Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
052401 medical treatment of peripheral arterial disease
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Nevertheless, patients with peripheral arterial diseaseare undertreated with regard to the use of lipid-lower-ing and antiplatelet drugs, as compared with patients
A L A S T A I R J . J . W O O D , M . D. , EditorCLINICAL MANIFESTATIONS MEDICAL TREATMENT OF PERIPHERAL
Approximately one third of patients with periph-
ARTERIAL DISEASE AND
eral arterial disease have typical claudication (Table 1),
CLAUDICATION
defined as pain in one or both legs on walking, pri-marily affecting the calves, that does not go away withcontinued walking and is relieved by rest.25 In patients
with claudication, the severity of the condition increas-es slowly; 25 percent have worsening claudication, and5 percent undergo an amputation within five years.26
ERIPHERAL arterial disease, which is caused
Less than 5 to 10 percent of patients have critical leg
by atherosclerotic occlusion of the arteries to the
ischemia (ischemic pain in the distal foot, ischemic ul-
legs, is an important manifestation of systemic
ceration, or gangrene), but their risk of limb loss is
atherosclerosis. The age-adjusted prevalence of periph-
substantial.19 More than 50 percent of patients iden-
eral arterial disease is approximately 12 percent, and
tified as having peripheral arterial disease on the basis
the disorder affects men and women equally (Table
of an abnormal ankle–brachial index value do not have
1).7,8 Patients with peripheral arterial disease, even in
typical claudication or limb ischemia at rest but, in-
the absence of a history of myocardial infarction or
stead, have other types of leg pain on exertion, with
ischemic stroke, have approximately the same relative
reduced ambulatory activity and quality of life.27,28
risk of death from cardiovascular causes as do patients
Thus, most patients with peripheral arterial disease
with a history of coronary or cerebrovascular disease
have a reduced functional capacity that limits their abil-
(Table 2).12,15 In patients with peripheral arterial dis-
ease, the rate of death from all causes is approximate-
The goals of treatment for patients with claudica-
ly equal in men and women and is elevated even in
tion are to relieve their exertional symptoms, improve
asymptomatic patients. The severity of peripheral ar-
their walking capacity, and improve their quality of
terial disease is closely associated with the risk of my-
life. These goals are similar for patients with critical
ocardial infarction, ischemic stroke, and death from
leg ischemia, with the additional goals of relieving is-
vascular causes. The lower the ankle–brachial index
chemic pain at rest, healing ischemic ulceration, and
(Fig. 1), the greater the risk of cardiovascular events.17,18
preventing limb loss. The overall approach to the di-
Patients with critical leg ischemia (the most severe
agnosis and treatment of peripheral arterial disease was
clinical manifestation of peripheral arterial disease),
extensively reviewed in a recent consensus publication
who have the lowest ankle–brachial index values, have
that provides a comprehensive discussion of the med-
ical and surgical therapies for the disease.29 This review
The major risk factors for peripheral arterial disease
will focus on risk-factor modification and antiplatelet
are older age (over 40 years), cigarette smoking, and
therapies, as well as strategies for symptomatic relief in
diabetes mellitus. Hyperlipidemia, hypertension, and
patients with peripheral arterial disease. Diagnosis and
hyperhomocysteinemia are also important risk fac-
management are summarized in Figures 2 and 3.
tors.5,8,20 Because of the presence of these risk factors,the systemic nature of atherosclerosis, and the high risk
MODIFICATION OF RISK FACTORS
of ischemic events, patients with peripheral arterial
Smoking Cessation
disease should be considered candidates for second-ary-prevention strategies that include aggressive risk-
Smoking cessation slows the progression to critical
factor modification and antiplatelet-drug therapy.21,22
leg ischemia and reduces the risks of myocardial infarc-tion and death from vascular causes.30 It is not certainwhether smoking cessation reduces the severity of
From the Section of Vascular Medicine, Divisions of Geriatrics and Car-
claudication. The authors of a meta-analysis of pub-
diology, Department of Medicine, University of Colorado School of Med-
lished data concluded that smoking cessation did not
icine, and the Colorado Prevention Center, Denver. Address reprint re-
improve maximal treadmill walking distance.31 Smok-
quests to Dr. Hiatt at the Colorado Prevention Center, 789 Sherman St.,Suite 200, Denver, CO 80203, or at [email protected].
ing-cessation programs, nicotine-replacement therapy,
1608 · N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y TABLE 1. PREVALENCE OF PERIPHERAL ARTERIAL DISEASE, CLAUDICATION, PREVALENCE PREVALENCE OF CLINICAL OF PERIPHERAL PREVALENCE OF CARDIOVASCULAR SUBJECTS ARTERIAL DISEASE CLAUDICATION
*An ankle–brachial index value of less than 0.90 was considered diagnostic of peripheral arterial
disease in all the studies. Dashes indicate that no data were presented. TABLE 2. RISKS OF DEATH FROM ALL CAUSES AND FROM CARDIOVASCULAR CAUSES IN PATIENTS SUBJECTS DEATH FROM ALL CAUSES DEATH FROM CARDIOVASCULAR DISEASE
*RR denotes relative risk, and CI confidence interval. Dashes indicate that no data were presented.
and the use of antidepressant drugs such as bupro-
of atherosclerotic risk, such as serum P-selectin con-
centrations.34,35 A meta-analysis was performed of ran-domized trials of lipid-lowering therapy in 698 pa-
Treatment of Hyperlipidemia
tients with peripheral arterial disease who were treated
Several large clinical trials have determined the ben-
with a variety of therapies, including diet, cholestyr-
efits of lowering cholesterol concentrations in patients
amine, probucol, and nicotinic acid, for four months
with coronary artery disease.33 In patients with pe-
to three years.36 The total mortality was 0.7 percent
ripheral arterial disease, therapy with a statin not only
in the treated patients, as compared with 2.9 percent
lowers serum cholesterol concentrations, but also im-
in the patients given placebo — a nonsignificant dif-
proves endothelial function, as well as other markers
ference. This analysis also demonstrated that lipid-
N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org · 1609
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
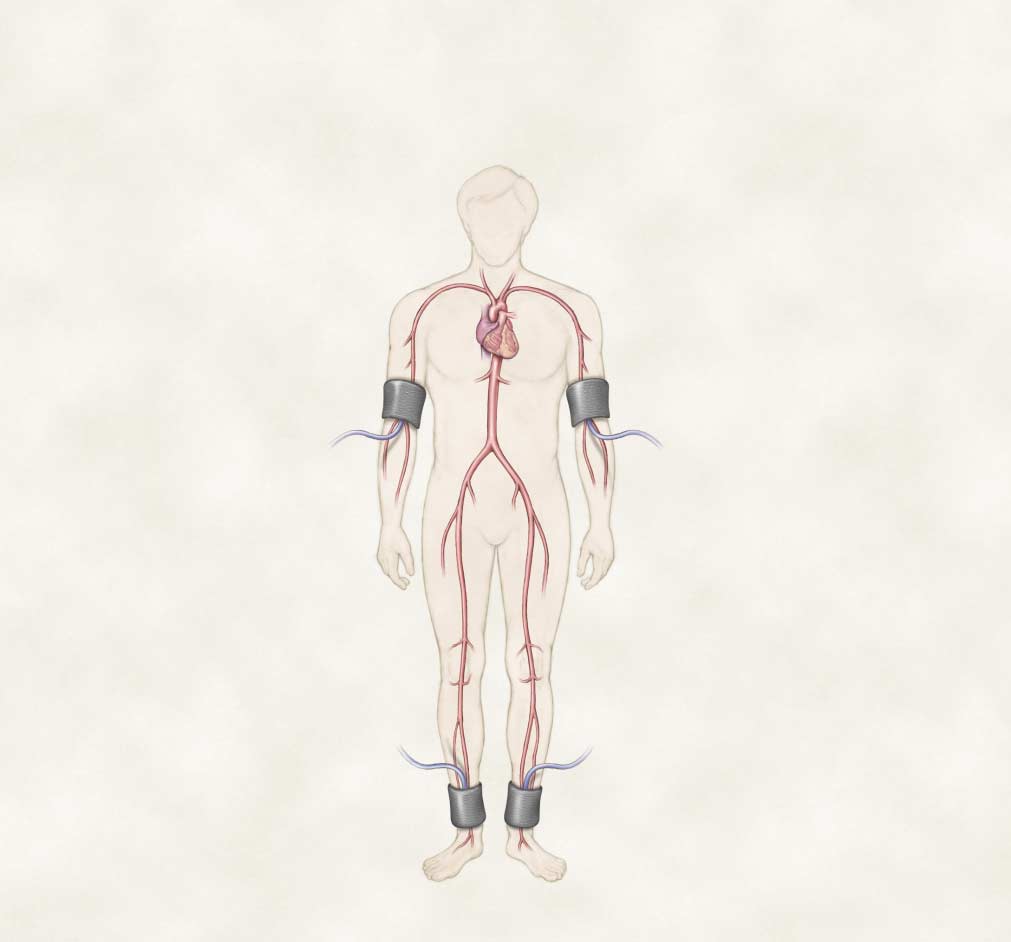
Interpretation of ABI Right ABI > 1.30 Noncompressible 0.91–1.30 0.41–0.90 Mild-to-moderate peripheral arterial disease 0.00–0.40 Severe peripheral arterial Right-arm Left-arm systolic pressure systolic pressure Right-ankle Left-ankle systolic pressure systolic pressure Figure 1. Measurement of the Ankle–Brachial Index (ABI).
Systolic blood pressure is measured by Doppler ultrasonography in each arm and in the dorsalis pedis (DP) and posterior tibial (PT)arteries in each ankle. The higher of the two arm pressures is selected, as is the higher of the two pressures in each ankle. Theright and left ankle–brachial index values are determined by dividing the higher ankle pressure in each leg by the higher arm pres-sure.16 The ranges of the ankle–brachial index values are shown, with a ratio greater than 1.30 suggesting a noncompressible, cal-cified vessel. In this condition, the true pressure at that location cannot be obtained, and additional tests are required to diagnoseperipheral arterial disease. Patients with claudication typically have ankle–brachial index values ranging from 0.41 to 0.90, and thosewith critical leg ischemia have values of 0.40 or less.
lowering therapy reduced disease progression, as meas-
then randomly assigned to placebo or colestipol plus
ured by angiography, and the severity of claudication.
niacin. Lipid-lowering therapy was associated with sta-
Several trials have evaluated the effects of lipid-low-
bilization or regression of femoral atherosclerosis.37
ering therapy on atherosclerosis in the peripheral
The St. Thomas trial, in which 25 men were treated
vessels. In the Cholesterol Lowering Atherosclerosis
with diet, cholestyramine, nicotinic acid, or clofibrate
Study, 188 men with evidence of both coronary and
for an average of 19 months, demonstrated a benefi-
peripheral arterial disease were treated with diet and
cial effect of therapy on femoral atherosclerosis.38 In
1610 · N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
Age »70 yearsLeg pain with exertionAbnormal results on vascular
Figure 2. Evaluation of Patients in Whom Peripheral Arterial Disease Is Suspected.
Patients should be evaluated for peripheral arterial disease if they are at increased risk because of their age or the presence ofatherosclerotic risk factors, have leg pain on exertion, or have distal limb ulceration for which the history and examination do notprovide an obvious explanation. Additional vascular studies can be performed in patients with an ankle–brachial index value above1.30, including pulse-volume recording, measurement of pressure in the first toe, or duplex ultrasonographic imaging of the pe-ripheral vessels, to determine whether peripheral arterial disease is present. Patients with leg pain on exertion who have ankle–brachial index values of 0.91 to 1.30 should be considered for an exercise test. An ankle–brachial index value that is over 0.90 atrest but decreases by 20 percent after exercise is diagnostic of peripheral arterial disease.16 If the initial ankle–brachial index valueis 0.90 or less at rest, the patient probably has peripheral arterial disease, and no additional tests are necessary.
contrast, the Probucol Quantitative Regression Swed-
duction in serum Lp(a) lipoprotein concentrations
ish Trial evaluated 303 patients with peripheral arterial
in patients receiving combined therapy, as compared
disease who were treated with diet and cholestyramine
with a 15 percent increase in patients receiving simva-
and then randomly assigned to receive probucol or
statin alone (P<0.001). Peripheral arterial end points
placebo for three years.39 This study found no ben-
were assessed with duplex ultrasonographic imaging
eficial effect of probucol (a drug that lowers serum
of the femoral and tibial vessels. At the end of the
low-density lipoprotein [LDL] and high-density lip-
study, the number of patients in the simvastatin-only
oprotein [HDL] cholesterol concentrations and has
group with hemodynamically important new stenoses
antioxidant properties) on femoral atherosclerosis or
in their peripheral vessels had increased from 6 to
13, as compared with a decrease from 9 to 7 patients
In a recent study of plasma apheresis to reduce se-
in the simvastatin-plus-apheresis group (P=0.002).
rum Lp(a) lipoprotein concentrations, 42 patients
Although apheresis is not a practical means of treat-
with coronary artery disease were randomly assigned
ing hyperlipidemia, this study suggests that high se-
to simvastatin plus apheresis or simvastatin alone and
rum Lp(a) lipoprotein concentrations are important
followed for two years.40 There was a 19 percent re-
in the development of peripheral arterial disease.
N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org · 1611
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Treadmill MWD and PFWDSF-36 and WIQ questionnaires
Glycosylated hemoglobin <7.0%Blood pressure <130/85 mm HgAngiotensin-converting–
Hemodynamic localizationDuplex ultrasonographyMagnetic resonance angiographyConventional angiography
Figure 3. Evaluation and Treatment of Patients with Proved Peripheral Arterial Disease.
All patients with peripheral arterial disease, regardless of the severity of symptoms, should undergo risk-factor modification toachieve the listed treatment goals and should receive antiplatelet therapy with aspirin or clopidogrel. Angiotensin-converting–enzyme inhibitors may be considered because of the potential for prevention of ischemic events that is independent of blood-pres-sure lowering.
A treadmill test to define the maximal walking distance (MWD) and the pain-free walking distance (PFWD) can provide an objectiveassessment of the severity of claudication and the response to therapy. The functional limitations of claudication and response totherapy can also be quantified by the physical-function scales of the non–disease-specific Medical Outcomes Short Form 36 ques-tionnaire (SF-36) and the disease-specific Walking Impairment Questionnaire (WIQ). Treatment of claudication should begin withexercise therapy or drugs such as cilostazol. In patients whose condition does not improve and who remain disabled, or who haveworsening symptoms, the location of the occlusive lesions should be determined to plan endovascular or surgical intervention.
Noninvasive localization can be performed with hemodynamic tests, such as segmental-limb-pressure and pulse-volume recording. Duplex ultrasonographic imaging and magnetic resonance angiography both have high sensitivity and specificity for the localiza-tion of lesions (with magnetic resonance angiography having the higher sensitivity), but conventional angiography is still requiredin most patients before surgery or angioplasty. Patients with critical leg ischemia typically have ankle–brachial index values of lessthan 0.40 and should initially be considered for localization of their occlusive disease in anticipation of the need for revasculariza-tion. LDL denotes low-density lipoprotein.
Two studies evaluated the effects of lipid-lowering
control group. In a subgroup of patients treated with
therapy on clinical end points in the leg. The Program
simvastatin in the Scandinavian Simvastatin Survival
on the Surgical Control of the Hyperlipidemias was
Study, the relative risk of new claudication or worsen-
a randomized trial of ileal-bypass surgery for the treat-
ing of preexisting claudication was 0.6 (95 percent
ment of hyperlipidemia in 838 patients.41 After five
confidence interval, 0.4 to 0.9; absolute risk reduction,
years, the relative risk of an abnormal ankle–brachial
1.3 percentage points), as compared with patients ran-
index value was 0.6 (95 percent confidence interval,
0.4 to 0.9; absolute risk reduction, 15 percentage
In summary, lipid-lowering therapy has benefit in
points; P<0.01), and the relative risk of claudication
patients with peripheral arterial disease, who often
or limb-threatening ischemia was 0.7 (95 percent con-
have coexisting coronary and cerebral arterial disease.
fidence interval, 0.2 to 0.9; absolute risk reduction,
The current recommendation for patients with periph-
7 percentage points; P<0.01), as compared with the
eral arterial disease is to achieve a serum LDL cho-
1612 · N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
lesterol concentration of less than 100 mg per deci-
The use of angiotensin-converting–enzyme inhib-
liter (2.6 mmol per liter) and a serum triglyceride
itors in patients with peripheral arterial disease may
concentration of less than 150 mg per deciliter (1.7
confer protection against cardiovascular events beyond
mmol per liter).43 A statin should be given as initial
that expected from blood-pressure lowering. In the
therapy, but niacin is an important drug because it
Heart Outcomes Prevention Evaluation Study, 4051
increases serum HDL concentrations and lowers se-
of the 9297 patients (44 percent) had evidence of
rum triglyceride concentrations without worsening
peripheral arterial disease (ankle–brachial index val-
ues of <0.90).52 In the entire study population, theprimary end point of death from vascular causes,
Treatment of Diabetes Mellitus
nonfatal myocardial infarction, or stroke occurred in
Intensive control of blood glucose prevents the mi-
17.7 percent of the placebo group, as compared with
crovascular complications of diabetes, but its effect on
14.1 percent of the ramipril group. The efficacy of
macrovascular complications is less certain. The Di-
ramipril did not differ significantly between patients
abetes Control and Complications Trial compared in-
with peripheral arterial disease and those without it
tensive and conventional insulin therapy in 1441 pa-
(Fig. 4). This study not only underscores the impor-
tients with type 1 diabetes. Intensive therapy was
tance of including patients with peripheral arterial
associated with a trend toward a reduction in cardio-
disease in trials of the secondary prevention of car-
vascular events (P=0.08) but had no effect on the
diovascular disease, but also suggests that angioten-
risk of peripheral arterial disease.45 The results were
sin-converting–enzyme inhibitors reduce the risk of
similar in 3867 patients with type 2 diabetes in the
United Kingdom Prospective Diabetes Study, whichcompared intensive drug treatment using sulfonylu-
Additional Approaches to Risk Modification
rea or insulin with dietary therapy. Intensive drug ther-
A high serum homocysteine concentration is an
apy was associated with a trend toward a reduction
independent risk factor for peripheral arterial disease
in myocardial infarction (P=0.05) but had no effect
and also increases the risk of death from cardiovas-
on the risk of death or amputation due to peripheral
cular causes.20 Homocysteine facilitates the oxidation
arterial disease (relative risk 0.6; 95 percent confidence
of LDL cholesterol. Furthermore, by causing the for-
interval, 0.4 to 1.2).46 These data suggest that inten-
mation of reactive oxygen species, homocysteine can
sive blood glucose control in patients with either
promote endothelial dysfunction and the proliferation
type 1 or type 2 diabetes may not favorably affect
of vascular smooth-muscle cells, leading to accelera-
tion of atherosclerosis.53 The causes of high serum ho-mocysteine concentrations include genetic defects in
Treatment of Hypertension
homocysteine metabolism, alterations in vitamin B12
Hypertension is a major risk factor for peripheral
metabolism, and dietary folate deficiency. Supplement-
arterial disease (as recognized by the Joint National
ing the diet with B vitamins and fortification of food
Committee22), but data are not available to clarify
with folate lower serum homocysteine concentra-
whether treatment will alter the progression of the dis-
tions.54 Despite the ease of therapy with vitamin sup-
plements, there are no clinical trials demonstrating
Beta-adrenergic–antagonist drugs have been
that reducing serum homocysteine concentration is
thought to have unfavorable effects on symptoms in
beneficial in patients with peripheral arterial disease.
patients with peripheral arterial disease.22 This con-
Estrogen therapy reduces several cardiovascular risk
cern arose from several early case reports of worsen-
factors in postmenopausal women. In a population-
ing claudication and decreases in blood flow in the
based study of 2196 women who had undergone nat-
legs in patients taking these drugs.47 In one study,
ural menopause, estrogen treatment for one year or
either atenolol or the calcium-channel–blocking drug
more was associated with a decrease in the incidence
nifedipine, given alone, did not adversely affect skin
of peripheral arterial disease, defined by an ankle–bra-
temperature in the extremities or maximal treadmill
chial index value of <0.90 (odds ratio, 0.5; 95 per-
walking distance, but the combination of the two
cent confidence interval, 0.2 to 0.8).55 The Heart and
drugs reduced maximal treadmill walking distance by
Estrogen/Progestin Replacement Study evaluated the
9 percent.48 In other studies, both selective and non-
effects of estrogen therapy in 2763 postmenopausal
selective beta-adrenergic–antagonist drugs had no ad-
women with coronary artery disease.56 The incidence
verse effects on the peripheral circulation in patients
of peripheral arterial events (defined as aortic or ca-
with peripheral arterial disease.49 A meta-analysis
rotid surgery or revascularization or amputation of the
and a critical review of these studies concluded that
foot or leg) was unaffected by therapy. In addition,
beta-adrenergic antagonists are safe in patients with
estrogen therapy has been associated with reduced
peripheral arterial disease, except in the most severe-
graft patency in women undergoing femoropopliteal
ly affected patients, in whom the drugs should be
bypass surgery, possibly as a result of the prothrom-
botic effects of the therapy.57 Thus, at present, estro-
N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org · 1613
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Figure 4. Results of Ramipril Therapy in Patients with and Patients without Peripheral Arterial Disease from the Heart Outcomes Prevention Evaluation Study.
The rate of the composite outcome of death from vascular causes, nonfatal myocardial infarction, and stroke was re-duced in patients treated with ramipril; the outcomes did not differ significantly between patients with and patientswithout peripheral arterial disease.52 Horizontal bars denote 95 percent confidence intervals. In the graph, values belowunity favor ramipril treatment.
gen has no role in the treatment of peripheral arte-
who had received peripheral arterial grafts or had
rial disease in postmenopausal women; however, the
undergone peripheral angioplasty. The interpretation
presence of peripheral arterial disease is not a con-
of these results has varied. The American College of
traindication to estrogen therapy in women with in-
Chest Physicians recommends aspirin at doses of 81
to 325 mg per day for patients with peripheral arte-rial disease.59 In contrast, a Food and Drug Admin-
Antiplatelet-Drug Therapy
istration (FDA) expert panel found insufficient evi-
In patients with cardiovascular disease, antiplatelet
dence to approve the labeling of aspirin as indicated
drugs reduce the risks of nonfatal myocardial infarc-
for patients with peripheral arterial disease.60
tion, ischemic stroke, and death from vascular causes.
Despite the lack of a statistically significant effect
These conclusions are based primarily on meta-analy-
of aspirin in reducing the overall risk of ischemic
ses of studies of antiplatelet-drug therapy (primarily
events in patients with peripheral arterial disease, as-
aspirin) conducted by the Antiplatelet Trialists’ Col-
pirin may favorably affect the peripheral circulation.
laboration, which included 102,459 patients who had
For example, in the Physicians’ Health Study, a pri-
clinical evidence of cardiovascular disease (acute or
mary-prevention trial, aspirin reduced the subsequent
prior myocardial infarction, ischemic stroke, or other
need for peripheral arterial surgery.61 The Antiplate-
vascular diseases, including peripheral arterial dis-
let Trialists’ Collaboration found that aspirin therapy
ease).58 The principal conclusion was that antiplate-
significantly improved vascular-graft patency in 3226
let-drug therapy reduced the risk of fatal or nonfatal
patients with peripheral arterial disease who were treat-
cardiovascular events from 11.9 percent in the con-
ed with bypass surgery (with a saphenous-vein or pros-
trol group to 9.5 percent in the treatment group.
thetic graft) or peripheral angioplasty and followed
Thus, aspirin is recommended for secondary disease
for an average of 19 months.62 Overall, there was a
prevention in patients with cardiovascular disease. The
43 percent reduction in the rate of vascular-graft oc-
data supporting the use of antiplatelet drugs in pa-
clusion: 25 percent in the control group as compared
tients with peripheral arterial disease are described
with 16 percent in the aspirin group. All the anti-
platelet regimens contained aspirin. Aspirin alone wasas effective as the combination of aspirin and dipy-
Aspirin
ridamole, sulfinpyrazone, or ticlopidine in preventing
The analysis by the Antiplatelet Trialists’ Collabo-
graft occlusion, and high-dose aspirin (600 to 1500
ration included a subgroup of 3295 patients with
mg per day) was as effective as low-dose aspirin (75 to
claudication. In these patients, the risk of myocardial
infarction, stroke, or death from vascular causes aftera mean of 27 months of follow-up was 9.7 percent
Ticlopidine
in patients who received antiplatelet therapy, as com-
Ticlopidine is a thienopyridine drug that inhibits
pared with 11.8 percent in control patients — a re-
platelet activation by blocking platelet adenosine di-
duction of 18 percent. However, the reduction was
phosphate receptors. In patients with peripheral arteri-
not statistically significant. Similar nonsignificant re-
al disease, ticlopidine was more effective than placebo
sults were obtained in a subgroup of 1928 patients
in reducing the risk of fatal or nonfatal myocardial
1614 · N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
infarction or stroke.63 Ticlopidine may reduce the se-
there was a nonsignificant 19 percent reduction in fa-
verity of claudication and the need for vascular sur-
tal and nonfatal ischemic events in the picotamide
gery.64,65 However, enthusiasm for this drug is tem-
group, as compared with the placebo group.69 No
pered by the substantial risk of thrombocytopenia,
further studies have been performed with this drug.
neutropenia (which occurs in 2.3 percent of treated
Ketanserin is an antagonist of S serotonin receptors
patients), and thrombotic thrombocytopenic purpu-
that has antiplatelet effects. In a large trial of ketanserin
ra (which occurs in 1 in 2000 to 4000 patients),
in 3899 patients with peripheral arterial disease, the
for which extensive hematologic monitoring is re-
mortality rate was slightly, but not significantly, high-
quired.66,67 This concern has led to the development
er in the ketanserin group (perhaps in relation to pro-
of other drugs in the thienopyridine class.
longation of the QT interval), and the drug did notrelieve claudication.70,71
Clopidogrel
In summary, patients with peripheral arterial dis-
Clopidogrel is a thienopyridine drug that has few-
ease have systemic atherosclerosis and are at high risk
er hematologic side effects than ticlopidine. The pri-
for cardiovascular disease and death. Although the
mary data that support the use of clopidogrel were
data are not conclusive, aspirin should be considered
derived from the Clopidogrel versus Aspirin in Pa-
the primary antiplatelet drug for preventing ischemic
tients at Risk of Ischaemic Events (CAPRIE) trial.
events in patients with peripheral arterial disease. As-
This trial compared 75 mg of clopidogrel per day
pirin is also effective in maintaining vascular-graft pa-
with 325 mg of aspirin per day in more than 19,000
tency and may prevent thrombotic complications of
patients with recent myocardial infarction, recent is-
peripheral arterial disease. Clopidogrel has FDA ap-
chemic stroke, or peripheral arterial disease (6452 pa-
proval for the prevention of ischemic events in patients
tients).15 The patients with peripheral arterial disease
with peripheral arterial disease and may be more effec-
either had claudication with an ankle–brachial index
tive than aspirin in these patients.
value of 0.85 or less or a history of claudication withprevious peripheral bypass surgery, angioplasty, or
NONPHARMACOLOGIC THERAPY
amputation. Thus, these patients were symptomatic
FOR CLAUDICATION
and had moderately severe peripheral arterial disease. Goals of Therapy
Clopidogrel was associated with an overall reductionof 8.7 percent in the primary end point of fatal or
Patients with claudication have marked impairment
nonfatal ischemic stroke, fatal or nonfatal myocardial
in exercise performance and overall functional capac-
infarction, or death from other vascular causes (P=
ity. Their peak oxygen consumption measured dur-
0.04) (Fig. 5). This result led to FDA approval of
ing graded treadmill exercise is 50 percent of that in
clopidogrel for the secondary prevention of athero-
age-matched normal subjects, indicating a level of im-
sclerotic events in patients with atherosclerosis, in-
pairment similar to that among patients with New
cluding those with peripheral arterial disease. In the
York Heart Association class III heart failure.72 In
CAPRIE trial, both clopidogrel and aspirin were well
addition, patients with claudication typically report
tolerated. However, a recent report described the oc-
great difficulty in walking short distances, even at a
currence of thrombotic thrombocytopenic purpura
slow speed. Reduced walking capacity is associated
early in the course of treatment with clopidogrel.68
with impairment in the performance of activities of
The estimated risk of thrombotic thrombocytopenic
daily living and in the quality of life.28,73 Improving
purpura is 4 per million patients, a level that does
mobility and improving the quality of life are impor-
not warrant routine hematologic monitoring.
tant treatment goals for patients with peripheral ar-
In the CAPRIE trial, there were differences in the
treatment effect among patients with stroke, myocar-dial infarction, and peripheral arterial disease. In the
Exercise Therapy
6452 patients with peripheral arterial disease, the
The primary nonpharmacologic treatment for clau-
primary end point occurred at an annual rate of 4.9
dication is a formal exercise-training program, as dem-
percent in patients given aspirin and 3.7 percent in
onstrated in over 20 randomized trials (albeit many
patients given clopidogrel, an adjusted risk reduction
with small samples).74 Exercise improves not only max-
of 23.8 percent. This treatment effect was greater than
imal treadmill walking distance, but also the quality
that in patients with myocardial infarction or stroke,
of life and community-based functional capacity (i.e.,
but the differences could also have occurred by chance
the ability to walk at defined speeds and for defined
distances).75 A rigorous exercise-training program maybe as beneficial as bypass surgery and may be more
Other Antiplatelet Drugs
beneficial than angioplasty.76,77 A meta-analysis of ran-
Picotamide inhibits thromboxane A synthase and
domized trials found that exercise training increased
blocks thromboxane A receptors. In an 18-month
maximal treadmill walking distance by 179 m (95 per-
trial in 2304 patients with peripheral arterial disease,
cent confidence interval, 60 to 298).31 This degree of
N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org · 1615
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
DRUG THERAPY FOR CLAUDICATION Vasodilator Drugs
Vasodilator drugs, such as papaverine, were the first
medications studied for the treatment of claudication,
but several controlled trials have found no evidenceof clinical efficacy of drugs of this class.83 There are
several pathophysiologic explanations for this finding.
During exercise, the portion of a resistance vessel lo-
cated distally to a stenosis or occlusion dilates in re-
sponse to ischemia. Vasodilators do not affect these
vessels, whose dilation is due to endogenous factors,but they may decrease resistance in other vessels, lead-
ing to a “steal” of blood flow away from the under-
perfused muscle. Vasodilators can also lower systemic
pressure, leading to a reduction in perfusion pressure. Thus, current data do not support the use of vasodi-
Figure 5. Results of the Clopidogrel versus Aspirin in Patients at Risk of Ischaemic Events (CAPRIE) Trial.
In the subgroup of patients with peripheral arterial disease, theprimary end point of fatal or nonfatal myocardial infarction, fa-
Pentoxifylline
tal or nonfatal stroke, or death from other vascular causes oc-
Pentoxifylline is a methylxanthine derivative that
curred at an annual rate of 4.9 percent in those taking aspirin
improves the deformability of red cells and white cells,
and 3.7 percent in those taking clopidogrel, a reduction of 23.8percent. This reduction was greater than that in the subgroups
lowers plasma fibrinogen concentrations, and has an-
of patients with myocardial infarction or stroke.15 Horizontal
tiplatelet effects.84 The drug was approved in 1984 for
bars denote 95 percent confidence intervals.
the treatment of claudication. In one of the first ran-domized trials, pentoxifylline increased maximal tread-mill walking distance by 12 percent as compared withplacebo, but there was no difference between the twogroups in the increase in maximal treadmill walkingdistance as compared with base-line values (Table 3).85
improvement should translate into longer walking dis-
Another study found a nonsignificant increase of 21
percent in maximal treadmill walking distance in pa-
Although exercise therapy is clearly effective, it has
tients treated with pentoxifylline as compared with
several limitations. The best results require a motivat-
placebo.86 Similarly, in a recent study pentoxifylline
ed patient in a supervised setting, typically modeled
was no more effective than placebo in increasing max-
after cardiac rehabilitation.78 However, supervised ex-
imal treadmill walking distance or functional status as
ercise-training programs are not covered by medical
assessed by questionnaires.87 A meta-analysis of the
insurance, which prevents their widespread use. Ex-
pentoxifylline studies found a net benefit of 44 m in
ercise training must also be maintained on a regular
the maximal distance walked on a treadmill (95 per-
basis, or the benefits will be lost. Thus, although ex-
cent confidence interval, 14 to 74).31 This and anoth-
ercise is recommended as the initial treatment for pa-
er meta-analysis and two systematic reviews of pentox-
tients with claudication (Fig. 3), lack of availability and
ifylline concluded that the drug may have a small effect
insurance coverage limit the overall effectiveness of
on walking ability, but that the data are insufficient to
Several studies have examined the mechanisms by
which exercise training exerts its benefits. Exercise
Cilostazol
training is not associated with substantial changes in
Cilostazol was approved in 1999 by the FDA for
blood flow to the legs, and the changes that occur do
the treatment of claudication. The primary action of
not predict the clinical response.79 Despite the absence
cilostazol is to inhibit phosphodiesterase type 3, there-
of a hemodynamic effect, exercise training improves
by increasing intracellular concentrations of cyclic
oxygen extraction in the legs.80 The intermediary me-
AMP. Cilostazol undergoes extensive hepatic me-
tabolism of skeletal muscle is also favorably affected
tabolism by the 3A4 isoform of cytochrome P450
by training, as evidenced by an improvement in mus-
(CYP3A4) and to a lesser extent by the 2C19 and
cle carnitine metabolism.81 Finally, alterations in gait
1A2 isoforms. Although the drug does not inhibit
and walking efficiency may contribute to the training
the cytochrome CYP450 enzyme system, other drugs
response. At submaximal workloads, training results
that inhibit CYP3A4 may increase serum cilostazol
in a decrease in oxygen consumption and thus im-
concentrations.103 Cilostazol inhibits platelet aggrega-
tion, the formation of arterial thrombi, and vascular
1616 · N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
smooth-muscle proliferation and causes vasodilata-
perior to both placebo and pentoxifylline.87 In three
tion.104-106 However, as discussed above, vasodilator
of the trials, cilostazol also improved several aspects
and antiplatelet drugs do not improve claudication-
of physical functioning and the quality of life, as as-
limited exercise performance, and therefore the mech-
sessed by questionnaires.89-91 The drug also causes
anism of effect of cilostazol in peripheral arterial dis-
small increases in ankle–brachial index values and rais-
es serum HDL cholesterol concentrations.90
Type 3 phosphodiesterase inhibitors such as milri-
The predominant side effect of cilostazol is head-
none were developed as inotropic agents for the treat-
ache, which affects 34 percent of patients taking 100
ment of heart failure. In patients with chronic heart
mg twice daily, as compared with 14 percent of pa-
failure, milrinone treatment was associated with an in-
tients taking placebo (data presented to the FDA Car-
crease in mortality.107 In comparison with milrinone,
diovascular and Renal Drugs Advisory Committee
cilostazol has fewer cardiac inotropic effects but equiv-
on July 9, 1998). In addition, transient diarrhea, pal-
alent vasodilating and platelet-inhibiting properties.108
pitations, and dizziness have been described. Cilosta-
Four randomized, placebo-controlled trials of cil-
zol can be administered with aspirin, but there are
ostazol enrolling 1534 patients with claudication have
no data on the safety of coadministration of cilosta-
been published (Table 3 and Fig. 6).87,89-91 In all four
zol with clopidogrel. Because of concern about the
trials, cilostazol (100 mg twice daily) improved both
risk of death with this class of drugs, data from more
pain-free and maximal treadmill walking distance, as
than 2000 patients who were followed for up to six
compared with placebo. Cilostazol (50 mg twice dai-
months were presented to the FDA. Death from car-
ly) also increased maximal treadmill walking distance.91
diovascular causes occurred in 0.6 percent of cilosta-
In one trial, cilostazol (100 mg twice daily) was su-
zol-treated patients and 0.5 percent of placebo-treat-
TABLE 3. DRUG THERAPIES FOR PATIENTS WITH CLAUDICATION. RESULTS OF FUNCTIONAL DRUG AND STUDY SUBJECTS OF THERAPY VALUE† ASSESSMENT‡
*Net MWD is the net improvement in maximal treadmill walking distance with the drug as compared
†NS indicates a result reported as not significant but with no P value provided.
‡Functional assessment involved the use of questionnaires to assess the effect of treatment on the
quality of life. ND denotes not done.
N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org · 1617
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
ed patients. Myocardial infarction occurred in 1.5
tive than levocarnitine in improving maximal treadmill
percent of cilostazol-treated patients and 1.1 percent
walking distance.113 In two multicenter trials enroll-
of placebo-treated patients. Because of the experience
ing 730 patients, the pain-free and maximal treadmill
with milrinone, the cilostazol label includes a black-
walking distance improved more in patients receiving
box warning that cilostazol should not be given to pa-
propionyl levocarnitine than in those receiving pla-
tients with claudication who also have heart failure.
cebo.95,96 The drug also improved the quality of lifemore than placebo and had fewer side effects.96 Pro-
Naftidrofuryl
pionyl levocarnitine has not been approved for use
Naftidrofuryl has been available for several decades
in Europe for treating claudication. Several mecha-nisms of action have been proposed, including antag-
Prostaglandins
onism of 5-hydroxytryptamine receptors. A critical
Prostaglandins have been evaluated primarily for the
review of five placebo-controlled trials concluded that
treatment of patients with critical leg ischemia. The
naftidrofuryl improved pain-free treadmill walking
primary end points of these trials were relief of ische-
distance, but not maximal walking distance (Table 3),
mic pain, healing of ischemic ulcers, and reduction in
and was associated with fewer cardiovascular events
the rate of amputation.114,115 Fewer studies have been
than placebo.109 This drug is not available in the Unit-
performed in patients with claudication. A study of
90 such patients found that parenteral administrationof prostaglandin E in a formulation of lipid micro-
Levocarnitine and Propionyl Levocarnitine
spheres improved maximal treadmill walking distance
In patients with peripheral arterial disease, meta-
and quality of life.97 Oral analogues of prostaglandins
bolic abnormalities develop in the skeletal muscles of
have not been as well studied. A small trial found
the lower extremities.110 These abnormalities include
that beraprost was moderately efficacious, but at high-
impairment of the activity of the mitochondrial elec-
er doses it had substantial side effects, such as head-
tron-transport chain in the ischemic muscles and ac-
ache, flushing, and gastrointestinal intolerance.99 A re-
cumulation of intermediates of oxidative metabolism
cent study found that beraprost had positive effects
(acylcarnitines).111,112 Exercise performance is most im-
on maximal treadmill walking distance and the qual-
paired in patients with the greatest accumulation of
ity of life (Table 3) and reduced the rate of critical
acylcarnitines in muscle. Thus, claudication is caused
cardiovascular events.100 The use of prostaglandins in
not just by reduced blood flow, but also by alterations
patients with peripheral arterial disease needs fur-
Levocarnitine and propionyl levocarnitine may im-
prove metabolism and exercise performance of ische-
Other Drugs
mic muscles. Levocarnitine, 2 g twice daily, improved
Treatment with chelation, vitamin E, or testoster-
maximal treadmill walking distance, but propionyl le-
one has no effect on claudication.116-118 Treatments that
vocarnitine (an acyl form of carnitine) was more effec-
have had promising results in preliminary studies in-
Figure 6. Results of Four Randomized, Placebo-Controlled Trials of Cilostazol for the Treatment of Clau- dication.
The data are shown as the geometric mean ratios of the maximal treadmill walking distance (on thehorizontal axis) and 95 percent confidence intervals for cilostazol as compared with placebo.87,89-91
1618 · N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
clude buflomedil, Ginkgo biloba, inositol niacinate,
3. Fowkes FGR , Housley E, Cawood EHH, Macintyre CCA, Ruckley CV,
defibrotide, verapamil, anticoagulants, and arginine,
Prescott RJ. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Ep-
but none of these have been evaluated in large clin-
4. Newman AB, Sutton-Tyrrell K, Rutan GH, Locher J, Kuller LH. Lower extremity arterial disease in elderly subjects with systolic hypertension. J Clin Epidemiol 1991;44:15-20. CONCLUSIONS 5. Newman AB, Siscovick DS, Manolio TA, et al. Ankle-arm index as a
Peripheral arterial disease is a highly prevalent man-
marker of atherosclerosis in the Cardiovascular Health Study. Circulation 1993;88:837-45.
ifestation of atherosclerosis that is associated with a
6. Zheng ZJ, Sharrett AR , Chambless LE, et al. Associations of ankle-bra-
substantial risk of illness and death and a marked re-
chial index with clinical coronary heart disease, stroke and preclinical ca-
duction in ambulatory capacity and quality of life.
rotid and popliteal atherosclerosis: the Atherosclerosis Risk in Communi-ties (ARIC) Study. Atherosclerosis 1997;131:115-25.
Unfortunately, peripheral arterial disease is under-
7. Criqui MH, Fronek A, Barrett-Connor E, Klauber MR , Gabriel S,
treated with regard to risk-factor modification, use
Goodman D. The prevalence of peripheral arterial disease in a defined pop-ulation. Circulation 1985;71:510-5.
of antiplatelet drugs, and treatment of symptoms. 8. Hiatt WR , Hoag S, Hamman RF. Effect of diagnostic criteria on the
Clinical trials specifically directed to patients with
prevalence of peripheral arterial disease: the San Luis Valley Diabetes
peripheral arterial disease are needed to address the
Study. Circulation 1995;91:1472-9. 9. Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10
benefits of the treatment of hyperlipidemia, diabetes,
years in patients with peripheral arterial disease. N Engl J Med 1992;326:
hyperhomocysteinemia, and other prevalent risk fac-
tors. Despite these limitations, patients with periph-
10. Vogt MT, Cauley JA, Newman AB, Kuller LH, Hulley SB. Decreased ankle/arm blood pressure index and mortality in elderly women. JAMA
eral arterial disease should be considered candidates
for secondary-prevention strategies, just as are patients
11. Leng GC, Lee AJ, Fowkes FG, et al. Incidence, natural history and car- diovascular events in symptomatic and asymptomatic peripheral arterial dis-
with coronary artery disease. Angiotensin-convert-
ease in the general population. Int J Epidemiol 1996;25:1172-81.
ing–enzyme inhibitors may decrease the risk of is-
12. Newman AB, Shemanski L, Manolio TA, et al. Ankle-arm index as a
chemic events. However, antiplatelet drugs are effec-
predictor of cardiovascular disease and mortality in the Cardiovascular Health Study. Arterioscler Thromb Vasc Biol 1999;19:538-45.
tive at reducing the risk of fatal and nonfatal ischemic
13. Newman AB, Tyrrell KS, Kuller LH. Mortality over four years in
events in patients with peripheral arterial disease. The
SHEP participants with a low ankle-arm index. J Am Geriatr Soc 1997;45:
data supporting the use of antiplatelet drugs are
1472-8. 14. Kornitzer M, Dramaix M, Sobolski J, Degre S, De Backer G. Ankle/
stronger than those supporting the use of angioten-
arm pressure index in asymptomatic middle-aged males: an independent
sin-converting–enzyme inhibitors. Aspirin should be
predictor of ten-year coronary heart disease mortality. Angiology 1995;46:211-9.
considered in all patients, with clopidogrel an alter-
15. CAPRIE Steering Committee. A randomised, blinded, trial of clopid-
native (and potentially more effective) drug.
ogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lan-
Medical therapies to treat the symptoms of clau-
cet 1996;348:1329-39. 16. Orchard TJ, Strandness DE. Assessment of peripheral vascular disease
dication and limited mobility are now well established.
in diabetes: report and recommendations of an international workshop
A supervised walking-based exercise program should
sponsored by the American Diabetes Association and the American Heart
be considered first for all patients because of the low
Association September 18-20, 1992, New Orleans, Louisiana. Circulation 1993;88:819-28.
risk and the likelihood of marked improvement in
17. McKenna M, Wolfson S, Kuller L. The ratio of ankle and arm arterial
functional capacity that is associated with exercise.
pressure as an independent predictor of mortality. Atherosclerosis 1991;87:119-28.
Drugs that improve functional status are also avail-
18. Vogt MT, McKenna M, Anderson SJ, Wolfson SK, Kuller LH. The re-
able. Pentoxifylline has limited efficacy, but cilosta-
lationship between ankle-arm index and mortality in older men and wom-
zol improves both pain-free and maximal treadmill
en. J Am Geriatr Soc 1993;41:523-30. 19. Dormandy JA, Heeck L, Vig S. The fate of patients with critical leg
walking distance and the quality of life. Several other
ischemia. Semin Vasc Surg 1999;12:142-7.
compounds, such as propionyl levocarnitine, are un-
20. Graham IM, Daly LE, Refsum HM, et al. Plasma homocysteine as a
der investigation for the treatment of claudication
risk factor for vascular disease: the European Concerted Action Project. JAMA 1997;277:1775-81. 21. Summary of the second report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). JAMA
Dr. Hiatt has received grant support from Bristol-Myers Squibb–Sanofi
Synthelabo, Cooke Pharma, Dupont Pharmaceuticals, Otsuka America
22. The sixth report of the Joint National Committee on prevention, de-
Pharmaceuticals–Pharmacia, Parke-Davis Pharmaceuticals, Sigma-Tau Phar-
tection, evaluation, and treatment of high blood pressure. Arch Intern Med
maceuticals, and United Therapeutics. He has served on the speakers’ bu-
1997;157:2413-46. [Erratum, Arch Intern Med 1998;158:573.]
reaus and steering committees of several of these corporations and has also
23. McDermott MM, Mehta S, Ahn H, Greenland P. Atherosclerotic risk
served on steering committees for Ajinomoto Pharmaceuticals, Berlex Lab-
factors are less intensively treated in patients with peripheral arterial disease
oratories, Eli Lilly, and Welfide Corporation.
than in patients with coronary artery disease. J Gen Intern Med 1997;12:209-15. I am indebted to Ms. Lisa Cox for assistance in the preparation of24. Clark AL, Byrne JC, Nasser A, McGroarty E, Kennedy JA. Cholester- the manuscript, and to Dr. Eric Brass for critical review.
ol in peripheral vascular disease — a suitable case for treatment? QJM 1999;92:219-22. REFERENCES 25. Rose GA, Blackburn H. Cardiovascular survey methods. World Health Organization monograph series. No. 56. Geneva: World Health Organiza- 1. Schroll M, Munck O. Estimation of peripheral arteriosclerotic disease
by ankle blood pressure measurements in a population study of 60-year-
26. Imparato AM, Kim GE, Davidson T, Crowley JG. Intermittent clau-
old men and women. J Chronic Dis 1981;34:261-9.
dication: its natural course. Surgery 1975;78:795-9. 2. Meijer WT, Hoes AW, Rutgers D, Bots ML, Hofman A, Grobbee DE. 27. McDermott MM, Mehta S, Liu K, et al. Leg symptoms, the ankle-
Peripheral arterial disease in the elderly: the Rotterdam Study. Arterioscler
brachial index, and walking ability in patients with peripheral arterial dis-
ease. J Gen Intern Med 1999;14:173-81.
N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org · 1619
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
28. Vogt MT, Cauley JA, Kuller LH, Nevitt MC. Functional status and 55. Westendorp IC, in’t Veld BA, Grobbee DE, et al. Hormone replace-
mobility among elderly women with lower extremity arterial disease: the
ment therapy and peripheral arterial disease: the Rotterdam study. Arch In-
Study of Osteoporotic Fractures. J Am Geriatr Soc 1994;42:923-9. 29. Dormandy JA, Rutherford RB. Management of peripheral arterial dis- 56. Hsia J, Simon JA, Lin F, et al. Peripheral arterial disease in randomized
ease (PAD). J Vasc Surg 2000;31:S1-S296.
trial of estrogen with progestin in women with coronary heart disease: the
30. Quick CRG, Cotton LT. The measured effect of stopping smoking on
Heart and Estrogen/Progestin Replacement Study. Circulation 2000;102:
intermittent claudication. Br J Surg 1982;69:Suppl:S24-S26. 31. Girolami B, Bernardi E, Prins MH, et al. Treatment of intermittent 57. Timaran CH, Stevens SL, Grandas OH, Piercy KT, Freeman MB,
claudication with physical training, smoking cessation, pentoxifylline, or
Goldman MH. Influence of hormone replacement therapy on graft paten-
nafronyl: a meta-analysis. Arch Intern Med 1999;159:337-45.
cy after femoropopliteal bypass grafting. J Vasc Surg 2000;32:506-18. 32. Jorenby DE, Leischow SJ, Nides MA, et al. A controlled trial of sus- 58. Collaborative overview of randomised trials of antiplatelet therapy.
tained-release bupropion, a nicotine patch, or both for smoking cessation.
I. Prevention of death, myocardial infarction, and stroke by prolonged anti-
platelet therapy in various categories of patients. BMJ 1994;308:81-106.
33. LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary
disease: a meta-analysis of randomized controlled trials. JAMA 1999;282:
59. Sachdev GP, Ohlrogge KD, Johnson CL. Review of the Fifth Ameri-
can College of Chest Physicians Consensus Conference on Antithrombotic
34. Khan F, Litchfield SJ, Belch JJ. Cutaneous microvascular responses are
Therapy: outpatient management for adults. Am J Health Syst Pharm
improved after cholesterol-lowering in patients with peripheral arterial dis-
ease and hypercholesterolaemia. Adv Exp Med Biol 1997;428:49-54. 60. Food and Drug Administration. Internal analgesic, antipyretic, and 35. Kirk G, McLaren M, Muir AH, Stonebridge PA, Belch JJ. Decrease in
antirheumatic drug products for over-the-counter human use: final rule for
P-selectin levels in patients with hypercholesterolaemia and peripheral arte-
professional labeling of aspirin, buffered aspirin, and aspirin in combination
rial occlusive disease after lipid-lowering treatment. Vasc Med 1999;4:23-6.
with antacid drug products. Fed Regist 1998;63(205):56802-19. 36. Leng GC, Price JF, Jepson RG. Lipid-lowering for lower limb athero- 61. Goldhaber SZ, Manson JE, Stampfer MJ, et al. Low-dose aspirin and
sclerosis (Cochrane review). In: The Cochrane library. Oxford, England:
subsequent peripheral arterial surgery in the Physicians’ Health Study. Lan-
37. Blankenhorn DH, Azen SP, Crawford DW, et al. Effects of colestipol- 62. Collaborative overview of randomised trials of antiplatelet therapy.
niacin therapy on human femoral atherosclerosis. Circulation 1991;83:438-
II. Maintenance of vascular graft or arterial patency by antiplatelet therapy.
38. Lewis B. Randomised controlled trial of the treatment of hyperlipi- 63. Janzon L, Bergqvist D, Boberg J, et al. Prevention of myocardial infarc-
daemia on progression of atherosclerosis. Acta Med Scand Suppl 1985;701:
tion and stroke in patients with intermittent claudication: effects of ticlopi-
dine: results from STIMS, the Swedish Ticlopidine Multicenter Study. J In-
39. Walldius G, Erikson U, Olsson AG, et al. The effect of probucol on
tern Med 1990;227:301-8. [Erratum, J Intern Med 1990;228:659.]
femoral atherosclerosis: the Probucol Quantitative Regression Swedish Tri-
64. Balsano F, Coccheri S, Libretti A, et al. Ticlopidine in the treatment
al (PQRST). Am J Cardiol 1994;74:875-83.
of intermittent claudication: a 21-month double-blind trial. J Lab Clin
40. Kroon AA, van Asten WN, Stalenhoef AF. Effect of apheresis of low-
density lipoprotein on peripheral vascular disease in hypercholesterolemic
65. Bergqvist D, Almgren B, Dickinson JP. Reduction of requirement for
patients with coronary artery disease. Ann Intern Med 1996;125:945-54.
leg vascular surgery during long-term treatment of claudicant patients with
41. Buchwald H, Bourdages HR , Campos CT, Nguyen P, Williams SE,
ticlopidine: results from the Swedish Ticlopidine Multicentre Study
Boen JR. Impact of cholesterol reduction on peripheral arterial disease in
(STIMS). Eur J Vasc Endovasc Surg 1995;10:69-76.
the Program on the Surgical Control of the Hyperlipidemias (POSCH).
66. Bennett CL, Weinberg PD, Rozenberg-Ben-Dror K, Yarnold PR ,
Kwaan HC, Green D. Thrombotic thrombocytopenic purpura associated
42. Pedersen TR , Kjekshus J, Pyorala K, et al. Effect of simvastatin on is-
with ticlopidine: a review of 60 cases. Ann Intern Med 1998;128:541-4.
chemic signs and symptoms in the Scandinavian Simvastatin Survival Study
67. Hankey GJ, Sudlow CL, Dunbabin DW. Thienopyridine derivatives
(ticlopidine, clopidogrel) versus aspirin for preventing stroke and other se-
43. Ansell BJ, Watson KE, Fogelman AM. An evidence-based assessment
rious vascular events in high vascular risk patients. Cochrane Database Syst
of NCEP Adult Treatment Panel II guidelines: National Cholesterol Edu-
cation Program. JAMA 1999;282:2051-7. 68. Bennett CL, Connors JM, Carwile JM, et al. Thrombotic thrombo- 44. Elam MB, Hunninghake DB, Davis KB, et al. Effect of niacin on lipid
cytopenic purpura associated with clopidogrel. N Engl J Med 2000;342:
and lipoprotein levels and glycemic control in patients with diabetes and
peripheral arterial disease: the ADMIT study: a randomized trial. JAMA
69. Balsano F, Violi F. Effect of picotamide on the clinical progression of
peripheral vascular disease: a double-blind placebo-controlled study. Circu-
45. Effect of intensive diabetes management on macrovascular events and
risk factors in the Diabetes Control and Complications Trial. Am J Cardiol
70. Prevention of atherosclerotic complications: controlled trial of ket-
anserin. BMJ 1989;298:424-30. [Erratum, BMJ 1989;298:644.]
46. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glu- 71. Randomized placebo-controlled, double-blind trial of ketanserin in
cose control with sulphonylureas or insulin compared with conventional
claudicants: changes in claudication distance and ankle systolic pressure:
treatment and risk of complications in patients with type 2 diabetes
PACK Claudication Substudy. Circulation 1989;89:1544-8.
(UKPDS 33). Lancet 1998;352:837-53. [Erratum, Lancet 1999;354:602.]
72. Hiatt WR , Nawaz D, Brass EP. Carnitine metabolism during exercise 47. Frohlich ED, Tarazi RC, Dustan HP. Peripheral arterial insufficiency:
in patients with peripheral vascular disease. J Appl Physiol 1987;62:2383-7.
a complication of beta-adrenergic blocking therapy. JAMA 1969;208:2471-2. 73. Khaira HS, Hanger R , Shearman CP. Quality of life in patients with 48. Solomon SA, Ramsay LE, Yeo WW, Parnell L, Morris-Jones W. Beta
intermittent claudication. Eur J Vasc Endovasc Surg 1996;11:65-9.
blockade and intermittent claudication: placebo controlled trial of atenolol
74. Nehler MR , Hiatt WR. Exercise therapy for claudication. Ann Vasc
and nifedipine and their combination. BMJ 1991;303:1100-4. 49. Hiatt WR , Stoll S, Nies AS. Effect of B-adrenergic blockers on the pe- 75. Regensteiner JG, Steiner JF, Hiatt WR. Exercise training improves
ripheral circulation in patients with peripheral vascular disease. Circulation
functional status in patients with peripheral arterial disease. J Vasc Surg
50. Radack K, Deck C. Beta-adrenergic blocker therapy does not worsen 76. Lundgren F, Dahllof A, Lundholm K, Schersten T, Volkmann R. In-
intermittent claudication in subjects with peripheral arterial disease: a meta-
termittent claudication — surgical reconstruction or physical training?
analysis of randomized controlled trials. Arch Intern Med 1991;151:1769-76.
A prospective randomized trial of treatment efficiency. Ann Surg 1989;209:
51. Heintzen MP, Strauer BE. Peripheral vascular effects of beta-blockers. 77. Creasy TS, McMillan PJ, Fletcher EWL, Collin J, Morris PJ. Is percu- 52. The Heart Outcomes Prevention Evaluation Study Investigators. Ef-
taneous transluminal angioplasty better than exercise for claudication? Pre-
fects of an angiotensin-converting–enzyme inhibitor, ramipril, on cardio-
liminary results from a prospective randomised trial. Eur J Vasc Surg 1990;
vascular events in high-risk patients. N Engl J Med 2000;342:145-53.
[Errata, N Engl J Med 2000;342:748, 1376.]
78. Regensteiner JG, Meyer TJ, Krupski WC, Cranford LS, Hiatt WR. 53. Welch GN, Loscalzo J. Homocysteine and atherothrombosis. N Engl
Hospital vs home-based exercise rehabilitation for patients with peripheral
arterial occlusive disease. Angiology 1997;48:291-300. 54. Jacques PF, Selhub J, Bostom AG, Wilson PWF, Rosenberg IH. The 79. Hiatt WR , Regensteiner JG, Hargarten ME, Wolfel EE, Brass EP.
effect of folic acid fortification on plasma folate and total homocysteine
Benefit of exercise conditioning for patients with peripheral arterial disease.
concentrations. N Engl J Med 1999;340:1449-54. 1620 · N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y 80. Zetterquist S. The effect of active training on the nutritive blood flow
teraction of cilostazol with human hepatic cytochrome P450 isoforms.
in exercising ischemic legs. Scand J Clin Lab Invest 1970;25:101-11. 81. Hiatt WR , Regensteiner JG, Wolfel EE, Carry MR , Brass EP. Effect 104. Kohda N, Tani T, Nakayama S, et al. Effect of cilostazol, a phospho-
of exercise training on skeletal muscle histology and metabolism in periph-
diesterase III inhibitor, on experimental thrombosis in the porcine carotid
eral arterial disease. J Appl Physiol 1996;81:780-8. 82. Hiatt WR , Wolfel EE, Meier RH, Regensteiner JG. Superiority of 105. Igawa T, Tani T, Chijiwa T, et al. Potentiation of anti-platelet aggre-
treadmill walking exercise versus strength training for patients with periph-
gating activity of cilostazol with vascular endothelial cells. Thromb Res
eral arterial disease: implications for the mechanism of the training re-
sponse. Circulation 1994;90:1866-74. 106. Tsuchikane E, Fukuhara A, Kobayashi T, et al. Impact of cilostazol 83. Coffman JD. Vasodilator drugs in peripheral vascular disease. N Engl
on restenosis after percutaneous coronary balloon angioplasty. Circulation
84. Samlaska CP, Winfield EA. Pentoxifylline. J Am Acad Dermatol 1994; 107. Packer M, Carver JR, Rodeheffer RJ, et al. Effect of oral milrinone on
mortality in severe chronic heart failure. N Engl J Med 1991;325:1468-75. 85. Porter JM, Cutler BS, Lee BY, et al. Pentoxifylline efficacy in the treat- 108. Cone J, Wang S, Tandon N, et al. Comparison of the effects of cil-
ment of intermittent claudication: multicenter controlled double-blind trial
ostazol and milrinone on intracellular cAMP levels and cellular function in
with objective assessment of chronic occlusive arterial disease patients. Am
platelets and cardiac cells. J Cardiovasc Pharmacol 1999;34:497-504. 109. Lehert P, Comte S, Gamand S, Brown TM. Naftidrofuryl in inter- 86. Lindgarde F, Jelnes R , Bjorkman H, et al. Conservative drug treatment
mittent claudication: a retrospective analysis. J Cardiovasc Pharmacol 1994;
in patients with moderately severe chronic occlusive peripheral arterial dis-
110. Brass EP, Hiatt WR. Acquired skeletal muscle metabolic myopathy in 87. Dawson DL, Cutler BS, Hiatt WR , et al. A comparison of cilostazol
atherosclerotic peripheral arterial disease. Vasc Med 2000;5:55-9.
and pentoxifylline for treating intermittent claudication. Am J Med 2000;
111. Brass EP, Hiatt WR , Gardner AW, Hoppel CL. Decreased NADH
dehydrogenase and ubiquinol-cytochrome c oxidoreductase in peripheral
88. Hood SC, Moher D, Barber GG. Management of intermittent claudi-
arterial disease. Am J Physiol Heart Circ Physiol 2001;280:H603-H609.
cation with pentoxifylline: meta-analysis of randomized controlled trials.
112. Hiatt WR , Wolfel EE, Regensteiner JG, Brass EP. Skeletal muscle
carnitine metabolism in patients with unilateral peripheral arterial disease.
89. Dawson DL, Cutler BS, Meissner MH, Strandness DEJ. Cilostazol has
beneficial effects in treatment of intermittent claudication: results from a
113. Brevetti G, Perna S, Sabba C, et al. Superiority of L-propionylcar-
multicenter, randomized, prospective, double-blind trial. Circulation 1998;
nitine vs L-carnitine in improving walking capacity in patients with periph-
eral vascular disease: an acute, intravenous, double-blind, cross-over study.
90. Money SR , Herd JA, Isaacsohn JL, et al. Effect of cilostazol on walk-
ing distances in patients with intermittent claudication caused by peripheral
114. Norgren L, Alwmark A, Angqvist KA, et al. A stable prostacyclin an-
vascular disease. J Vasc Surg 1998;27:267-74.
alogue (iloprost) in the treatment of ischaemic ulcers of the lower limb:
91. Beebe HG, Dawson DL, Cutler BS, et al. A new pharmacological
a Scandinavian-Polish placebo controlled, randomised multicenter study. Eur
treatment for intermittent claudication: results of a randomized, multi-
center trial. Arch Intern Med 1999;159:2041-50. 115. U.K. Severe Limb Ischaemia Study Group. Treatment of limb threat- 92. Moody AP, al-Khaffaf HS, Lehert P, Harris PL, Charlesworth D. An
ening ischaemia with intravenous iloprost: a randomised double-blind pla-
evaluation of patients with severe intermittent claudication and the effect
cebo controlled study. Eur J Vasc Surg 1991;5:511-6.
of treatment with naftidrofuryl. J Cardiovasc Pharmacol 1994;23:Suppl 3:
116. Ernst E. Chelation therapy for peripheral arterial occlusive disease:
a systematic review. Circulation 1997;96:1031-3. 93. Trubestein G, Bohme H, Heidrich H, et al. Naftidrofuryl in chronic 117. Kleijen J, Mackerras D. Vitamin E for intermittent claudication
arterial disease: results of a controlled multicenter study. Angiology 1984;
(Cochrane review). In: The Cochrane library. Oxford, England: Update
94. Adhoute G, Andreassian B, Boccalon H, et al. Treatment of stage II 118. Price JF, Leng GC. Steroid sex hormones for lower limb atheroscle-
chronic arterial disease of the lower limbs with the serotonergic antagonist
rosis (Cochrane review). In: The Cochrane library. Oxford, England: Up-
naftidrofuryl: results after 6 months of a controlled, multicenter study.
J Cardiovasc Pharmacol 1990;16:Suppl 3:S75-S80. 119. Trubestein G, Balzer K, Bisler H, et al. Buflomedil in arterial occlu- 95. Brevetti G, Perna S, Sabba C, Martone VD, Condorelli M. Propionyl-
sive disease: results of a controlled multicenter study. Angiology 1984;35:
L-carnitine in intermittent claudication: double-blind, placebo-controlled,
dose titration, multicenter study. J Am Coll Cardiol 1995;26:1411-6. 120. Peters H, Kieser M, Holscher U. Demonstration of the efficacy of 96. Brevetti G, Diehm C, Lambert D. European multicenter study on
ginkgo biloba special extract EGb 761 on intermittent claudication —
propionyl-L-carnitine in intermittent claudication. J Am Coll Cardiol
a placebo-controlled, double-blind multicenter trial. Vasa 1998;27:106-10. 121. O’Hara J, Jolly PN, Nicol CG. The therapeutic efficacy of inositol 97. Belch JJF, Bell PRF, Creissen D, et al. Randomized, double-blind, pla-
nicotinate (Hexopal) in intermittent claudication: a controlled trial. Br J
cebo-controlled study evaluating the efficacy and safety of AS-013, a pros-
taglandin E prodrug, in patients with intermittent claudication. Circula-
122. Violi F, Marubini E, Coccheri S, Nenci GG. Improvement of walking
distance by defibrotide in patients with intermittent claudication — results
98. Diehm C, Balzer K, Bisler H, et al. Efficacy of a new prostaglandin
of a randomized, placebo-controlled study (the DICLIS study): Defi-
E1 regimen in outpatients with severe intermittent claudication: results of
brotide Intermittent CLaudication Italian Study. Thromb Haemost 2000;
a multicenter placebo-controlled double-blind trial. J Vasc Surg 1997;25:
123. Bagger JP, Helligsoe P, Randsbaek F, Kimose HH, Jensen BS. Effect 99. Lievre M, Azoulay S, Lion L, Morand S, Girre JP, Boissel JP. A dose-
of verapamil in intermittent claudication: a randomized, double-blind, pla-
effect study of beraprost sodium in intermittent claudication. J Cardiovasc
cebo-controlled, cross-over study after individual dose-response assess-
100. Lievre M, Morand S, Besse B, Fiessinger JN, Boissel JP. Oral bera- 124. Girolami B, Bernardi E, Prins MH, et al. Antithrombotic drugs in
prost sodium, a prostaglandin I(2) analogue, for intermittent claudication:
the primary medical management of intermittent claudication: a meta-
a double-blind, randomized, multicenter controlled trial. Circulation
analysis. Thromb Haemost 1999;81:715-22. 125. Boger RH, Bode-Boger SM, Thiele W, Cruetzig A, Alexander K, 101. Ernst E. Pentoxifylline for intermittent claudication: a critical review.
Frolich JC. Restoring vascular nitric oxide formation by L-arginine im-
proves the symptoms of intermittent claudication in patients with periph-
102. Radack K, Wyderski RJ. Conservative management of intermittent
eral arterial occlusive disease. J Am Coll Cardiol 1998;32:1336-44.
claudication. Ann Intern Med 1990;113:135-46. 103. Abbas R , Chow CP, Browder NJ, et al. In vitro metabolism and in-
Copyright 2001 Massachusetts Medical Society.
N Engl J Med, Vol. 344, No. 21 · May 24, 2001 · www.nejm.org · 1621
Downloaded from www.nejm.org at TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER on April 19, 2010 .
Copyright 2001 Massachusetts Medical Society. All rights reserved.
2nd Balkandiab Meeting Chronic diabetic complications INTRODUCTION (or the status of Diabetes Care) will be presented. Dr Christos Manes In the second half we will discuss with the advisory President of Northern Greece, Diabetes association board the plan of our activities in the future. So it’stime to start. I would like to ask Dr. I. Kalo and Pr. M. On behalf of Northern
Behavior and Presence of Antidepressant Pharmaceuticals and Their DegradatesMethods Research and Development Program, National Water Quality Laboratory,Antidepressants are widely prescribed pharmaceuticals. In 2004, six of the 100most widely dispensed pharmaceuticals were antidepressants, including sertraline(Zoloft), fluoxetine (Prozac), venlafaxine (Effexor), paroxetine (Paxil), citalopram(Cel



 The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Interpretation of ABI
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Interpretation of ABI