Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Randomized, placebo-controlled, double-blind clinical trial evaluating the treatment of plantar fasciitis with an extracoporeal shockwave therapy (eswt) device: a north american confirmatory study
Randomized, Placebo-Controlled, Double-Blind ClinicalTrial Evaluating the Treatment of Plantar Fasciitis with anExtracorporeal Shockwave Therapy (ESWT) Device:A North American Confirmatory Study
Patricia Kudo,1 Katie Dainty,1 Michael Clarfield,2 Larry Coughlin,3 Pauline Lavoie,4 Constance Lebrun1
1Fowler Kennedy Sport Medicine Clinic, 3M Centre University of Western Ontario, London, Ontario N6A 3K7, Canada
2The Sports Medicine Specialists, 150 Eglinton Avenue East, Toronto, Ontario M4P 1E8, Canada
3West Island Orthopedic & Sports Medicine Center, 3881 Boulevard St-Jean Dollard-des-Ormeaux,Quebec H9G 2V1, Canada
4Action Sport Physio, 1451 rue Montarville, St-Bruno, Quebec J3V 3T6, Canada
Received 2 December 2004; accepted 16 May 2005
Published online 18 November 2005 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jor.20008
ABSTRACT: Despite numerous publications and clinical trials, the results of treatment ofrecalcitrant chronic plantar fasciitis with extracorporeal shockwave therapy (ESWT) still remainequivocal as to whether or not this treatment provides relief from the pain associated with thiscondition. The objective of this study was to determine whether extracorporeal shock wave therapycan safely and effectively relieve the pain associated with chronic plantar fasciitis compared toplacebo treatment, as demonstrated by pain with walking in the morning. This was set in amulticenter, randomized, placebo-controlled, double-blind, confirmatory clinical study undertakenin four outpatient orthopedic clinics. The patients, 114 adult subjects with chronic plantar fasciitis,recalcitrant to conservative therapies for at least 6 months, were randomized to two groups. Treatment consisted of approximately 3,800 total shock waves (Æ10) reaching an approximated totalenergy delivery of 1,300 mJ/mm2 (EDþ) in a single session versus placebo treatment. This studydemonstrated a statistically significant difference between treatment groups in the change frombaseline to 3 months in the primary efficacy outcome of pain during the first few minutes of walkingmeasured by a visual analog scale. There was also a statistically significant difference betweentreatments in the number of participants whose changes in Visual Analog Scale scores met the studydefinition of success at both 6 weeks and 3 months posttreatment; and between treatment groups inthe change from baseline to 3 months posttreatment in the Roles and Maudsley Score. The results ofthis study confirm that ESWT administered with the Dornier Epos Ultra is a safe and effectivetreatment for recalcitrant plantar fasciitis. ß 2005 Orthopaedic Research Society. Published byWiley Periodicals, Inc. J Orthop Res 24:115–123, 2006Keywords:
plantar fasciitis; shock wave therapy; heel pain; ESWT
tripsy (ESWL) has been well established for over20 years for the treatment of urologic conditions,1
In the past 20 years extracorporeal shock waves
and more recently, there has been significant
have been used to safely and effectively treat a
interest in orthopedic applications such as non-
number of medical conditions. Shock wave litho-
union fractures and several types of tendonopa-thies. Despite numerous publications and clinical
Correspondence to: Katie Dainty (Telephone: 416-480-6100,
trials, one orthopedic application of ESWT, which
still remains highly equivocal, is the treatment of
ß 2005 Orthopaedic Research Society. Published by Wiley Periodicals,Inc.
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
Plantar fasciitis is defined as a tensile overload
Two ESWT devices have now gained approval
of the plantar fascia at its origin on the medial
from the Food and Drug Administration for the
tubercle of the calcaneus.15 The plantar fascia is a
treatment of recalcitrant plantar fasciitis in
thick fibrous tissue on the bottom of the foot that
the United States; however, the evidence is still
protects sensitive plantar structures such as
divergent. The significant differences in the
nerves, vessels, muscles, and tendons, and in
results of the various studies may be explained
addition, is responsible for maintaining the plan-
by a number of factors including technical differ-
tar arch. The symptoms usually start as a dull
ences (machine design, shock intensity and fre-
intermittent pain that most often progresses to a
quency, and the use of different forms of placebo
sharp persistent pain. The patient typically suffers
treatment), as well as differences in subject
pain with the first steps in the morning or after
populations, severity of disease, and study design.
period of prolonged sitting. This pain is aggravated
This highlights the need for further investigation
by continuous weight bearing, and becomes pro-
using solid randomized prospective and confirma-
gressively more severe. Its onset is insidious, and
tory clinical trials. To further enhance the results
not always associated with a specific incident or
shown in the first study using the Dornier Epos
trauma. Standard care at present is conservative
Ultra, the present study was designed as a con-
treatment, but about 10% of patients fail to
firmatory evidence trial to assess the safety and
respond or heal spontaneously.3 This extremely
effectiveness of the Dornier Epos Ultra in the
painful condition has been reported to effect up to
treatment of pain associated with chronic plantar
20% of the general population over their lifetime,4
and is responsible for approximately 1 millionpatient visits per year in the United States.5
In a review of the current published literature
on the use of shockwave therapy for the treatmentof plantar fasciitis, several clinical trials were
This was a multicenter, randomized, placebo-con-trolled, prospective, double-blind, confirmatory clinical
found. Among a plethora of nonrandomized pub-
study with two groups: one group receiving ESWT with
lications, there are only six placebo-controlled
the Epos Ultra (Active group) and a Control group
trials.6–11 all of which have reported extremely
receiving placebo treatment. The objective of the study
variable results. A meta-analysis done by Ogden
was to determine whether ESWT could safely and
et al. in 200212 found that those published studies
effectively relieve the pain associated with chronic
that fulfilled the criteria for acceptable methodol-
plantar fasciitis compared to placebo treatment with a
ogy with sufficient duration did show that directed
single high-energy treatment, as demonstrated by relief
application of shockwaves to the origin of the
of pain with the first few minutes of walking in the
plantar fascia is a safe and effective nonsurgical
method for treating chronic, recalcitrant heel pain
The initial sample size calculation was based on the
syndrome.4 However, recent studies such as those
primary efficacy outcome, defined as the differencebetween the Active Epos treatment and the Placebo
by Buchbinder et al.,7 Haake et al.,8 and Speed
treatment measured by the change from baseline to
et al.10 have reported no statistically significant
3 months in the Visual Analog Scale (VAS) score for pain
differences in the degree of improvement between
while walking for the first few minutes in the morning
( p ¼ 0.05). The expected effect size of the primary
Of those trials that reported a positive outcome,
outcome was estimated from the treatment difference
shock wave therapy for the treatment of plantar
and standard deviation of 1.4 and 3.0, respectively,
fasciitis was shown to be most efficacious with
found in the original pivotal U.S. clinical study11 should
a single therapy session. A pivotal study approv-
be #13. The calculation was done using Statistical
ed by the Food and Drug Administration in
Solutions nQuery Advisor1 Release 3.0 software, and
2002, showed that the Dornier Epos Ultra shock-
was adjusted by 15% to account for attrition rates.
wave device could safely produce clinical improve-
Secondary efficacy outcomes included change scores forthe American Orthopedic Foot and Ankle Society
ment in chronic plantar fasciitis using a single
(AOFAS) ankle–hindfoot scale score16 (pain and range
therapeutic session.11 The Active treatment
of motion domains), the Roles and Maudsley Score2
group in this trial reported 56% success and the
(a four-point patient self-assessment of pain and limita-
control group reported 47% success at 3 months
tions of activity), the SF 12 Global Health Rating
posttreatment. Other publications from all over
Scale,14 and pain on palpation (point of tenderness) as
the world have shown success rates as high as
measured with a pressure threshold meter (PTM, Pain
Diagnostics and Thermography, Great Neck, NY). A
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
primary safety analysis was also done comparing the
tion. Absence of a calcaneal fracture, bony abnormality,
incidence of adverse events between groups at the time
or other pathology (i.e., tumors) was confirmed with a
of treatment, and during follow-up. All follow-up data
lateral radiograph prior to treatment.
was measured by independent research investigators ateach site, all of whom were blinded to the randomization
The randomization scheme was generated by BiostatInternational, Inc., Tampa, Florida. Sealed, opaque,
tamper-proof envelopes containing individual randomi-zation assignments were provided to each investiga-
The study was conducted at four centers throughout
tional site prior to the beginning of the study. Subjects
Canada. Each site obtained approval from an institu-
were randomized by the treating investigator just prior
tional ethics review board review board prior to begin-
to the beginning of treatment. The first subject was
ning the study. An Investigational Testing Authorization
randomized in November 2000, and the last subject was
from the Therapeutic Products Programme Division of
Health Canada was also granted. Subjects were recruit-ed through outpatient clinics at each of the study sites.
All coinvestigators were primary care, sport medicinephysicians or orthopedic specialists and were trained on
All procedures were performed in outpatient settings
treatment with the Dornier Epos Ultra extracorporeal
using a single treatment method with the Dornier
shockwave system prior to the study. All potential
Epos Ultra extracorporeal shockwave therapy system
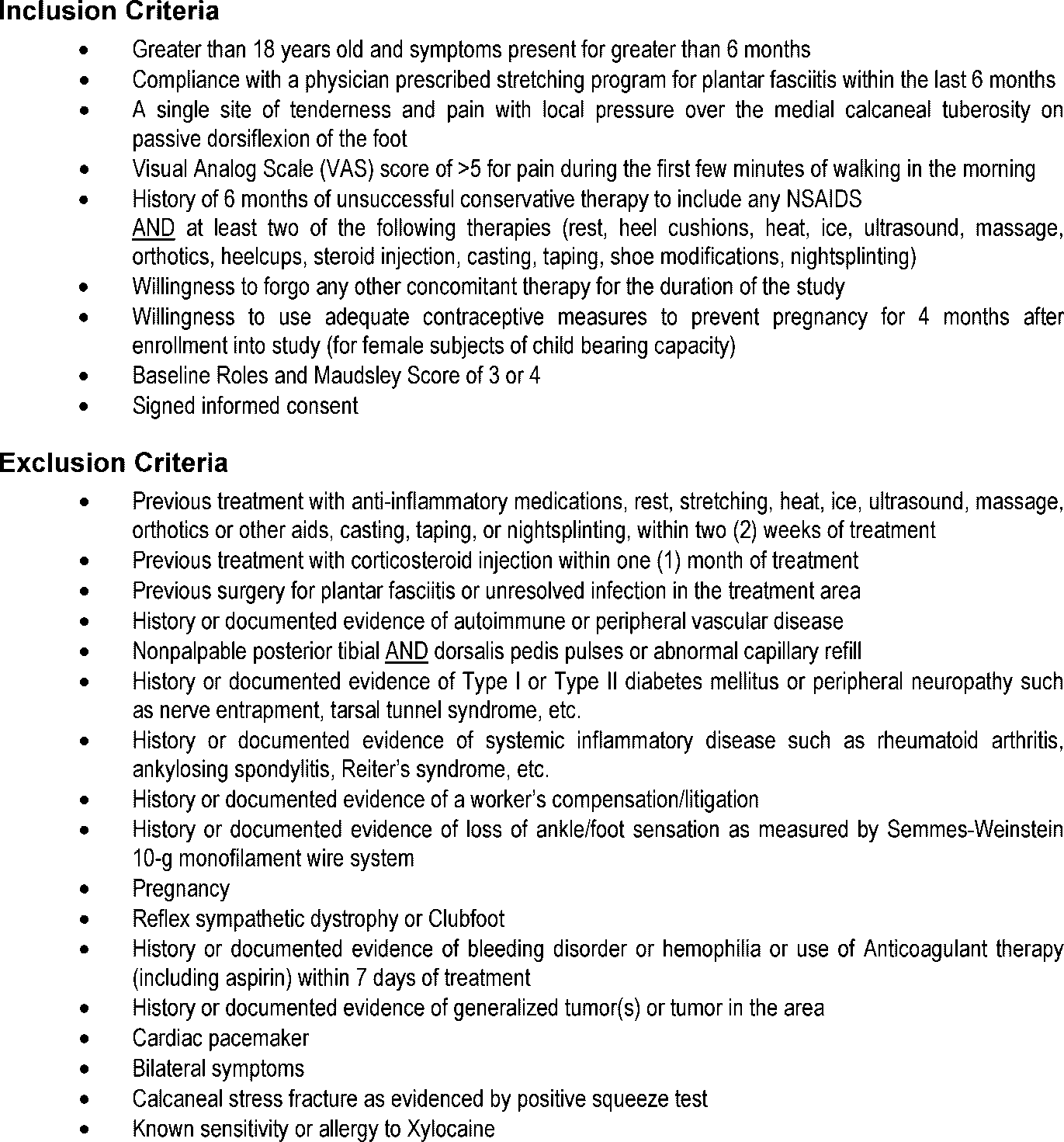
subjects were assessed according to the inclusion and
(Dornier MedTech Systems, GmbH, Germany). The
exclusion criteria (Fig. 1) in the study protocol and
subjects were placed either prone (44.7% of subjects) or
signed informed consent prior to their baseline evalua-
on their side (55.3% of subjects) on the examination table
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
with the study foot placed in a supported position. Choice
3 months posttreatment. Unblinding occurred at the
of position was based on patient comfort. Prior to shock
3-month visit. Subjects who received Active treatment
wave exposure, the area of pain was marked with an X
continued in the study and were evaluated at 6 and
on the skin to assist in focusing the delivery of the shock
12 months posttreatment. Subjects who originally
waves, and all study subjects, including the Placebo
received placebo treatment and whose symptoms were
group, were given a medial calcaneal nerve block using
still significant according to specified inclusion criteria
5 mL of 1% Xylocaine, 15–20 min prior to the procedure.
were offered to ‘‘crossover,’’ and receive Active treat-
The therapy head was coupled tangentially on the
ment with the Epos Ultra after their 3 month follow-up
medial aspect of the foot, and ultrasound localization
visit. Subjects originally randomized to the Placebo
was used for positioning of the focal area.
group who elected not to cross over at 3 months were
The Active treatment session was performed using
discontinued from study follow-up. All subjects were
the energy levels indicated in Table 1. The energy
given a pain medication diary with instructions during
parameter was 0.36 mJ/mm2 (EDþ), which is equivalent
screening and at each follow-up visit. Entries were
to 0.64 mJ/mm2 (ED). Shock wave frequency began at 60
made by the subject for any alternative medication
shocks/min, and was increased in increments of 30
taken between follow-up visits (i.e., Tylenol for a
shocks/min. During treatment, the frequency of release
headache). All subjects underwent a physical examina-
of the shock waves began at 60 shocks/min at level 1, and
tion including a pressure threshold measurement and
was increased by one level of 30 shocks/min at each
were asked to assess their pain using a VAS for various
energy level until 240 shocks/min were reached at level
activities of daily living, and complete the Roles and
7. Fifty (Æ10) shocks were delivered at levels 1–6 as the
Maudsley Pain questionnaire, the AOFAS ankle–hind-
frequency was being increased. Approximately 3,500
foot scale, and the SF-12 Global Health Rating Scale
(Æ10) shock waves were administered at level 7 to reach
before treatment and at follow-up visits. Adverse events
an approximated total energy delivery of 1,300 mJ/mm2
were evaluated by the type, nature, severity, and
(EDþ) or 2,330 mJ/mm2 (ED) (3,800 total shocks).
intensity during treatment and at each follow-up visit.
The Placebo group received the identical treatment
The last follow-up visit for the primary efficacy end-
procedure; however, shock waves were prevented from
entering the subject’s foot by a thin foam cushion placedon the therapy head with an application of ultrasound
gel. The cushion was put in place prior to the subject’sarrival in the treatment room to maintain blinding. A
All statistical analyses were performed using the SAS1
new cushion was used with each treatment session.
System (Cary, NC), with a significance level of 0.05 and
All treatments were performed according to instruc-
on an intention-to-treat basis. The primary analysis
tions in the Epos Ultra Operating Manual. Pain
method was a two-sample t-test comparing treatment
intensity during treatment and immediately posttreat-
groups in the changes from baseline to 3 months post-
ment were recorded, as well as any adverse events
treatment. Statistical testing also included a repeated
resulting during the treatment session. After treatment
measures analysis of the changes from baseline, testing
and at each follow-up visit, blinding was assessed by
for treatment and time main effects, and treatment by
asking subjects to identify which treatment they
interaction effects, with relevant covariates, such as
believed they received. All subjects were instructed to
baseline VAS score, included in the model. The effect of
eliminate athletic activities and pain medication post-
missing data on efficacy results was determined prior to
therapy until the 6 week follow-up evaluation.
analysis. All follow-up, evaluations were included in theanalysis out to 3 months, prior to treatment unblinding. Investigational site effects on the changes in pain score
at 3 months were tested for significance in a two-way
All subjects were evaluated by an independent
analysis of variance. To reduce the size of the residual
(blinded) investigator at 3–5 days, 6 weeks, and
error term used in making inferences on treatment
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
effect at 3 months, analysis of covariance was employed
group missed the 6-week visit. One subject in the
to investigate linear effects of baseline characteristics,
Active group and two subjects in the Placebo
for example, pain, age, or weight. In addition to eva-
group missed the 3-month follow-up visit. Rea-
luating the actual changes in pain score, the proportion
sons for withdrawal are included in Figure 2. At
of subjects achieving at least 60% improvement in pain
3 months, 53 of the 58 subjects from the Active
was compared between treatment groups at 3 months
treatment group and 52 of the 56 subjects from
using a chi-square test. Proportions of subjects experi-
the Placebo group were evaluated (92%).
encing adverse events were also compared betweentreatment groups via Fisher’s Exact tests, whereby the
column totals (denominators) were the total number of
respect to baseline demographics such as age,
gender, height, weight, duration of symptoms,pain on VAS, and characteristics of physicalinspection (Table 2). There were no significant
differences between groups in the baseline data forprevious therapies tried.
One hundred fourteen study participants were
Significant differences were found between
randomly assigned to either the Active treatment
groups on outcomes measured during treatment
group (58) or the Placebo control group (56). Two
including pain and verification of blinding. Forty-
participants in the Active group and two partici-
six of the 58 participants in the Active group
pants in the Placebo group withdrew after the
reported pain during treatment compared to five
follow-up visit at 3–5 days. Two subjects in the
in the Placebo group ( p < 0.0001). There was no
Active group withdrew from the study after
significant difference between groups with regard
the visit at 6 weeks and one subject in the Placebo
to pain reported immediately after treatment.
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
Participate in weekly exercise (No. of pts)
When comparing verification of blinding data,
tently numerically superior to placebo with mar-
34 participants in the Active group believed they
ginal statistical significance ( p < 0.10) between
had received the ESWT treatment when ques-
treatments in these clinical outcomes. Success,
tioned immediately posttreatment versus only
defined as a score of none or mild on the pain
13 in the Placebo group ( p ¼ 0.0007). Twenty-two
portion of the AOFAS ankle–hindfoot scale
participants in the Active group (37.9%) and
was also numerically superior to placebo with
33 (58.9%) in the Placebo group reported they did
marginal statistical significance at 3 months
not know whether they had received the treatment
or not. This was not statistically significant.
In terms of the Secondary Outcomes measures,
With regard to the primary outcome measure, a
no significant difference between groups was
statistically significant difference ( p ¼ 0.0124)
found with the numbers available in any of the
was found in the change from baseline to 3 months
AOFAS ankle–hindfoot indices (Table 3) or the
in the VAS scores of the treated versus Placebo
SF-12 Global Health Rating Scale. However, a
group (Table 3). In the Active treatment group, the
significant difference between groups was deter-
mean pain score decreased from 7.5 to 3.9 at 3
mined on the Roles and Maudsley scores ( p ¼
months ( p < 0.0001), resulting in a mean percen-
0.0121) using a Cochran–Mantel–Haenszel mean
tage improvement of 49.1%. In the Placebo group,
score test and the pain measurement on palpation
the mean pain score decreased from 7.9 to 5.3
( p ¼ 0.0027) using a two-way ANOVA F-test for
at 3 months ( p < 0.0001), a mean percentage
group effect at 3 months posttreatment (Table 3).
Adverse events (other than pain) reported
Clinical success was defined as >60% improve-
during treatment or in the first 3–5 days after
ment from baseline in VAS scores for pain during
treatment were relatively few, and there was no
the first few minutes of walking. Table 3 shows
significant difference in number of side effects
that at 3 months after treatment, there was a
reported between groups through 3 months. The
statistically significant difference between the
adverse events reported were primarily antici-
percentage of Active treatment and Placebo treat-
pated and included ecchymosis, edema, pain, and
ment subjects that met the above definition of a
transient parasthesias. There was one report of
success. In the Active group, 47% (25 of 53) of the
low back pain in the Active group and one of
subjects achieved greater than 60% improvement
pruritis in the Placebo group. Both were deemed
in pain, and in the Placebo group only 23% (12 of
unrelated to the study intervention.
52) met the same criteria ( p ¼ 0.0099). Although
After 3–5 days and through 3 months post-
both Placebo and Active groups also reported
treatment, one participant in the Placebo group
significant improvement in their pain with normal
sustained an accidental injury, which led to
activity, leisure/sport activity, and prior to bed, the
increased pain in the study foot, and one had gene-
improvements in the Active group were consis-
ralized spasms in the study foot following activity.
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
Results for Primary and Secondary Outcome Measures
Primary outcome measurePain during the first few minutes of walking scored on VAS
Defined by >60% improvement on the primary
aDefined as score of none or mild on the pain domain.
bCochran-Mantel-Haenszel mean score test.
The onset of pain and edema during this period
visit (Table 3). Statistical analysis is pending for
were comparable between treatment groups. One
the 6- and 12-month follow-up (Active group) and
subject in the Active Group experienced tingling in
Crossover safety and efficacy data.
the affected foot at the 6-week follow-up visit. Theevent was coded as anticipated/not serious and
resolved by the 3-month visit. One subject in theActive Group experienced peripheral neuritis at
This study demonstrated a statistically signifi-
the 6-week visit. The event was coded as antici-
cant difference between groups in the primary
pated/not serious and resolved prior to the 3 month
outcome measure of change from baseline to
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
3 months after treatment in VAS pain scores in
results. Our results are only valid for the ther-
the first few minutes of walking (49.1% vs. 33.3%;
apeutic variables used in this study. It is difficult
p ¼ 0.0124). Although improvement was noted in
to compare studies, which use different patient
the Placebo group, this phenomenon could simply
populations, energy sources, and treatment proto-
reflect the spontaneous remission or natural his-
cols. It is unclear if the negative results of other
tory of plantar fasciitis as a self-limiting condition
studies are due to insufficient energy levels,
or a sustained placebo effect. Standard treatment
possible over treatment, which can produce a lack
for plantar fasciitis is conservative, but about 10%
of/or negative biologic effect, or inclusion of sub-
of patients fail to respond or heal spontaeously.3
jects who might not benefit from ESWT. The
Because this represents a significant number of
results presented here confirm those of the pre-
people, we consider our findings about the effect
vious randomized controlled trial performed as
of ESWT as an alternative treatment are quite
part of the initial study in which some of the same
relevant and useful. There were also statistically
significant differences between treatments in the
ESWT has several advantages and should be
number of participants whose changes in VAS
considered an effective and safe tool in the treat-
scores met the study definition of success and in
ment of chronic plantar fasciitis. As an alternative
the distribution of Roles and Maudsley pain and
to surgery, it is a noninvasive technology, which
activity self-assessment scores. This provides
has considerably less complications. It has a
further evidence that ESWT does offer an addi-
relatively short recovery time during which the
tional benefit with regard to pain and activity
patient can continue with most employment and
levels to at least 3 months posttreatment. The
activities of daily living, as soon as the day
Roles and Maudsley score is considered to be
following treatment. Finally, because ESWT can
clinically significant for providing patient self-
be used utilized earlier in the course of this disease,
assessment information,2 which in many cases is
it can aid in reducing patient suffering, loss of time
moreimportantthanother clinicaloutcomes.Unfor-
at work, and health care costs associated with
tunately, the study was not powered to show signi-
ficant difference in the SF-12 scale, as this wouldhave required an unfeasible amount of patients.
The significant difference in blinding verifica-
tion between the groups deserves explanation. This most likely was influenced by the subject’s
Present conservative treatments for plantar
judgment about the presence or absence of pain
fasciitis include rest, physical therapy, heel
during treatment, which incidentally was also
cushions, nonsteroidal anti-inflammatory drugs,
statistically significant. The presence or absence of
corticosteroid injections, taping, orthotics, shoe
pain during treatment in either group could be due
modifications, nightsplinting, and casting. ESWT
to several variables such as differences in subject’s
is proposed as an additional conservative treat-
pain tolerance or inconsistent adequacy of the
ment to be used to avoid surgery, when other
available conservative methods have failed. Relief
To truly compare a clinical intervention to
from pain can be recognized with a single session
placebo, as the comparative clinical trials in the
compared to traditional conservative therapies
past have claimed to do, blinding of subjects and
that require multiple applications and for which
assessment of the efficacy of the blinding are
clear benefits have not been established. Shock
necessary to attemp to control the placebo effect.
wave therapy is minimally invasive, has a short
Many previous trials of ESWT for plantar fasciitis
recuperation period, and reports only minor, tran-
did not include blinding or assessment of blinding,
sient side effects. Also, shock wave therapy may
so it is difficult to compare our results in this area
circumvent the need for surgical intervention
to others in the literature. It should be noted that
and the associated costs, lost time from work,
our assessment of the subjects’ blindness to the
and complications associated with surgery.
type of treatment is of interest only for evaluating
The results of this study confirm that high-
our method of blinding, and we can safely conclude
energy ESWT, administered with the Dornier
that our method of blinding worked as well as
Epos Ultra is a safe and effective treatment for
patients who have failed previous conservative
nonsurgical treatments for chronic plantar fascii-
controlled trials published recently with varying
tis. The future of our research of ESWT will include
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
further study of optimal dosing, frequency, and
placebo-controlled double-blind study. Z Orthop
7. Buchbinder R, Ptasznik R, Gordon J, et al. 2002.
therapy for plantar fasciitis: a randomized con-trolled trial. JAMA 288:1364–1372.
All clinical sites received research grant funding from
8. Haake M, Buch M, Schoellner C, et al. 2003. Extra-
Dornier MedTech America, Inc., Atlanta, GA. We grate-
corporeal shock wave therapy for plantar fasciitis:
fully acknowledge the following investigators for their
randomised controlled multicentre trial. BMJ
dedication and participation in the clinical trial: Joyce
Johansson, MD, Alain Scheldeman, B.Sc. PT., CAT(c),
9. Hammer DS, Adam F, Kreutz A, et al. 2003. Extra-
Rory Mullin MSc, ATC, CAT (c), Dac., and Susanne
corporeal shock wave therapy (ESWT) in patients
Pare, Bsc.PT. A special thank you to the many other
with chronic proximal plantar fasciitis: a 2-year
colleagues and especially the Research Coordinators,
follow-up. Foot Ankle Int 24:823–828.
who could not all be named but without whom the study
10. Speed CA, Nichols D, Wies J, et al. 2003. Extra-
corporeal shock wave therapy for plantar fasciitis. A
11. Theodore GH, Buch M, Amendola A, et al. 2004.
Extracorporeal shock wave therapy for the treat-
1. Chaussy C, Eisenberger F, Wanner K. 1976. The
ment of plantar fasciitis. Foot Ankle Int 25:290–297.
use of shock waves for the destruction of renal cal-
12. Ogden JA, Alvarez RG, Marlow M. 2002. Shock-
culi without direct contact. Urol Res 181:352–357.
wave therapy for chronic proximal plantar fasciitis:
2. Roles NC, Maudsley RH. 1972. Radial tunnel
a meta-analysis. Foot Ankle Int 23:301–308.
syndrome: resistant tennis elbow as a nerve
13. Strash WW, Perez RR. 2002. Extracorporeal shock-
entrapment. J Bone Joint Surg Br 54:499–508.
wave therapy for chronic proximal plantar fasciitis.
3. Davis PF, Severud E, Baxter DE. 1994. Painful heel
syndrome: results of non-operative treatment. Foot
14. Ware JE, Kosinski M, Keller SE. 1996. A 12-Item
short-form health survey: construction of scales
4. Ogden JA, Alvarez R, Levitt R, et al. 2001. Shock
and preliminary tests of reliability and validity.
wave therapy for chronic proximal plantar fasciitis.
15. Schon LC. 1993. Plantar fasciitis/heel pain. In
5. Riddle DL, Schappert SM. 2004. Volume of ambu-
Pfeffer GB, Frey CC, Anderson RB, et al., editors.
latory care visits and patterns of care for patients
Current practice in foot and ankle surgery, Vol. 1.
diagnosed with plantar fasciitis: a national study of
New York: McGraw-Hill; pp 243–261.
medical doctors. Foot Ankle Int 25:303–310.
16. Kltaoka HB, Alexander IJ, Adelaar RS, Nunley JA,
6. Abt T, Hopfenmuller W, Mellerowicz H. 2002.
et al. 1994. Clinical rating systems for the ankle-
Shock wave therapy for recalcitrant plantar fascii-
hindfoot, midfoot, hallux, and lesser toes. Foot
tis with heel spur: a prospective randomized
JOURNAL OF ORTHOPAEDIC RESEARCH FEBRUARY 2006
CALENDAR SPONSOR A CHALLENGE CRACK A CHALLENGE SHARE A SOLUTION Home - Share a Solution - Current Solutions - Non-invasive diffusion tracking in pharmacokinetics Print to PDF Send to Friend Current Solutions Non-invasive diffusion tracking in pharmacokinetics Share a Solution Solutions Funding Lein Applied Diagnostics is seeking partners to u
Clozapine, USP ODT Patient Registry Healthcare Practitioner Enrollment Form Instruction: This form is used to enroll a health care practitioner in the Clozapine, USP ODT Patient Registry. Submitting this completed form indicates you have read and agree to the Statement of OBLIGATIONS below. All forms must be signed and dated by the health care practitioner. Health Care Practitioner
 CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
primary safety analysis was also done comparing the
tion. Absence of a calcaneal fracture, bony abnormality,
incidence of adverse events between groups at the time
or other pathology (i.e., tumors) was confirmed with a
of treatment, and during follow-up. All follow-up data
lateral radiograph prior to treatment.
CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
primary safety analysis was also done comparing the
tion. Absence of a calcaneal fracture, bony abnormality,
incidence of adverse events between groups at the time
or other pathology (i.e., tumors) was confirmed with a
of treatment, and during follow-up. All follow-up data
lateral radiograph prior to treatment.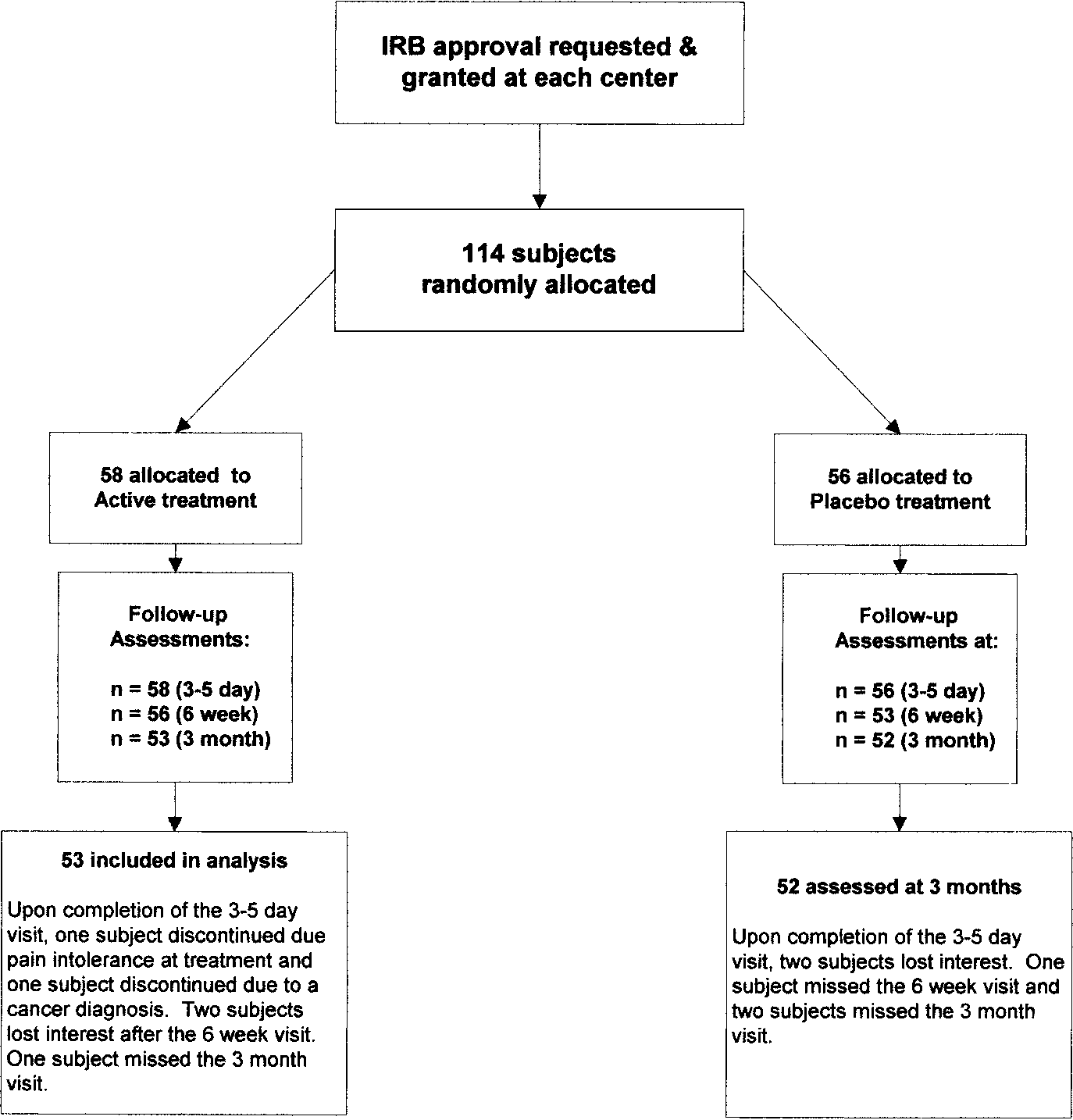 CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
effect at 3 months, analysis of covariance was employed
group missed the 6-week visit. One subject in the
to investigate linear effects of baseline characteristics,
Active group and two subjects in the Placebo
for example, pain, age, or weight. In addition to eva-
group missed the 3-month follow-up visit. Rea-
luating the actual changes in pain score, the proportion
sons for withdrawal are included in Figure 2. At
of subjects achieving at least 60% improvement in pain
3 months, 53 of the 58 subjects from the Active
was compared between treatment groups at 3 months
treatment group and 52 of the 56 subjects from
using a chi-square test. Proportions of subjects experi-
the Placebo group were evaluated (92%).
CONFIRMATORY RCT OF ESWT FOR PLANTAR FASCIITIS
effect at 3 months, analysis of covariance was employed
group missed the 6-week visit. One subject in the
to investigate linear effects of baseline characteristics,
Active group and two subjects in the Placebo
for example, pain, age, or weight. In addition to eva-
group missed the 3-month follow-up visit. Rea-
luating the actual changes in pain score, the proportion
sons for withdrawal are included in Figure 2. At
of subjects achieving at least 60% improvement in pain
3 months, 53 of the 58 subjects from the Active
was compared between treatment groups at 3 months
treatment group and 52 of the 56 subjects from
using a chi-square test. Proportions of subjects experi-
the Placebo group were evaluated (92%).