizures [19]. There is some
enced a single seizure attributable to brain tumours will be put
experience that gabapentin is well tolerated and provide effec-
on regular AED and often keep on taking their anticonvulsive
tive seizure control in children under CTD [36]. Levetiracetam is
medication for years. The rational for this policy has been ad-
considered as a wide-spectrum AED effective in both partial and
dressed in several studies, but continues to be controversial [68].
generalized seizures [19, 63]. In adults with end stage brain tu-
However, growing evidence clearly points against the usefulness
mours levetiracetam has been reported as a good option due to
of preventive AED treatment. A practice parameter established by
its efficacy and tolerability [34]. In children with treatment-re-
the American Academy of Neurology [24] recommended that pro-
sistant partial seizures it was effective and well tolerated as ad-
phylactic anticonvulsants should not be used routinely in patients
with newly diagnosed brain tumours. Perioperative prophylaxis
should be tapered off after the first postoperative week. In support
However, it has to be stressed that recommendations of long-
of this view, two recent meta-analyses found no evidence to sup-
term AED treatment in the oncology patient are not supported
port AED prophylaxis with PBT, PHT, or valproic acid in patients
by robust empirical evidence. In addition, due to the complexity
with brain tumours and no history of seizures, regardless of neo-
of patients under cancer treatment an individualized approach
plastic type [68, 70]. However, currently available data need to be
to any such child with epilepsy is required. According to the spe-
interpreted with some caution. None of the studies included in
cific patients needs different AED treatment regimes may be in-dicated, including enzyme-inducing AED or combination ther-
apy. Therefore, the right choice of treatment requires consider-
Busulfan and options of preventive AED treatment
able expertise in the care of paediatric epilepsy patients.
If only short-term use is expected, clonazepan may be a candidate
with an excellent broad-spectrum efficacy. Its use is sometimes
limited by sedating effects, hypersalivation, ataxia, and most im-
portantly, the development of tolerance, usually after 3–6 months.
Short-term use of PHT, PB or VPA may be justified if i.v.-applica-
tion is necessary. However, closed monitoring of drug levels of
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
meta-analyses were performed using newer AED. Moreover, there
5 Biton V. Effect of antiepileptic drugs on bodyweight: overview and
is a lack of reliable risk-factors predictive for seizure occurrence
clinical implications for the treatment of epilepsy. CNS Drugs 2003;17: 781 – 791
6 Blackburn SC, Oliart AD, Garcia Rodriguez LA, Perez Gutthann S. Anti-
epileptics and blood dyscrasias: a cohort study. Pharmacotherapy
In addition, it needs to be stressed, that once a patient experi-
ences a seizure clearly attributable to a brain tumor, long-term
Bourg V, Lebrun C, Chichmanian RM, Thomas P, Frenay M. Nitroso-urea-cisplatin-based chemotherapy associated with valproate: in-
treatment with AED is generally accepted as proper medical
crease of haematologic toxicity. Ann Oncol 2001; 12: 217 – 219
care due to the high risk of recurrence [69].
8 Brickell K, Porter D, Thompson P. Phenytoin toxicity due to fluoropyr-
imidines (5FU/capecitabine): three case reports. Br J Cancer 2003; 89:615 – 616
9 Brodie MJ, French JA. Management of epilepsy in adolescents and
10 Bug G, Ritter M, Wassmann B, Schoch C et al. Clinical trial of valproic
Antiepileptic treatment in paediatric oncology poses numerous
acid and all-trans retinoic acid in patients with poor-risk acute mye-
diagnostic and therapeutic challenges. This requires a close in-
loid leukemia. Cancer 2005; 104: 2717 – 2725
11 Chalk JB, Ridgeway K, Brophy T, Yelland JD, Eadie MJ. Phenytoin im-
terdisciplinary approach to the seizing child or adolescent. A
pairs the bioavailability of dexamethasone in neurological and neuro-
prompt and detailed diagnostic work-up is needed in every sin-
surgical patients. J Neurol Neurosurg Psychiatry 1984; 47: 1087 – 1090
gle case in order to establish the diagnosis and, equally impor-
12 Chan KW, Mullen CA, Worth LL, Choroszy M, Koontz S, Tran H, Slopis J.
tant, to detect any treatable underlying pathology.
Lorazepam for seizure prophylaxis during high-dose busulfan admin-istration. Bone Marrow Transplant 2002; 29: 963 – 965
13 Crawford P. Interactions between antiepileptic drugs and hormonal
If clinical events are not clearly defined as seizures the best way
contraception. CNS Drugs 2002; 16: 263 – 272
to prevent adverse effects of AEDs is to consider not to give AED
14 Crawford P. Best practice guidelines for the management of women
at all. Preventive AED treatment in patients with primary brain
with epilepsy. Epilepsia 2005; 46 (Suppl 9): 117 – 124
15 Creutzig U, Hannemann J, Kramer I, Zimmermann M, Herold R, Marx
JF. The “quality house pediatric oncology” as an instrument for im-proving the performance of the trial centers. Klin Padiatr 2005; 217:
If AED treatment is initiated possible drug interactions and side
effects relevant in paediatric oncology have to be taken into ac-
De La Camara R, Tomas JF, Figuera A, Berberana M, Fernandez-RanadaJM. High dose busulfan and seizures. Bone Marrow Transplant 1991;
count. Enzyme inducing and inhibiting AEDs should be avoided
unless alternative treatment with non-inducing AEDs is not fea-
17 DiMario FJ, Packer RJ. Acute mental status changes in children with
sible. Regular review of the continuing need for AED treatment is
systemic cancer. Pediatrics 1990; 85: 353 – 360
Farwell JR, Lee YJ, Hirtz DG et al. Phenobarbital for febrile seizures –effects on in telligence and on seizure recurrence. N Engl J Med 1990;322: 364 – 369
Regarding the new non-enzyme inducing or inhibiting AEDs,
19 French JA, Kanner AM, Bautista J, Abou-Khalil B, Browne T, Harden CL,
preliminary studies indicate that gabapentin and levetiracetam
Theodore WH, Bazil C, Stern J, Schachter SC, Bergen D, Hirtz D, Mon-
may provide a favourable profile in terms of efficacy and safety.
touris GD, Nespeca M, Gidal B, Marks Jr WJ, Turk WR, Fischer JH, Bour-geois B, Wilner A, Faught Jr RE, Sachdeo RC, Beydoun A, Glauser TA. Efficacy and tolerability of the new antiepileptic drugs I: treatment of
However, more properly designed clinical studies are warranted
new onset epilepsy: report of the Therapeutics and Technology As-
to raise the level of evidence for robust clinical recommenda-
sessment Subcommittee and Quality Standards Subcommittee of the
tions. These studies should also investigate the influence of AED
American Academy of Neurology and the American Epilepsy Society. Neurology 2004; 62: 1252 – 1260
treatment on overall outcome measures. We believe that compe-
20 Gieron MA, Barak LS, Estrada J. Severe encephalopathy associated
tence networks will be helpful to structure clinical trials and
with ifosfamide administration in two children with metastatic tu-
standardize future therapy regimes [15]. Clinicians will need to
continue to question current policies and adapt their daily prac-
Gilliam FG, Fessler AJ, Baker G, Vahle V, Carter J, Attarian H. Systematicscreening allows reduction of adverse antiepileptic drug effects. Neu-
22 Ghosh C, Lazarus HM, Hewlett JS, Creger RJ. Fluctuation of serum PHT
concentrations during autologous bone marrow transplant for pri-
mary central nervous system tumors. J Neurooncol 1992; 12: 25 – 32
23 Ghosn M, Carde P, Leclerq B, Flamant F, Friedman S, Droz JP, Hayat M.
Ifosfamide/mesna related encephalopathy: a case report with a possi-
The authors have no conflict of interest to disclose.
ble role of phenobarbital in enhancing neurotoxicity. Bull Cancer1988; 75: 391 – 392
24 Glantz MJ, Cole BF, Forsyth PA, Recht LD, Wen PY, Chamberlain MC,
Grossman SA, Cairncross JG. Practice parameter: anticonvulsant pro-phylaxis in patients with newly diagnosed brain tumors: report of
the Quality Standards Subcommittee of the American Academy ofNeurology. Neurology 2000; 54: 1886 – 1893
1 Aldenkamp AP, De Krom M, Reijs R. Newer antiepileptic drugs and
25 Glauser TA, Ayala R, Elterman RD, Mitchell WG, Van Orman CB, Gauer
cognitive issues. Epilepsia 2003; 44 (Suppl 4): 21 – 29
LJ, Lu Z. Double-blind placebo-controlled trial of adjunctive levetira-
2 Arzimanoglou A, Guerrini R, Aicardi J. Aicardi’s Epilepsy in Children.
cetam in pediatric partial seizures. Neurology 2006; 66: 1654 – 1660
3rd edn. Lippincott Williams & Wilkins, Philadelphia 2004; 369
26 Grossman SA, Sheidler VR, Gilbert MR. Decreased phenytoin levels in
3 Beaumont A, Whittle IR. The pathogenesis of tumor associated epi-
patients receiving chemotherapy. Am J Med 1989; 87: 505 – 510
lepsy. Acta Neurochir 2000; 142: 1 – 15
27 Guerrini R. Epilepsy in children. Lancet 2006; 367: 499 – 524
4 Bhatia S. Cancer survivorship – pediatric issues. Hematology (Am Soc
28 Hartmann O. Ifosfamide induced encephalopathy: 15 observations.
Hematol Educ Program) 2005; 1: 507 – 515
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
29 Hassan M, Oberg G, Bjorkholm M, Wallin I, Lindgren M. Influence of
54 Pelgrims J, De Vos F, Van den Brande J, Schrijvers D, Prove A, Vermor-
prophylactic anticonvulsant therapy on high-dose busulphan ki-
ken JB. Methylene blue in the treatment and prevention of ifosfamide-
netics. Cancer Chemother Pharmacol 1993; 33: 181 – 186
induced encephalopathy: report of 12 cases and a review of the litera-
30 Hildebrand J. Management of epileptic seizures. Curr Opin Oncol
55 Plotkin SR, Wen PY. Neurologic complications of cancer therapy. Neu-
31 Hindley D, Ali A, Robson C. Diagnoses made in a secondary care “fits,
faints, and funny turns” clinic. Arch Dis Child 2006; 91: 214 – 218
56 Primavera A, Audenino D, Cocito L. Ifosfamide encephalopathy and
32 Ikeda H, Murakami T, Takano M, Usui T, Kihira K. Pharmacokinetic in-
nonconvulsive status epilepticus. Can J Neurol Sci 2002; 29: 180 – 183
teraction on valproic acid and recurrence of epileptic seizures during
57 Quinn CT, Griener JC, Bottiglieri T, Hyland K, Farrow A, Kamen BA. Ele-
chemotherapy in an epileptic patient. Br J Clin Pharmacol 2005; 59:
vation of homocysteine and excitatory amino acid neurotransmitters
in the CSF of children who receive methotrexate for treatment of can-
33 Isojarvi JI. Reproductive dysfunction in women with epilepsy. Neurol-
cer. J Clin Oncol 1997; 15: 2800 – 2806
58 Quinn CT, Griener JC, Bottiglieri T, Hyland K, Farrow A, Kamen BA.
34 Junck L. Supportive management in neuro-oncology: opportunities
Methotrexate, homocysteine and seizures. J Clin Oncol 1998; 16:
for patient care, teaching, and research. Curr Opin Neurol 2004; 17:
59 Relling MV, Pui CH, Sandlund JT, Rivera GK, Hancock ML, Boyett JM,
35 Keime-Guibert F, Napolitano M, Delattre JY. Neurological complica-
Schuetz EG, Evans WE. Adverse effect of anticonvulsants on efficacy
tions of radiotherapy and chemotherapy. J Neurol 1998; 245: 695 –
of chemotherapy for acute lymphoblastic leukaemia. Lancet 2000;
36 Khan RB, Hunt DL, Boop FA, Sanford RA, Merchant TE, Gajjar A, Kun LE.
60 Rosenow F, Hamer HM, Knake S, Katsarou N, Fritsch B, Oertel WH,
Seizures in children with primary brain tumors: incidence and long-
Shiratori K, Luders HO. Lateralizing and localizing signs and symp-
term outcome. Epilepsy Res 2005; 64: 85 – 91
toms of epileptic seizures: significance and application in clinical
37 Khan RB, Onar A. Seizure Recurrence and Risk Factors after Antiepi-
practice. Nervenarzt 2001; 72: 743 – 749
lepsy Drug Withdrawal in Children with Brain Tumors. Epilepsia
61 Rüegg S. Dexamethasone/phenytoin interactions: neurooncological
concerns. Swiss Med Wkly 2002; 132: 425 – 426
38 Kieslich M, Porto L, Lanfermann H, Jacobi G, Schwabe D, Bohles HJ.
62 Ruffmann C, Bogliun G, Beghi E. Epileptogenic drugs: a systematic re-
Cerebrovascular complications of L-asparaginase in the therapy of
view. Expert Rev Neurother 2006; 6: 575 – 589
acute lymphoblastic leukemia. Pediatr Hematol Oncol 2003; 25:
63 Sankar R. Initial treatment of epilepsy with antiepileptic drugs: pedia-
tric issues. Neurology 2004; 63 (Suppl 4): S30 – S39
39 Kilickap S, Cakar M, Onal IK, Tufan A, Akoglu H, Aksoy S, Erman M, Te-
64 Schroder H, Ostergaard JR. Interference of high-dose methotrexate in
kuzman G. Nonconvulsive Status Epilepticus Due to Ifosfamide. Ann
the metabolism of valproate? Pediatr Hematol Oncol 1994; 11: 445 –
40 Lackner TE. Interaction of dexamethasone with phenytoin. Pharma-
65 Schwarer AP, Opat SS, Watson AL, Cole-Sinclair MF. Clobazam for sei-
zure prophylaxis during busulfan chemotherapy. Lancet 1995; 346:
41 Laurence V, Gbolade BA, Morgan SJ, Glaser A. Contraception for teen-
agers and young adults with cancer. Eur J Cancer 2002; 40: 2705 –
66 Serkova NJ, Christians U, Benet LZ. Biochemical mechanisms of cyclos-
porine neurotoxicity. Mol Interv 2004; 4: 97 – 107
42 Lawson LA, Blouin RA, Smith RB, Rapp RP, Young AB. Phenytoin-dexa-
67 Siemes H, Brandl U, Helmstadter C, Kurlemann G, Rating D, Salke-Kel-
methasone interaction: a previously unreported observation. Surg
lermann RA, Stephani U, Uberall M, Wiemer-Kruel A, Bergmann L. Op-
timizing epilepsy therapy in children and adolescents with lamotri-
43 Langebrake C, Uhlenbrock S, Ritter J, Groll AH. Drug interactions of
gine. Klin Padiatr 2005; 217: 222 – 229
antimicrobial agents in children with cancer. Klin Padiatr 2005; 217
68 Sirven JL, Wingerchuk DM, Drazkowski JF, Lyons MK, Zimmerman RS.
Seizure Prophylaxis in Patients With Brain Tumors: A Meta-analysis.
44 Loring DW, Meador KJ. Cognitive side effects of antiepileptic drugs in
children. Neurology 2004; 62: 872 – 877
69 Sperling MR, Ko J. Seizures and brain tumors. Semin Oncol 2006; 33:
45 Maytal J, Grossman R, Yusuf FH, Shende AC, Karayalycin G, Lanzkows-
ky P, Schaul N, Eviatar L. Prognosis and treatment of seizures in chil-
70 Stevens GH. Antiepileptic therapy in patients with central nervous
dren with acute lymphoblastic leukemia. Epilepsia 1995; 36: 831 –
system malignancies. Curr Neurol Neurosci Rep 2006; 6: 311 – 318
71 Tomson T, Perucca E, Battino D. Navigating toward fetal and maternal
46 Meador KJ, Loring DW, Vahle VJ, Ray PG, Werz MA, Fessler AJ, Ogrocki
health: the challenge of treating epilepsy in pregnancy. Epilepsia
P, Schoenberg MR, Miller JM, Kustra RP. Cognitive and behavioral ef-
fects of lamotrigine and topiramate in healthy volunteers. Neurology
72 Uldall P, Alving J, Hansen LK, Kibaek M, Buchholt J. The misdiagnosis of
epilepsy in children admitted to a tertiary epilepsy centre with parox-
47 Micali G, Linthicum K, Han N, West DP. Increased risk of erythema
ysmal events. Arch Dis Child 2006; 91: 219 – 221
multiforme major with combination anticonvulsant and radiation
73 Vassal G, Deroussent A, Hartmann O, Challine D, Benhamou E, Val-
therapies. Pharmacotherapy 1999; 19: 223 – 227
teau-Couanet D, Brugieres L, Kalifa C, Gouyette A, Lemerle J. Dose-de-
48 Mockenhaupt M, Messenheimer J, Tennis P, Schlingmann J. Risk of Ste-
pendent neurotoxicity of high-dose busulfan in children: a clinical
vens-Johnson syndrome and toxic epidermal necrolysis in new users
and pharmacological study. Cancer Res 1990; 50: 6203 – 6207
of antiepileptics. Neurology 2005; 64: 1134 – 1138
74 Vecht CJ, Wagner GL, Wilms EB. Interactions between antiepileptic
49 Ney GC, Lantos G, Barr WB, Schaul N. Cerebellar atrophy in patients
and chemotherapeutic drugs. Lancet Neurol 2003; 2: 404 – 409
with long term PHT exposure and epilepsy. Arch Neurol 1994; 51:
75 Verstappen CC, Heimans JJ, Hoekman K, Postma TJ. Neurotoxic com-
plications of chemotherapy in patients with cancer: clinical signs and
50 Nicolao P, Giometto B. Neurological toxicity of ifosfamide. Oncology
optimal management. Drugs 2003; 63: 1549 – 1563
76 Winick NJ, Bowman WP, Kamen BA, Roach ES, Rollins N, Jacaruso D,
51 Oberndorfer S, Piribauer M, Marosi C, Lahrmann H, Hitzenberger P,
Buchanan GR. Unexpected acute neurologic toxicity in the treatment
Grisold W. P450 enzyme inducing and non-enzyme inducing antiepi-
of children with acute lymphoblastic leukemia. J Natl Cancer Inst
leptics in glioblastoma patients treated with standard chemotherapy.
77 Wong DD, Longenecker RG, Liepman M, Baker S, LaVergne M. Pheny-
52 Ochs JJ, Bowman WP, Pui C-H et al. Seizures in childhood lymphoblas-
toin-dexamethasone: a possible drug-drug interaction. JAMA 1985;
tic leukemia patients. Lancet 1984; 2: 1422 – 1424
53 Orbach D, Brisse H, Doz F. Central neurological manifestations during
78 Zupanc ML. Antiepileptic drugs and hormonal contraceptives in ado-
chemotherapy in children. Arch Pediatr 2003; 10: 533 – 539
lescent women with epilepsy. Neurology 2006; 66 (Suppl 3): S37 –S45
Tibussek D et al. Antiepileptic Treatment in … Klin Pädiatr 2006; 218: 340 – 349
Sleep Your Way to Better Health Want to lose weight, boost your immune system, improve your energy and performance at work and look years younger ? The answer could be as simple as getting a good night’s sleep. North Americans are sleeping less than ever before and the effect on our health care system is substantial. As a societ
 Example of seizure incidence in paediatric brain tumours
In general, acute neurological symptoms under certain CTDs are
not uncommon [35, 55, 75]. The toxicity of CTDs to the central ner-
vous system is directly related to their ability to cross the BBB.
Example of seizure incidence in paediatric brain tumours
In general, acute neurological symptoms under certain CTDs are
not uncommon [35, 55, 75]. The toxicity of CTDs to the central ner-
vous system is directly related to their ability to cross the BBB.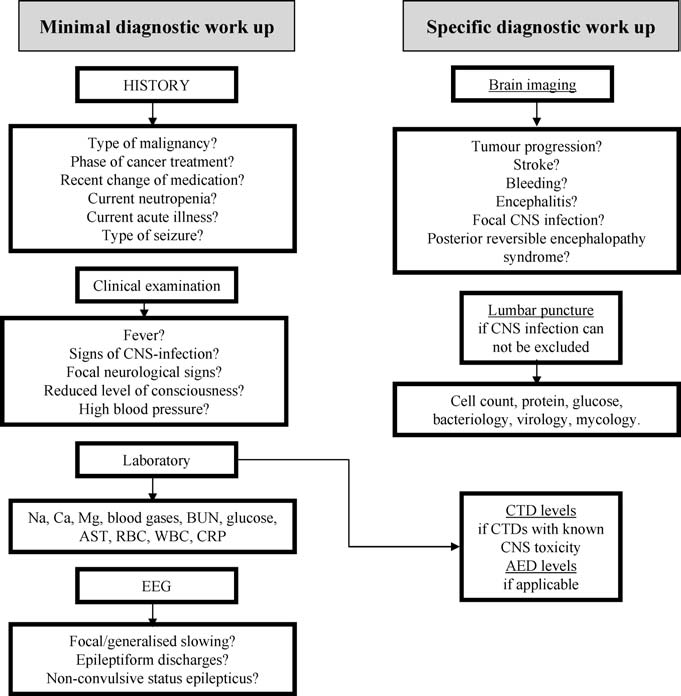 of AEDs and their possible toxic effects [21]. Predicting the risk of
age and sex of the patient, comorbidities, and comedications.
of AEDs and their possible toxic effects [21]. Predicting the risk of
age and sex of the patient, comorbidities, and comedications.