Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Doi:10.1016/j.ajog.2005.05.074
American Journal of Obstetrics and Gynecology (2006) 194, 138–43
Selective use of fetal fibronectin detection after cervicallength measurement to predict spontaneous pretermdelivery in women with preterm labor
Thomas Schmitz, MD,a,* Franc¸oise Maillard, MSc,b Sandrine Bessard-Bacquaert, MD,aGilles Kayem, MD,c Yvonne Fulla, MD,d Dominique Cabrol, MD, PhD,aFranc¸ois Goffinet, MD, PhDa,b
Maternite´ Port-Royal,a De´partement de Me´decine Nucle´aire,d Hopital Cochin, AP-HP, Universite´ Rene´ DescartesParis V, INSERM U149,b Pavillon Baudelocque, Paris, France; Service de Gyne´cologie et Obste´trique,c CentreHospitalier Intercommunal de Cre´teil, Universite´ Paris XII, Cre´teil, France
Received for publication January 11, 2005; revised April 18, 2005; accepted May 18, 2005
Objective: The purpose of this study was to determine whether selective use of fetal fibronectin
detection after ultrasound measurement of cervical length predicts preterm delivery in
symptomatic patients better than either indicator alone.
Study design: This prospective blinded study performed both tests on 359 women hospitalized
for preterm labor between 18 and 34 completed weeks’ gestation. The primary outcome waspreterm delivery before 35 weeks’gestation. Results: Among the 359 women included, 48 (13.4%) delivered before 35 weeks’ gestation. Thesensitivity, specificity, and positive and negative predictive values of cervical length %25 mm were75%, 63%, 24%, and 94%, respectively, and of fetal fibronectin R50 ng/mL, 63%, 81%, 33%,and 93%. Fetal fibronectin detection was significantly (P ! .001) more specific than cervicallength measurement. For selective use of fetal fibronectin detection after cervical lengthmeasurement, the test was considered positive if cervical length was %15 mm or if cervical lengthwas between 16 and 30 mm with fetal fibronectin R50 ng/mL. The predictive values of this testwere not significantly different from those of fetal fibronectin detection (67%, 81%, 36%, and94%). This strategy could have avoided 200 fibronectin tests. Conclusion: Selective use of fetal fibronectin detection after cervical length measurement is morespecific than cervical length and as effective as fetal fibronectin assays in the entire population ofwomen in preterm labor for predicting preterm birth. Ó 2006 Mosby, Inc. All rights reserved.
Preterm birth is the main cause of perinatal morbidity
and mortThe rate of preterm delivery has notdecreased significantly the last 20 years and preterm
* Reprint requests: Dr Thomas Schmitz, Maternite´ Port-Royal,
birth still accounts for 6.8% of all deliveries in Franc
123 Boulevard de Port-Royal, 75014 Paris, France.
This situation can be explained, at least in part, by the
0002-9378/$ - see front matter Ó 2006 Mosby, Inc. All rights reserved. doi:10.1016/j.ajog.2005.05.074
lack of reliable criteria for selecting populations at high
General characteristics and pregnancy outcomes of
risk for preterm delivery to provide them with special
monitoring and prevention. Indeed, both cervical clin-
ical examinationand uterine contraction frequency
have poor sensitivity and specificity for predicting pre-term birth in patients with preterm labor and, thus,
produce high rates of false-negatives and false-positives.
High false-negative rates result in unpredicted preterm
birth of infants delivered without the benefits of corti-
costeroids and tertiary neonatal care, whereas high rates
of false-positives are responsible for unnecessary and
potentially hazardous treatments.New markers for the
prediction of preterm birth have therefore been devel-
oped. Among them, transvaginal ultrasonographic mea-
surement of cervical length and detection of fetal
fibronectin in cervicovaginal fluids both show particular
promise for improving the prediction rate for preterm
delivery.However, despite a considerable literature,
no clear, rational, and evaluated strategy for a daily
practical use of these new markers has emerged, mainly
because too few studieshave assessed the combined
or selective use of fetal fibronectin detection after
cervical length measurement for evaluating the risk of
In the present prospective study, our goal was to
Mean interval between inclusion and delivery
determine whether the selective use of fetal fibronectin
detection after ultrasound cervical length measurement
was more effective than either indicator alone for
predicting preterm delivery in patients with preterm
eclampsia, or medically indicated preterm delivery be-
fore 35 weeks’ gestation. Gestational age was establishedby the date of the last menstrual period and confirmed
This prospective blinded study was conducted between
by ultrasonography performed during the first trimester
January 1997 and May 2000 at the tertiary university
of pregnancy. If menstrual dates were unreliable or
Port-Royal Maternity Hospital. The protocol was
discordant by more than 5 days, gestational age was set
approved by the local ethics committee (Conseil Consul-
tatif Pour la Participation a` la Recherche Biome´dicale–
Vaginal sampling for fetal fibronectin and cervical
CCPPRB) of Cochin Hospital. All subjects gave
length measurement were performed at admission dur-
informed consent at the time of screening in accordance
ing the same consultation in the emergency room of the
with our institutional review board policies. Women
maternity. Each subject was first examined with a
were eligible for the study if they were hospitalized for
vaginal speculum. A Dacron swab was rotated in the
preterm labor at the maternity between 18 and 34 weeks
posterior fornix of the vagina and sent to the labo-
and 6 days of gestation. Preterm labor was defined by
ratory. Fetal fibronectin concentrations were measured
regular uterine contractions 30 seconds in duration at a
by enzyme-linked immunosorbent assay (ELISA) with
rate of at least 4 contractions per 30 minutes, confirmed
the specific monoclonal antibody FDC-6. Results were
by external uterine tocodynamometry, and cervical dila-
tation of 0 to 3 cm (nulliparous women) or 1 to 3 cm
Ultrasound examination of the cervix was performed
(primiparous or multiparous women) and 50% cervical
as soon as the uterine activity recording ended. Cervical
effacement. Patients were excluded in case of cervical
length was measured in the sagittal plane by the follow-
manipulation or sexual intercourse within the previous
ing standardized technique used in our maternity.
24 hours, multiple pregnancy, confirmed rupture of
A Hitachi (Tokyo, Japan) EUB-405 ultrasonography
membranes, cervical dilatation R3 cm, cervical cerclage,
machine with a 6.5 MHz transvaginal transducer was
uterine anomalies, vaginal bleeding, placenta previa,
used. Each examination, performed with an empty
abruptio placentae, intrauterine growth restriction, pre-
bladder to avoid a deceptively elongated image, began
Comparison of receiver-operator characteristic
Comparison of receiver-operator characteristic
curves constructed for cervical length and fetal fibronectin
curves constructed for cervical length and fetal fibronectin
levels in prediction of preterm delivery before 35 weeks’
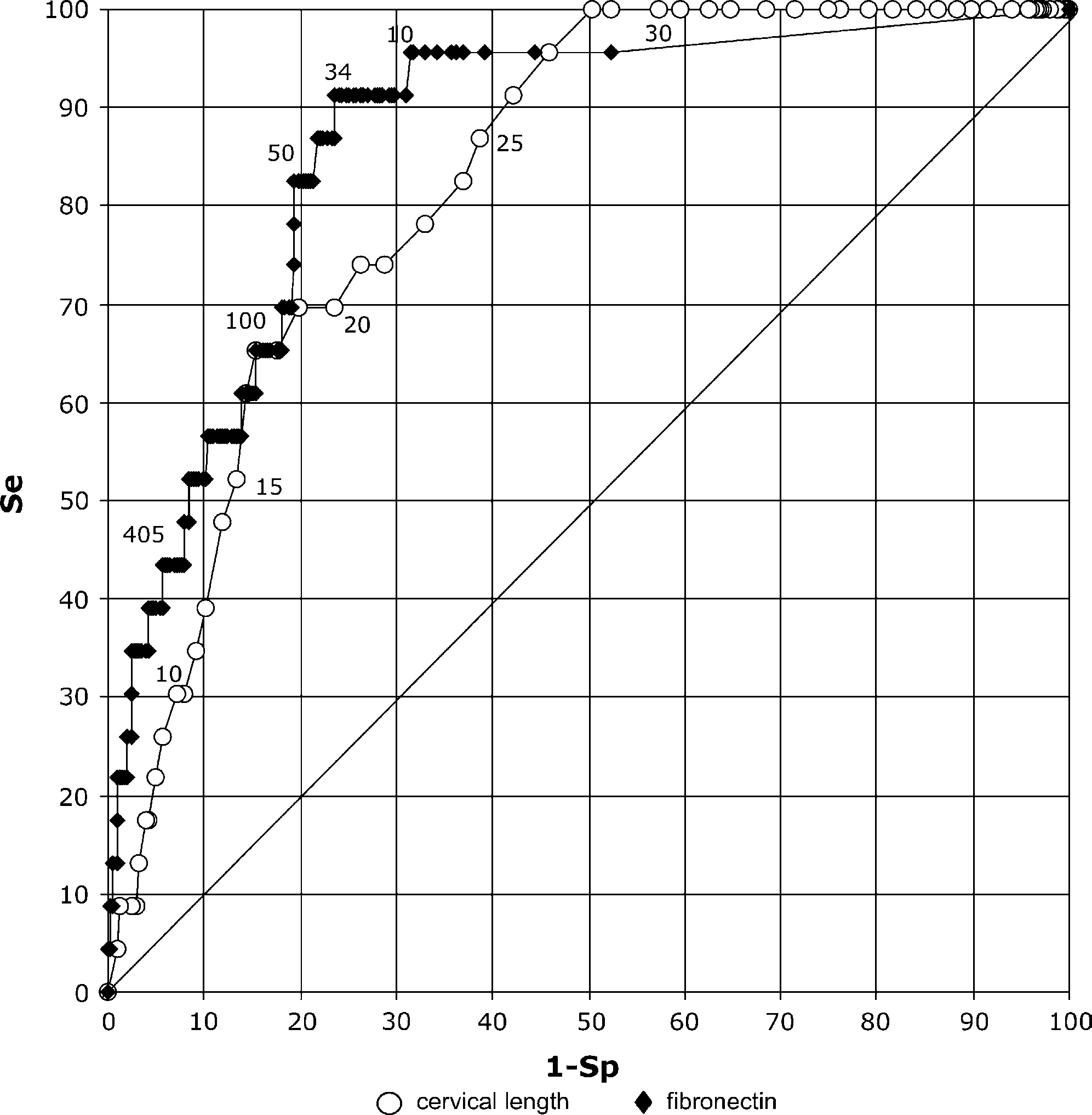
levels in prediction of preterm delivery within 7 days. Areas
gestation. Areas under the cervical length (0.758) and fetal
under the cervical length (0.826) and fetal fibronectin (0.868)
fibronectin (0.797) curves did not differ significantly (P = .47).
curves did not differ significantly (P = .28). Areas under both
Areas under both curves differed significantly from the area
curves differed significantly from the area (0.500) under the 45-
(0.500) under the 45-degree diagonal line of unity (P ! .001
degree diagonal line of unity (P ! .001 and P ! .001,
by placing the transducer on the cervix and identifying
algorithm with Stata Software (College Station, TX)
the internal cervical os, the cervical canal, and the
and compared using the c2 test. For selective use of fetal
external os. Pressure on the transducer was then relaxed
fibronectin detection after cervical length measurement,
to the point at which the image blurs before enough
we retrospectively analyzed the predictive values of fetal
gentle pressure to recreate a clear cervical image was
fibronectin of ultrasonography-selected women. The
cervical length cutoffs were chosen to provide high
During the study period, results of ultrasound exam-
sensitivity and specificity values. Predictive values and
ination of the cervix and fetal fibronectin assay were
likelihood ratios with their 95% confidence interval were
blinded to the obstetric team and did not influence
first calculated for each test considered separately, then
subsequent patient management. Hospitalization was
for the 2 markers used selectively and compared with
decided exclusively on clinical grounds, ie, syste-
matic digital examination of the cervix and uterinecontractions. Tocolytic therapy and corticosteroidswere administered on the discretion of the attending
physician. Salbutamol was the main tocolytic drugprescribed and was maintained until contractions dis-
Between January 1997 and May 2000, 815 women
appeared. The infusion flow was then progressively
consulted at Port-Royal Maternity Hospital for preterm
reduced and finally withdrawn when judged possible.
labor. After exclusion of 137 women with multiple
pregnancies, 123 with preterm premature rupture of
The primary outcome measure was delivery before 35
membranes, 34 with both multiple pregnancy and pre-
weeks’ gestation. The secondary outcome measure was
term premature rupture of membranes, and 16 women
delivery within 7 days following inclusion. To determine
at a term equal to 35 weeks, 505 women were eligible for
the most useful cutoff point for cervical length and fetal
the study, 445 (88%) of whom had cervical length
fibronectin, we constructed receiver-operator character-
measured with ultrasound and 403 (80%) of whom
istic (ROC) curves. The areas under the ROC curves
had fetal fibronectin assayed. Reasons that 1 or both
were calculated following the Delong and Clark-Pearson
tests were not always performed for every eligible
Predictive values for preterm birth of cervical length, fetal fibronectin, and selective use of fetal fibronectin in
ultrasonography-selected patients (n = 359)
Se (%) (95% CI) Sp (%) (95% CI) PPV (%) (95% CI) NPV (%) (95% CI) LRC (95% CI)
To analyze selective use of fetal fibronectin in ultrasonography-selected patients (selective test), we considered the test positive if cervical length was%15 mm or between 16 and 30 mm with fetal fibronectin R50 ng/mL. The test was considered negative if cervical length was O30 mm or between 16and 30 mm with fetal fibronectin !50 ng/mL. CL, Cervical length; fFn, fetal fibronectin; Se, sensitivity; Sp, specificity; PPV, positive predictive value;NPV, negative predictive value; LRC, likelihood ratio for a positive result; LRÿ, likelihood ratio for a negative result.
* n = 48. y n = 23. z P = .24 vs CL. x P = .29 vs CL. { P = 1.0 vs CL.
Predictive values for preterm birth of various cervical length cutoff values (n = 359)
CL, Cervical length; Se, sensitivity; Sp, specificity; PPV, positive predictive value; NPV, negative predictive value.
women included: no available ultrasound operator,
were the best cutoff points for predicting preterm birth
cervical manipulation or sexual intercourse within the
previous 24 hours, or vaginal bleeding. Finally, 370
patients (73%) had both tests, but 2 were respectively
sensitive but less specific than fetal fibronectin O50 ng/
excluded from the analysis because of labor induction
mL for predicting preterm birth both before 35 weeks’
and 9 for planned cesarean section before 35 weeks.
Therefore, the final study population consisted of the
We decided to evaluate fetal fibronectin detection in
cervical ultrasonography-selected patients based firstly
The general characteristics of the population are
on the high sensitivity and negative predictive value of
given in Preterm delivery rates before 35 weeks’
cervical length %30 mm for predicting preterm birth
gestation and within 7 days following inclusion were
and secondly on the high specificity of cervical length
13.4% (48/359) and 6.4% (23/359), respectively. Cervi-
%15 mm. Indeed, when a 30 mm cutoff was chosen, the
cal length and fetal fibronectin ROC curves were
sensitivity of the test for predicting preterm birth before
significantly above the 45-degree diagonal line of unity
35 weeks’ and within 7 days was 90% and 100%,
but areas under the curves did not differ significantly
respectively, with negative predictive values of 97%
(). ROC curve analysis of cervical length
and fetal fibronectin showed that 25 mm and 50 ng/mL
mm, specificity was 89% for delivery before 35 weeks
Predictive values for preterm birth of fetal fibronectin for women with cervical length between 16 and 30 mm (n = 159)
fFn, Fetal fibronectin, Se, sensitivity; Sp, specificity; PPV, positive predictive value; NPV, negative predictive value.
these new markers, used separately or in combination, in
cervical length values between 16 and 30 mm (
any single population.Indeed, current protocols for
fetal fibronectin detection was more specific than cervi-
the management of preterm laborrely on data
cal length measurement with a 25 mm cutoff (P ! .001)
extracted from heterogenous populations. Second, se-
(Therefore, to analyze selective use of fetal
lective use of these new markers, by combining the
fibronectin after cervical length measurement, we con-
strength of the 2 tests, could further reduce the high
sidered that patients were at high risk of preterm birth
rates of false-positives resulting from the poor specificity
if their cervical length was %15 mm or between 16 and
of the clinical indicators. This false-positive rate results
30 mm with a fetal fibronectin concentration R50 ng/mL.
in prescription of unnecessary tocolytic and glucocorti-
Patients were at low risk if their cervical length was
coid therapies and in utero transfer. Third, performing
O30 mm or between 16 and 30 mm with a fetal
fetal fibronectin detection only in ultrasonography-
fibronectin !50 ng/mL. In this 2-step strategy, the first
selected patients could be helpful in reducing the num-
step, based on cervical length measurement, is very
sensitive (90% and 100%), and the second step, based
We evaluated the selective use of fetal fibronectin
on fetal fibronectin detection in patients with cervical
detection after cervical length measurement for predict-
length between 16 and 30 mm, is specific, with spec-
ing preterm birth before 35 weeks’ gestation and within
ificity values of 83% and 82% (The spec-
7 days following inclusion. By constructing ROC curves,
ificity of fetal fibronectin detection used selectively as
we first determined that 25 mm and 50 ng/mL were the
mentioned here was significantly greater (P ! .001)
best cutoff points for these 2 markers. These values are
than that of cervical length measurement (
in accordance with what is commonly reported in
Predictives values of the selective test and of fetal
fibronectin detection in the entire population of women
Fetal fibronectin detection in cervical ultrasonogra-
in preterm labor did not differ significantly (
phy-selected patients provided excellent negative predic-
However, this 2-step strategy could have avoided 200
tive values (94% and 99%) for a delivery both before 35
fibronectin tests thus reducing their number
weeks’ and within 7 days. Fetal fibronectin used selec-
tively in a daily obstetric practice could thus provide the
Further analysis according to patient origin (trans-
clinician with a specific test on which a decision not to
ferred patients or not) or gestational age at admission
treat may be based. Furthermore, the positive predictive
(before or after 28 weeks’ gestation) did not modify the
values, although less impressive, seem higher than those
of cervical examination or uterine contraction fre-quency.Accordingly, this selective test may lead to areduction in the number of unnecessary or potentially
hazardous treatments now administered because of thepoor capabilities of the clinical indicators. Fetal fibro-
The aim of this study was to evaluate in the same
nectin detection in patients selected by cervical ultraso-
population a practical strategy for selective use of fetal
nography predicts preterm birth before 35 weeks and
fibronectin detection after cervical length measurement
within 7 days with greater specificity than cervical length
in women with preterm labor. Such studies are needed
measurement and as effectively as fetal fibronectin in the
for several different reasons. First, although use of
entire preterm labor population but decreases the num-
cervical length measurement and fetal fibronectin detec-
ber of fetal fibronectin tests by 55%. This 2-step strategy
tion in the management of women with preterm labor
therefore requires fewer than half as many fetal fibro-
has decreased false-positive and false-negative rates,
nectin detection tests as the 1-step combination we
there are very few reports of the predictive values of
actually used, when we prescribed both tests to every
patient. We must note, however, that selective use of
detection in the entire preterm labor population for
fetal fibronectin is not possible with the current test
predicting preterm birth, and it reduces the number of
because fetal fibronectin detection by ELISA provides
fetal fibronectin ELISA tests performed by 55%. There-
delayed results, and decisions about tocolysis and cor-
fore, once an effective fetal fibronectin bedside test is
ticoid administration cannot yet be postponed until
available, fetal fibronectin might usefully be assayed only
these results are ready. The benefits from the strategy
in women with cervical lengths between 16 and 30 mm.
described above depend on the availability of a reliablebedside test as effective as ELISA. The practical interestof our results thus lies in their use in planning future
studies to evaluate the impact of a bedside fibronectin
1. Stevenson DK, Wright LL, Lemons JA, Oh W, Korones SB,
test performed only in ultrasonography-selected patients
Papile LA, et al. Very low birth weight outcomes of the National
Institute of Child Health and Human Development Neonatal
Previous studies have compared the predictive values
Research Network, January 1993 through December 1994. Am J
of cervical length measurement and fetal fibronectin
2. Blondel B, Norton J, Mazaubrun C, Breart G. Evolution des
detection within a single population. Rizzo et al,
principaux indicateurs de la sante´ pe´rinatale en France me´tropol-
however, did not present results regarding predictive
itaine entre 1995 et 1998. Re´sultats des enqueˆtes nationales
values for the combined use of sonography and fibro-
pe´rinatales. J Gynecol Obstet Biol Reprod 2001;30:552-64.
nectin, while Rozenberg et alused a 1-step combina-
3. Iams JD, Casal D, McGregor JA, Goodwin TM, Kreaden US,
tion of the 2 techniques (both tests performed for every
Lowensohn R, et al. Fetal fbronectin improves the accuracy ofdiagnosis of preterm labor. Am J Obstet Gynecol 1995;173:141-5.
patient) and concluded that the additional information
4. King JF, Keirse MJNC, Chalmers I. Betamimetics in preterm
about the fibronectin level provided only slight benefits.
labor: an overview of the randomised clinical trials. BJOG
Gomez et al, on the contrary, reported recently that
adding consideration of fetal fibronectin results to those
5. Gomez R, Galasso M, Romero R, Mazor M, Sorokin Y,
of cervical length measurement significantly improved
Goncalves L, et al. Ultrasonographic examination of the uterinecervix is better than cervical digital examination as a predictor of
the prediction of preterm delivery.Their report did
the likelihood of premature delivery in patients with preterm labor
not, however, provide information about the predictive
and intact membranes. Am J Obstet Gynecol 1994;171:956-64.
values of a combined test with cervical length and fetal
6. Leitich H, Brunbauer M, Kaider A, Egarter C, Husslein P.
fibronectin. The first group to evaluate a 2-step strategy
Cervical length and dilatation of the internal cervical os detected
was Hincz et al.They assayed fetal fibronectin in cases
by vaginal ultrasonography as markers for preterm delivery:a systematic review. Am J Obstet Gynecol 1999;181:1465-72.
where the cervical length was between 21 and 31 mm
7. Lockwood CL, Senyei AE, Dische M. Fetal fibronectin in cervical
and concluded that sequential use of cervical sonogra-
and vaginal secretions as a predictor of preterm delivery. N Engl J
phy and fetal fibronectin testing produced higher sensi-
tivity and a better negative predictive value than either
8. Honest H, Bachmann LM, Gupta JK, Kleijnen J, Khan KS.
of these methods alone. Nevertheless, the primary end
Accuracy of cervicovaginal fetal fibronectine test in predicting riskof spontaneous preterm birth: systematic review. BMJ 2002;325:
point of their study was delivery within 28 days, which
raises significant doubts about the clinical interest of
9. Rizzo G, Capponi A, Arduini D, Lorido C, Romanini C. The
their results: because patients were included through 34
value of fetal fibronectin in cervical and vaginal secretions and of
weeks, they may have delivered at term. The Ohio State
ultrasonic examination of the uterin cervix in predicting premature
protocol has also proposed performing fetal fibronectin
delivery for patient with preterm labor and intact membranes. Am J Obstet Gynecol 1996;175:1146-51.
detection only when clinical and sonography data are
10. Rozenberg P, Goffinet F, Malagrida L, Giudicelli Y, Perdu M,
equivocal (eg, dilatation 2 cm and cervical length
Houssin I. Evaluating the risk of preterm delivery: a comparison of
between 20 and 30 mm).This strategy is based on
fetal fibronectin and transvaginal ultrasonographic measurement
findings in the literature from a variety of populations.
of cervical length. Am J Obstet Gynecol 1997;176:196-9.
Because the sensitivity and specificity of the selective test
11. Gomez R, Romero R, Medina L, Nien JK, Chaiworapongsa T,
Carstens M, et al. Cervicovaginal fibronectin improves the predic-
did not fall when we assayed fetal fibronectin only in
tion of preterm delivery based on sonographic cervical length in
ultrasonography-selected patients, our results confirm
patients with preterm uterine contractions and intact membranes.
the strategy suggested by Iams et al.Its impact on
preterm birth rates, duration of hospitalization, and
12. Hincz P, Wilczynski J, Kosarzewski M, Szaflik K. Two-step test:
tocolytic treatments now needs to be evaluated.
the combined use of fetal fibronectin and sonographic examinationof the uterine cervix for prediction of preterm delivery in symp-
In conclusion, fetal fibronectin in cervical ultraso-
tomatic patients. Acta Obstet Gynecol Scand 2002;81:58-63.
nography-selected patients is more specific than cervical
13. Iams JD. Prediction and early detection of preterm labor. Obstet
length measurement and as effective as fetal fibronectin
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Guideline title Hip fracture: the management of hip fracture in adults 1.1 Short title The remit The Department of Health has asked NICE: ”to prepare a clinical guideline on the management of fractured neck of femur”. Clinical need for the guideline 3.1 Epidemiology About 70–75,000 hip fractu
Definition SHBG erniedrigt, v.a. bei adipösen u. insulinresistenten Frauen 17-OH-Progesteron hochnormal (vermehrte ovarielle Inhibin B erhöht, in der frühen Follikelphase fast Polizystische Ovarien (mind. 12 kleinzystische Strukturen <10mm DM und/oder vergrössertes ovarielles Volumen >10mL (HxBxL / 2). ) AMH erhöht, korreliert mit Ovargrösse u. Follikelzahl 2 von 3 Kriterie
 American Journal of Obstetrics and Gynecology (2006) 194, 138–43
Selective use of fetal fibronectin detection after cervicallength measurement to predict spontaneous pretermdelivery in women with preterm labor
Thomas Schmitz, MD,a,* Franc¸oise Maillard, MSc,b Sandrine Bessard-Bacquaert, MD,aGilles Kayem, MD,c Yvonne Fulla, MD,d Dominique Cabrol, MD, PhD,aFranc¸ois Goffinet, MD, PhDa,b
Maternite´ Port-Royal,a De´partement de Me´decine Nucle´aire,d Hopital Cochin, AP-HP, Universite´ Rene´ DescartesParis V, INSERM U149,b Pavillon Baudelocque, Paris, France; Service de Gyne´cologie et Obste´trique,c CentreHospitalier Intercommunal de Cre´teil, Universite´ Paris XII, Cre´teil, France
Received for publication January 11, 2005; revised April 18, 2005; accepted May 18, 2005
Objective: The purpose of this study was to determine whether selective use of fetal fibronectin
detection after ultrasound measurement of cervical length predicts preterm delivery in
symptomatic patients better than either indicator alone.
American Journal of Obstetrics and Gynecology (2006) 194, 138–43
Selective use of fetal fibronectin detection after cervicallength measurement to predict spontaneous pretermdelivery in women with preterm labor
Thomas Schmitz, MD,a,* Franc¸oise Maillard, MSc,b Sandrine Bessard-Bacquaert, MD,aGilles Kayem, MD,c Yvonne Fulla, MD,d Dominique Cabrol, MD, PhD,aFranc¸ois Goffinet, MD, PhDa,b
Maternite´ Port-Royal,a De´partement de Me´decine Nucle´aire,d Hopital Cochin, AP-HP, Universite´ Rene´ DescartesParis V, INSERM U149,b Pavillon Baudelocque, Paris, France; Service de Gyne´cologie et Obste´trique,c CentreHospitalier Intercommunal de Cre´teil, Universite´ Paris XII, Cre´teil, France
Received for publication January 11, 2005; revised April 18, 2005; accepted May 18, 2005
Objective: The purpose of this study was to determine whether selective use of fetal fibronectin
detection after ultrasound measurement of cervical length predicts preterm delivery in
symptomatic patients better than either indicator alone.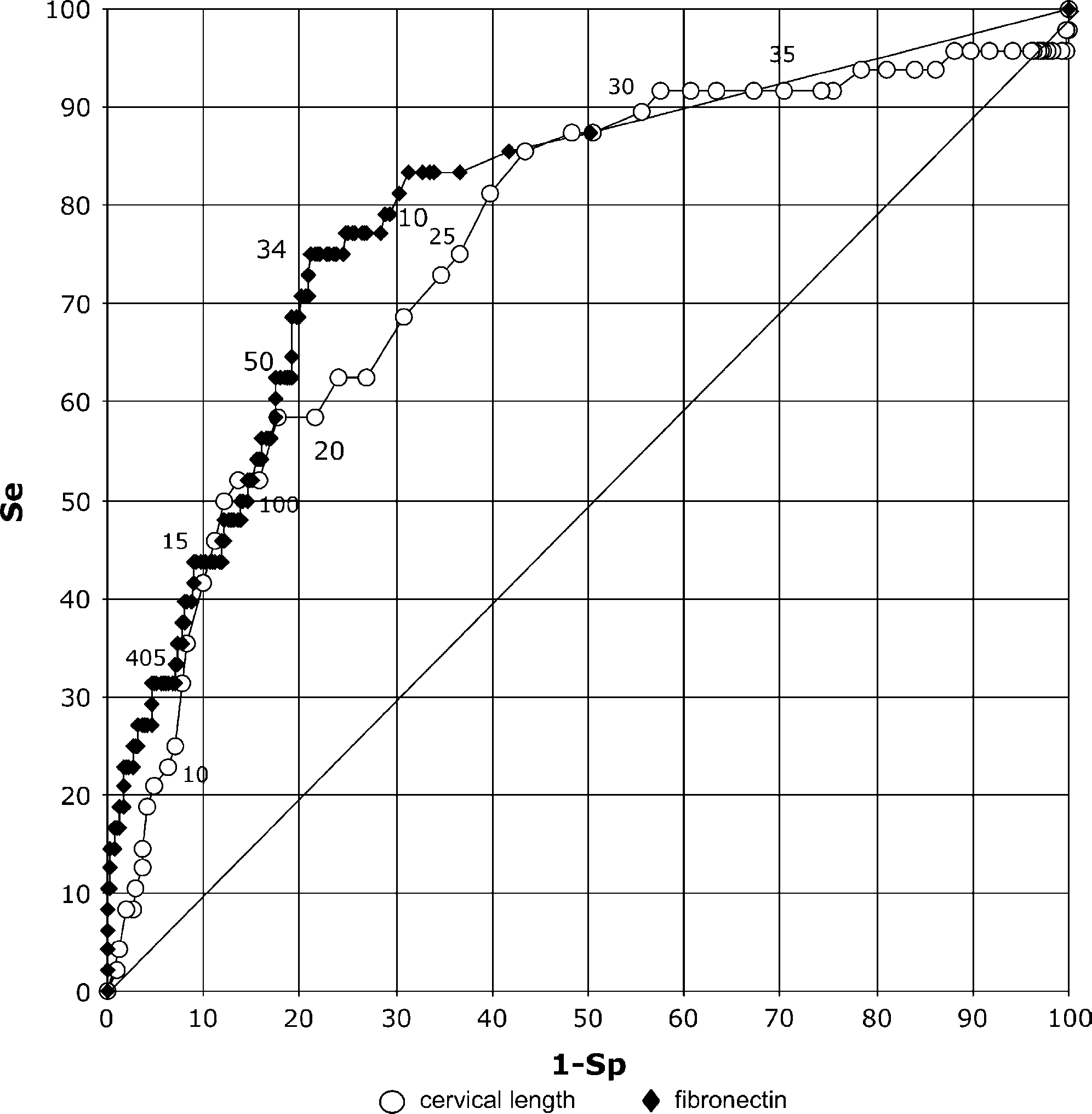
 Comparison of receiver-operator characteristic
Comparison of receiver-operator characteristic
curves constructed for cervical length and fetal fibronectin
curves constructed for cervical length and fetal fibronectin
levels in prediction of preterm delivery before 35 weeks’
levels in prediction of preterm delivery within 7 days. Areas
gestation. Areas under the cervical length (0.758) and fetal
under the cervical length (0.826) and fetal fibronectin (0.868)
fibronectin (0.797) curves did not differ significantly (P = .47).
Comparison of receiver-operator characteristic
Comparison of receiver-operator characteristic
curves constructed for cervical length and fetal fibronectin
curves constructed for cervical length and fetal fibronectin
levels in prediction of preterm delivery before 35 weeks’
levels in prediction of preterm delivery within 7 days. Areas
gestation. Areas under the cervical length (0.758) and fetal
under the cervical length (0.826) and fetal fibronectin (0.868)
fibronectin (0.797) curves did not differ significantly (P = .47).