Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Jco 17/9
H e a l t h - R e l a t e d Q u a l i t y o f L i f e a n d T a m o x i f e n i n B r e a s t C a n c e r P r e v e n t i o n : A R e p o r t F r o m t h e N a t i o n a l S u r g i c a l A d j u v a n t B r e a s t a n d B o w e l P r o j e c t P - 1 S t u d y
By Richard Day, Patricia A. Ganz, Joseph P. Costantino, Walter M. Cronin, D. Lawrence Wickerham, and Bernard Fisher
Purpose: This is the initial report from the health- the MOS SF-36 summary physical and mental scores. related quality of life (HRQL) component of the National The mean number of symptoms reported was consis- Surgical Adjuvant Breast and Bowel Project Breast Can- tently higher in the tamoxifen group and was associ- cer Prevention Trial. This report provides an overview of ated with vasomotor and gynecologic symptoms. Signifi- HRQL findings, comparing tamoxifen and placebo cant increases were found in the proportion of women groups, and advice to clinicians counseling women on tamoxifen reporting problems of sexual functioning about the use of tamoxifen in a prevention setting. at a definite or serious level, although overall rates of Patients and Methods: This report covers the base- sexual activity remained similar. line and the first 36 months of follow-up data on 11,064 Conclusion: Women need to be informed of the in- women recruited over the first 24 months of the study. creased frequency of vasomotor and gynecologic symp- Findings are presented from the Center for Epidemiologi- toms and problems of sexual functioning associated cal Studies–Depression Scale (CES-D), the Medical Out- with tamoxifen use. Weight gain and depression, two comes Study 36-Item Short Form Health Status Survey clinical problems anecdotally associated with tamoxi- (MOS SF-36) and sexual functioning scale, and a symp- fen treatment, were not increased in frequency in this tom checklist. trial in healthy women, which is good news that also Results: No differences were found between pla- needs to be communicated. cebo and tamoxifen groups for the proportion of partici- J Clin Oncol 17:2659-2669. 1999 by American pants scoring above a clinically significant level on the Society of Clinical Oncology. CES-D. No differences were found between groups for THIS IS THE INITIAL report of the findings from the
health-related quality of life (HRQL) component of
the National Surgical Adjuvant Breast and Bowel Project
This report covers the baseline HRQL examination and the first 36
(NSABP) Breast Cancer Prevention Trial (P-1), a multicen-
months of follow-up data on 11,064 women recruited over the first 24
ter, double-blinded, placebo-controlled clinical trial. The
months (June 1, 1992, to May 31, 1994) of the study. This cohort of
purpose of this report is to provide a concise overview of the
women represents 82.6% of the total P-1 accrual (n ϭ 13,388). Restrictions were imposed on the initial HRQL report for two reasons.
P-1 HRQL findings and an assessment of the effects of
First, by limiting our attention to this cohort of women, we avoided the
tamoxifen, when used as a preventative agent, on self-
potential bias created by events beginning in March 1994,4,5 which
reported symptoms and everyday physical, emotional, and
resulted in a suspension of accrual to the P-1 study. Second, a focus on
social functioning. Recommendations have been provided
the first 36 months of data collection permitted improved control overtypes of missing HRQL data because all 11,064 participants should have
that may be helpful to physicians involved in counseling
completed the eight scheduled examinations before the disclosure of the
women considering the use of tamoxifen in the setting of
results of the trial in the spring of 1998.
The primary objective of the P-1 study was to evaluate
whether 5 years of tamoxifen therapy would reduce the
From the National Surgical Adjuvant Breast and Bowel Project
incidence of invasive breast cancer in women at an increased
(NSABP) Operations and Biostatistical Centers, Pittsburgh, PA, and
risk for the disease. Secondary objectives were to assess the
Jonsson Comprehensive Cancer Center, University of California Los
incidence of ischemic heart disease, bone fractures, and
other events, such as depression, that might be associated
Submitted December 7, 1998; accepted April 22, 1999. Supported by public health service grants from the National Cancer
with the use of tamoxifen. Eligible participants were random-
Institute (NCI-U10-CA-37377/69974) and a career development award
ized either to 20 mg daily of tamoxifen or to a placebo for a
from the Department of Defense (DAMD17-97-1-7058).Address reprint requests to Richard Day, PhD, Department of
Detailed descriptions of the rationale, planning, and
Biostatistics, Graduate School of Public Health, 130 DeSoto St,University of Pittsburgh, Pittsburgh, PA 15261; email rdfac@vms.
design of the of the Breast Cancer Prevention Trial and the
HRQL component of the P-1 study, as well as specific
1999 by American Society of Clinical Oncology.
instruments, have been provided in separate reports.1-3
Journal of Clinical Oncology, Vol 17, No 9 (September), 1999: pp 2659-2669
Imputation procedures for missing items in otherwise complete
scales were only used for eight SF-36 subscales, as recommended in the
The 104-item P-1 HRQL Questionnaire3 was composed of the Center
SF-36 scoring manual.9 No data imputation was carried out for other
for Epidemiological Studies–Depression Scale (CES-D, 20 items), the
scales, and incomplete scales were considered missing.6
Medical Outcomes Study (MOS) 36-Item Short Form Health StatusSurvey (SF-36, 36 items), the MOS sexual functioning scale (five
items), and a symptom checklist (SCL, 43 items). The questionnairewas scheduled to be administered to all participants before randomiza-
Table 1 lists the demographic, medical, and behavioral
tion (baseline), at 3 months, at each succeeding 6-month examination
characteristics of our participant cohort of 11,064 women by
for the planned 5 years of treatment, and for 1 year after treatment was
trial group. These data show that the women in the P-1 study
were predominately white (96%), well educated (65% Նsome college), married (70%), professional and technically
trained (68.2%), currently employed (64.9%), and reported a
The P-1 study has multiple, complex levels of missing and incom-
middle- to upper-middle class family income (median,
plete data. In the case of self-administered instruments, such as the
$35,000 to $49,999). None of the variables in Table 1 show a
HRQL questionnaire, participants could leave items blank by error or
striking imbalance between the two trial groups.
because they did not wish to answer the question.6 Beyond this, the
Figure 1 charts the overall proportion and total numbers
staffs of collaborating centers were generally unable to collect self-
of women completing the HRQL questionnaire at each
administered instruments on participants who quit taking pills becausethey no longer appeared for follow-up examinations, although many of
examination. It provides a general measure of comparative
these participants can still be observed for primary end points (eg, breast
participant adherence with regard to the HRQL question-
cancer and fractures). In addition, there are participants who did not
naire in the two trial groups. Both trial groups showed a
complete all of the scheduled follow-up HRQL questionnaires because
consistent decline in HRQL adherence across the first 36
of the disclosure of the trial results in the spring of 1998,1 although they
months of the study, averaging 4.2% per examination in the
are still observed for primary end points. Finally, a small proportion ofparticipants (1.7%) were lost to follow-up, even for primary end points.
placebo group and 4.6% per examination in the tamoxifengroup. The proportion of HRQL-adherent participants wassmaller in the tamoxifen than in the placebo group at every
one of the seven follow-up examinations (sign test, P ϭ
The P-1 HRQL data set is composed of multiple HRQL instruments,
.0078), with a maximum difference of 3.1% occurring at 36
each with its own psychometric properties and research history.3 This
complexity is magnified by the fact that data distributions and patterns
A number of demographic, clinical, and HRQL variables
of missing data differ across the various instruments included in the
were examined to investigate whether differences could be
HRQL questionnaire. In addition, sample sizes are large, resulting in thepossibility of statistically significant findings for clinically negligible
detected between the women who failed to complete the
effects. All of these considerations argue for future detailed analyses of
HRQL questionnaire at 36 months in the tamoxifen and the
the data from each specific instrument. In this initial report, however,
placebo groups. These variables included mean age (tamoxi-
our aims were essentially descriptive in nature and emphasized basic
fen ϭ 53.1 years v placebo ϭ 53.5 years) and mean RR (5.42
comparisons of the two trial groups. In making these comparisons, we
v 5.43), treatment status (10.1% v 10.5% on treatment),
seek to identify consistent differences, between the trial groups, usingsimple nonparametric procedures. The sign test7 is used to examine the
breast cancer in a first-degree relative (76.89% v 78.40%),
consistency of binary differences (Ϯ) between the two trial groups
prior estrogen use (32.5% v 33.3%), mean maximum CES-D
across time, independent of the magnitude of these differences. A
score (12.52 v 12.46), and mean maximum number of
one-sided alternative is routinely used because tamoxifen is expected to
reported symptoms on the SCL (14.2 v 13.9). These
have a negative effect on most short-term measures of HRQL.
comparisons suggested that participants who failed to com-
Friedman’s test,7 implemented as a generalization of the paired signtest,8 was used as a nonparametric analog to the two-way analysis of
plete the HRQL questionnaire in each group were similar
variance when we wanted to block on a specific factor, such as age
group. Positive findings, with regard to consistent differences between
When, within a treatment group, the same variables were
trial groups, were independently reviewed for magnitude to assess their
used to compare HRQL adherent and nonadherent women,
clinical and functional significance for the participants’ quality of life.
only the treatment status variable was different between the
Clinical experience, as well as initial statistical investigations of the
P-1 HRQL data set, suggested that the age of the study participants was
two groups. A significantly greater proportion of HRQL-
a key factor contributing to the observed distribution of HRQL
adherent women in both groups remained on treatment
measures. Hence, the results presented here from various HRQL
(87.0% v 89.6%) compared with HRQL-nonadherent women
instruments were routinely stratified by three age groups (35 to 49 years,
(10.1% v 10.5%). In other words, adherence in the HRQL
50 to 59 years, and 60 years or older) that generally paralleled
component of P-1 was largely a reflection of treatment
menopausal status. Relative risks (RRs) or absolute differences in meancounts are presented in the tables to estimate differences in effect size
adherence. This was because most collaborating centers did
not have the staff resources to administer the HRQL
HEALTH-RELATED QUALITY OF LIFE AND TAMOXIFEN
Table 1. Demographic, Clinical, and Health Behavior Characteristics of P-1 Table 1. Demographic, Clinical, and Health Behavior Characteristics of P-1 HRQL Study Participants (N ؍ 11,064) (Cont’d) HRQL Study Participants (N ؍ 11,064)
53.83 Ϯ 9.167 53.82 Ϯ 9.184 53.83 Ϯ 9.175
questionnaire via the telephone or mail to women who
stopped treatment and failed to appear for their scheduled
By the 36-month examination, 3,421 women had stopped
their assigned treatment and failed to fill out the HRQL
questionnaire for at least 6 months. Table 2 lists the primary
reasons these women gave for stopping treatment. The
placebo and tamoxifen groups did not differ with regard to
protocol-specified events, such as invasive breast cancer,
depression, or deep vein thrombosis, or other medical
reasons, such as anxiety disorders or cardiovascular condi-
tions. Hot flashes were clearly the most frequently reported
sign or symptom that caused women to stop their assigned
treatment (251 women); they occurred most often in thetamoxifen group (184 women). When stopping their as-
Fig 1. Proportion of participants in the tamoxifen group and placebo group completing HRQL question- naire by examination (placebo, n ؍ 5,537; tamoxifen, n ؍ 5,527). Fig- ures on chart are the number of women in the placebo/tamoxifen groups completing the HRQL ques- tionnaire and the difference be- tween TAM and placebo groups in terms of percent missing HRQL data.
signed treatment, participants in the placebo group were
regard to the relationship between the two trial groups
more likely to cite other nonmedical reasons, such as fear of
emerged from the analysis of the five-item mental health
side effects, change of mind, or desire to adopt an alternative
subscale on the MOS SF-36 (not shown).
The results of the SF-36 are summarized using the
Table 3 shows the proportion of P-1 participants, by age
physical component summary (PCS) and mental component
group and examination, who scored above the most fre-
summary (MCS) scores12 and the eight SF-36 subscales. The
quently used clinical cutoff (Ն 16) on the CES-D.10,11 The
PCS and MCS scores represent aggregate measures that
youngest age group (35 to 49 years) in both trial groups
combine data from the eight subscales generally reported on
consistently had the highest proportion of members scoring
the SF-36. The PCS aggregates data from the Physical
above the clinical cutoff, followed by the 50- to 59-year-old
Functioning, Role-Physical, Bodily Pain, and General Health
age group (Friedman test, P ϭ .001 tamoxifen and placebo).
subscales, while the MCS draws on data from the Vitality,
The RRs listed in Table 3 show that, for all three age groups,
Social Functioning, Role-Emotional, and Mental Health
the magnitude of the differences is small, and there was no
subscales. The PCS and MCS are scored using norm-based
consistent excess of participants in the tamoxifen groupscoring above the clinical cutoff on the CES-D when
Table 3. Proportion of Participants in Tamoxifen Arm With a Clinically
compared with the placebo group. Similar findings with
Significant Score (м 16) on the CES-D by Age Group and Examination Table 2. Reasons for Stopping Assigned Therapy by Participants Not Completing Quality of Life Questionnaire (Baseline to 36-Month Examination, n ؍ 3421)
12 months 0.128 0.937 0.122 0.999 0.096 0.989 0.116 0.968
18 months 0.139 0.892 0.126 0.918 0.101 0.929 0.123 0.908
30 months 0.142 0.978 0.107 0.961 0.104 0.934 0.120 0.959
HEALTH-RELATED QUALITY OF LIFE AND TAMOXIFEN
methods; both component scores have a mean of 50 and a
The youngest age group (35 to 49 years) had the greatest
SD of 10 in the general United States (U.S.) population. This
proportion of participants reporting vaginal discharge at
means that the PCS and MCS can be meaningfully com-
each examination (median, 35.5%; Friedman test, P Ͻ
pared with one another, and their scores have a direct
.001), and the oldest age group (Ն 60 years) reported the
interpretation in relation to the distribution of scores in the
greatest increase of vaginal discharge relative to the placebo
controls (median RR, 3.05; Friedman test, P ϭ .005).
Figure 2 charts the PCS and MCS for the tamoxifen and
Figure 4 summarizes the information from the five items
placebo groups at each examination and by age group. As
on the MOS sexual functioning scale. Figure 4A shows that
expected, mean PCS declines across the age groups. At
a greater proportion of participants in the tamoxifen group,
follow-up examinations, the tamoxifen group was consis-
as compared with the placebo group, reported being sexually
tently lower on the PCS only in the 50- to 59-year-old age
active during the 6 months before each follow-up examina-
group (one-sided sign test, P ϭ .065). However, the absolute
tion. Although apparently consistent (P ϭ .031), the abso-
differences were small, approximating one tenth of an SD.
lute difference was small (mean, 0.78%) and may have been
With regard to the MCS, all of the age groups scored above
caused by chance. Figure 4B through 4E show that a small
the mean MCS for the general U.S. population, and no
but consistently larger percentage of participants in the
consistent differences emerged between the two trial groups.
tamoxifen group reported a definite or serious problem in
Figure 3 summarizes the overall data from eight subscales
three of the four specific domains of sexual functioning
on which the component subscores are based.
Table 4 lists the mean number of symptoms reported on
the 43-item SCL by age group and examination. The mean
number of symptoms reported was consistently highest in
We observed in our earlier article3 that measuring the
the 50- to 59-year-old age group, followed by the 35- to
impact of new treatments on HRQL is particularly important
49-year-old and 60 years or older age groups (Friedman test,
within the context of disease-prevention and health-
P ϭ .001 tamoxifen and placebo). The participants in the
promotion trials. Compared with patients suffering from
tamoxifen group also reported a small but consistent excess
clinically manifest disease, decrements in overall quality of
in the mean number of symptoms (Ͻ one) reported at 19 of
life are likely to have a much greater impact on the
the 21 age-stratified follow-up examinations (3 to 36 months;
subjective appraisal of treatment acceptability and the
one-sided sign test, 35 to 49 years, P ϭ .0078; 50 to 59 years
maintenance of long-term treatment adherence among high-
and Ն 60 years, P ϭ .065) (Table 4).
risk but otherwise healthy individuals. This report covers the
Table 5 provides information on the proportion of women
initial HRQL findings from a large, multicenter chemopre-
in the tamoxifen and placebo groups who reported symp-
vention trial, which has shown that tamoxifen reduced the
toms on the SCL at least once during the treatment period, ie,
risk of invasive breast cancer in high-risk women by 49%
the period excluding baseline but including the seven
during the first 5 years of administration. Given the apparent
follow-up examinations. The five symptoms with the great-
clinical efficacy of tamoxifen in the prevention setting, it is
est relative difference between the two trial groups are given
important to assess whether the various secondary effects of
for each age group, and the 10 symptoms with the greatest
the drug might act to reduce this practical efficacy.13-15
relative difference are presented for all participants com-
The cohort of women taking part in the P-1 study clearly
was not representative of the general population. They were
Tables 6 and 7 give detailed information, by age group
predominately white, well educated, and middle class, with
and examination, on the reported frequency of hot flashes
a strong professional and technical orientation. The initial
and vaginal discharge in the trial groups. The proportion of
HRQL findings presented in this report must be assessed
participants who reported hot flashes was elevated in all age
within the context of the socioeconomic and cultural charac-
groups of the tamoxifen group at every follow-up examina-
tion. Among the participants in the tamoxifen group, the 50-
The subcohort of women discussed in this report represent
to 59-year-old age group had the largest proportion of
82.6% of the total study cohort. This subcohort was chosen
women reporting hot flashes at each examination (median,
to exclude potential biases, because of external factors
69.8%; Friedman test, P ϭ .001), but the youngest age group
eventuating in the suspension of accrual in P-1, and to
(35 to 49 years) showed the greatest relative increase in
control for the amount and types of missing data. Despite
proportion of women reporting hot flashes (median RR,
this, we still lost 31.5% of our participants by the 36-month
1.50; Friedman test, P ϭ .011). Vaginal discharge was the
follow-up examination. This proportion closely approxi-
most consistently elevated symptom in the tamoxifen group.
mates the 10%-per-year loss to follow-up rate predicted at
Fig 2. Mean scores by age group and examination on SF-36 physical and mental component scores (higher scores represent better quality of life).
HEALTH-RELATED QUALITY OF LIFE AND TAMOXIFEN
Fig 3. Mean SF-36 subscale scores by examination. Table 4. Mean Number of Total Symptoms Reported on Symptom Checklist by Age Group and Examination
Abbreviation: TAM, tamoxifen. *Difference ϭ tamoxifen minus placebo.
the beginning of the P-1 trial and is similar in pattern and
but, instead, to the prevalence of clinically significant
number to the adherence data recently reported in a second
affective distress that might be associated with a number of
large, multicenter chemoprevention trial of hormone replace-
specific psychiatric disorders. However, if tamoxifen use
ment therapy for heart disease.16 We have shown that there is
was associated with the onset of clinically diagnosable
only a small difference in the proportion of nonadherent
depression, we would have expected to see a consistent
participants in the tamoxifen and placebo groups and that the
excess of individuals scoring Ն 16 on the CES-D in the
nonadherent women in both trial groups have generally
tamoxifen group. No such consistent excess was observed.
similar key demographic, clinical, and HRQL variables.
These findings agreed with the data from the mental health
Given these considerations, it seems unlikely that a maxi-
mum difference of 3% in the HRQL follow-up rates between
The MOS SF-36 served in this study as a measure of
the two groups was sufficient to create a significant bias in
overall HRQL. For this initial report, we have presented data
from the SF-36 in terms of two high-level component
HRQL adherence is closely related to treatment adher-
scores12 and the eight basic subscales generally used in
ence. Based on the reasons for quitting treatment, it would
scoring this instrument.9 Neither of these two methods of
seem that nonadherent women in both trial groups were
summarizing the SF-36 data demonstrated any clinically
those who were sensitive to the actual or possible occurrence
significant differences between the tamoxifen and placebo
of side effects caused by tamoxifen.
Much concern has been expressed about a potential
The first clear signs of consistent differences between the
relationship between tamoxifen use and the onset of depres-
tamoxifen and placebo groups were observed in the SCL. In
sion.17-21 Women who reported a history of depressive
19 out of 21 follow-up comparisons, the mean number of
episodes or a history of treatment for nervous or mental
symptoms reported on the SCL were consistently different
disorders were not excluded from the trial. A brief eight-item
by age group (50 to 59 years Ͼ 35 to 49 years Ͼ 60ϩ years)
affective screening questionnaire based on the CES-D and
and by trial group (tamoxifen Ͼ placebo). The absolute
the Diagnostic Interview Schedule22 was part of the baseline
differences between the trial groups were relatively small
examination.23 Using data from this brief screening instru-
and tended to be associated with the types of vasomotor,
ment, local investigators were alerted to eligible participants
gynecologic, and sexual functioning symptoms previously
showing signs of potentially serious affective distress at the
baseline examination and caution was advised regarding
The data from the MOS sexual functioning scale indicate
their enrollment onto the trial. However, women who
that relatively small (Ͻ 4.0%) but consistent differences
showed current signs of affective distress or depression were
exist between the two groups in regard to the proportion of
not routinely excluded from the trial.
women reporting definite or serious problems in at least
With regard to the primary screening instrument used in
three specific domains of sexual functioning, sexual interest,
the follow-up examinations, it has been pointed out that ‘‘the
arousal, and orgasm. These problems do not seem to be age
items in. (the CES-D) are generally related to affective
group specific. Despite these findings for specific domains
distress but not to any particular psychiatric disorder.’’11 For
of functioning, there is no evidence that these problems
this reason, the numbers listed in Table 3 refer not to the
result in a reduction of the overall proportion of women in
prevalence of clinically diagnosable depressive disorders
the tamoxifen group who are sexually active.
HEALTH-RELATED QUALITY OF LIFE AND TAMOXIFEN
Table 5. Symptoms Reported at Least Once Between Months 3 and 36 Table 6. Proportion of Women Reporting Hot Flashes in Tamoxifen Arm and With the Largest Relative Difference Between Trial Arms RR Compared to Placebo Arm by Age Group and Examination
0.258 0.959 0.533 0.989 0.268 1.030 0.346 0.991
0.581 1.588 0.761 1.241 0.511 1.413 0.616 1.399
0.610 1.666 0.765 1.268 0.503 1.481 0.626 1.455
12 months 0.614 1.525 0.740 1.273 0.460 1.412 0.606 1.396
18 months 0.613 1.510 0.715 1.239 0.419 1.461 0.586 1.387
24 months 0.622 1.457 0.681 1.199 0.388 1.311 0.570 1.322
30 months 0.627 1.362 0.642 1.206 0.330 1.177 0.541 1.265
36 months 0.627 1.414 0.667 1.276 0.364 1.362 0.560 1.348
of these possible symptoms. Weight gain and depression,
two clinical problems anecdotally associated with tamoxifen
treatment in women with breast cancer, did not increase in
frequency in this large placebo-controlled trial of healthy
women. This is good news that must also be communicated
to women. An informed discussion with a woman consider-
ing tamoxifen therapy should include these points in the
Disclosure of likely and unlikely symptoms should pre-
pare a woman for what she might experience and reduce her
anxiety or concerns should she begin preventive therapy.
Without the detailed evaluation of HRQL data obtained in
the P-1 trial, we would not be able to provide this level of
information and reassurance to women considering preven-tive therapy. In addition, the setting of preventive therapy
Based on these data, we conclude that tamoxifen use is
differs considerably from the treatment of breast cancer.
associated with an increase in specific vasomotor, gyneco-
Therefore, if a woman experiences untoward symptoms
logic, and sexual functioning symptoms. At the same time,
after starting tamoxifen treatment, the medication can be
we did not observe any evidence that overall physical and
discontinued if the symptoms cannot be controlled or her
emotional well being were significantly affected by these
personal assessment of the risks and benefits changes.
differences in the frequency of symptoms. We also found noevidence on the CES-D or the SF-36 mental health scale foran association in any age group between tamoxifen use and
Table 7. Proportion of Women Reporting Vaginal Discharge in Tamoxifen
an increase in the proportion of women reporting clinically
Arm and RR Compared to Placebo Arm by Age Group and Examination
significant levels of affective distress and/or depression.
How should clinicians integrate the results from the HRQL
study data into decision-making and recommendations to
women considering the use of tamoxifen in the setting of
0.201 0.957 0.135 1.041 0.058 0.907 0.138 0.975
prevention? As demonstrated by the SCL data from the
0.379 1.549 0.308 2.023 0.275 3.665 0.326 1.972
placebo group of the trial, many symptoms experienced by
0.391 1.686 0.302 1.931 0.269 3.057 0.327 1.973
12 months 0.380 1.700 0.304 1.973 0.262 3.333 0.321 2.020
women who participated in this study are age and meno-
18 months 0.363 1.558 0.278 2.251 0.252 3.029 0.303 1.961
pause related and exist independent of the use of tamoxifen.
24 months 0.341 1.797 0.272 1.991 0.238 2.994 0.288 2.052
However, several symptoms are substantially more frequent
30 months 0.325 1.633 0.282 2.404 0.246 3.075 0.288 2.083
in women using tamoxifen; these include vasomotor symp-
36 months 0.316 1.671 0.264 2.332 0.241 3.096 0.277 2.095
toms (cold sweats, night sweats, and hot flashes), vaginal
discharge, and genital itching. Women need to be informed
Fig 4. Proportion of women in the tamoxifen group and placebo group reporting a definite or serious problem in past 4 weeks on MOS sexual functioning scale (B through E, women who reported being sexually active in last 6 months).
HEALTH-RELATED QUALITY OF LIFE AND TAMOXIFEN
The current report is a brief overview of the P-1 study
HRQL data that focuses on important clinical and functional
We thank Carol Redmond, DSc, University of Pittsburgh; Leslie
implications of tamoxifen use for women’s overall HRQL. It
Ford, MD, National Cancer Institute, Bethesda, MD; Carol Moinpour,
will be supplemented in the future by a series of additional
PhD, Southwest Oncology Group Statistical Center; John E. Ware, Jr,New England Medical Center, Boston, MA; David Cella, Northwestern
methodologic and clinical reports that will provide in-depth
University, Chicago, IL; Sheela Goshal and Wei Chen, NSABP
analyses of the data obtained from each one of the several
Biostatistical Center; and members of the NSABP Prevention Quality of
1. Fisher B, Costantino JP, Wickerham L, et al: Tamoxifen for the
15. Gorin MB, Day R, Costantino JP, et al: Long term tamoxifen
prevention of breast cancer: A report from the NSABP P-1 study. J Natl
citrate and potential ocular toxicity. Am J Ophthalmol 125:493-501,
2. Fisher B, Costantino J: Highlights of the NSABP Breast Cancer
16. Hulley S, Grady D, Bush T, et al: Randomized trial of estrogen
Prevention Trial. Cancer Control 4:78-86, 1997
plus progestin for secondary prevention of coronary heart disease in
3. Ganz PA, Day R, Ware JE, et al: Base-line quality-of-life
postmenopausal women. JAMA 280:605-613, 1998
assessment in the National Surgical Adjuvant Breast and Bowel Project
17. Cathacart CK, Jones SE, Pumroy CS, et al: Clinical recognition
Breast Cancer Prevention Trial. J Natl Cancer Inst 87:1372-1382, 1995
and management of depression in node negative breast cancer patients
4. Fisher B, Redmond C: Fraud in breast cancer trials. N Engl J Med
treated with tamoxifen. Breast Cancer Res Treat 27:277-281, 1993
18. Love RL, Cameron L, Connell BL, et al: Symptoms associated
5. Fisher B, Anderson S, Redmond C, et al: Reanalysis and results
with tamoxifen treatment in postmenopausal women. Arch Intern Med
after 12 years of follow-up in a randomized clinical trial comparing totalmastectomy with lumpectomy with or without irradiation in the
treatment of breast cancer. N Engl J Med 333:1456-1461, 1995
19. Shariff S, Cumming CE, Lees A, et al: Mood disorder in women
6. Ganz PA, Day R, Costantino JP: Compliance with quality of life
with early breast cancer taking tamoxifen, an estradiol receptor
data collection in the NSABP breast cancer prevention trial. Stat Med
antagonist: An unexpected effect? Ann N Y Acad Sci 761:365-368,
7. Daniel WW: Applied Non-Parametric Statistics. Boston, MA,
20. Moredo Anelli T, Anelli A, Tran KN, et al: Tamoxifen administra-
tion is associated with a high rate of treatment-limiting symptoms in
8. Deshpande JV, Gore AP, Shanubhougue A: Statistical Analysis of
male breast cancer patients. Cancer 74:74-77, 1994
Non-Normal Data. New York, NY, John Wiley & Sons, 1995
21. Pluss JL, Dibella NJ: Reversible central nervous system dysfunc-
9. International Resource Center for Health Care Assessment: How
tion due to tamoxifen in a patient with breast cancer. Ann Intern Med
to Score the SF-36 Health Status Survey. Boston, MA, New England
22. Robins LN, Helzer JE, Croughan J, et al: National Institute of
10. Radloff LS: The CES-D scale: A self-report depression scale for
Health Diagnostic Interview Schedule: Its history, characteristics and
research in the general population. Appl Psychol Meas 1:385-401, 1977
validity. Arch Gen Psychiatry 35:837-846, 1978
11. Roberts RE, Vernon SW: The Center for Epidemiologic Studies
23. Burnam MA, Wells KB, Leake B, et al: Development of a brief
Depression Scale: Its use in a community sample. Am J Psychiatry
screening instrument for detecting depressive disorders. Med Care
12. Ware JE, Kosinski M, Keller SD: SF-36 Physical and Mental
Summary Scales: A User’s Manual (3rd Printing Revised). Boston, MA,
24. Fisher B, Dignam J, Bryant J, et al: Five versus more than five
The Health Institute, New England Medical Center, 1994
years of tamoxifen therapy for breast cancer patients with negative
13. Fisher B: A commentary on endometrial cancer deaths in
lymph nodes and estrogen receptor-positive tumors. J Natl Cancer Inst
tamoxifen-treated breast cancer patients. J Clin Oncol 14:1027-1039,
25. Fisher B, Costantino J, Redmond C, et al: A randomized clinical
14. Fisher B, Costantino JP, Redmond CK, et al: Endometrial cancer
trial evaluating tamoxifen in the treatment of patients with node-
in tamoxifen-treated breast cancer patients: Findings from NSABP
negative breast cancer who have estrogen-receptor-positive tumors. N
B-14. J Natl Cancer Inst 86:527-537, 1994
Methicillin-resistant Staphylococcus aureus (MRSA) in the community – laboratory based study Selma Uzunović-Kamberović1, Suad Sivić2 Objective To determine the occurrence and antibiotic resis- Microbiology, 2 Department of social medicine, tance of community-acquired methicillin-resistant Staphylo- Cantonal Public Health Institution Zenica, coccus aureus (MRSA) isolates.
Phytosterols and vascular diseaseSaji John, Alexey V. Sorokin and Paul D. ThompsonPhytosterols and stanols are plant derivatives that competeThe remarkable reductions in low-density lipoproteinwith cholesterol for intestinal absorption and thereby lowercholesterol (LDL-C) levels produced by the hydroxyl-serum cholesterol concentrations. They have beenmethyl-glutaryl coenzyme-A (HMG CoA) redu
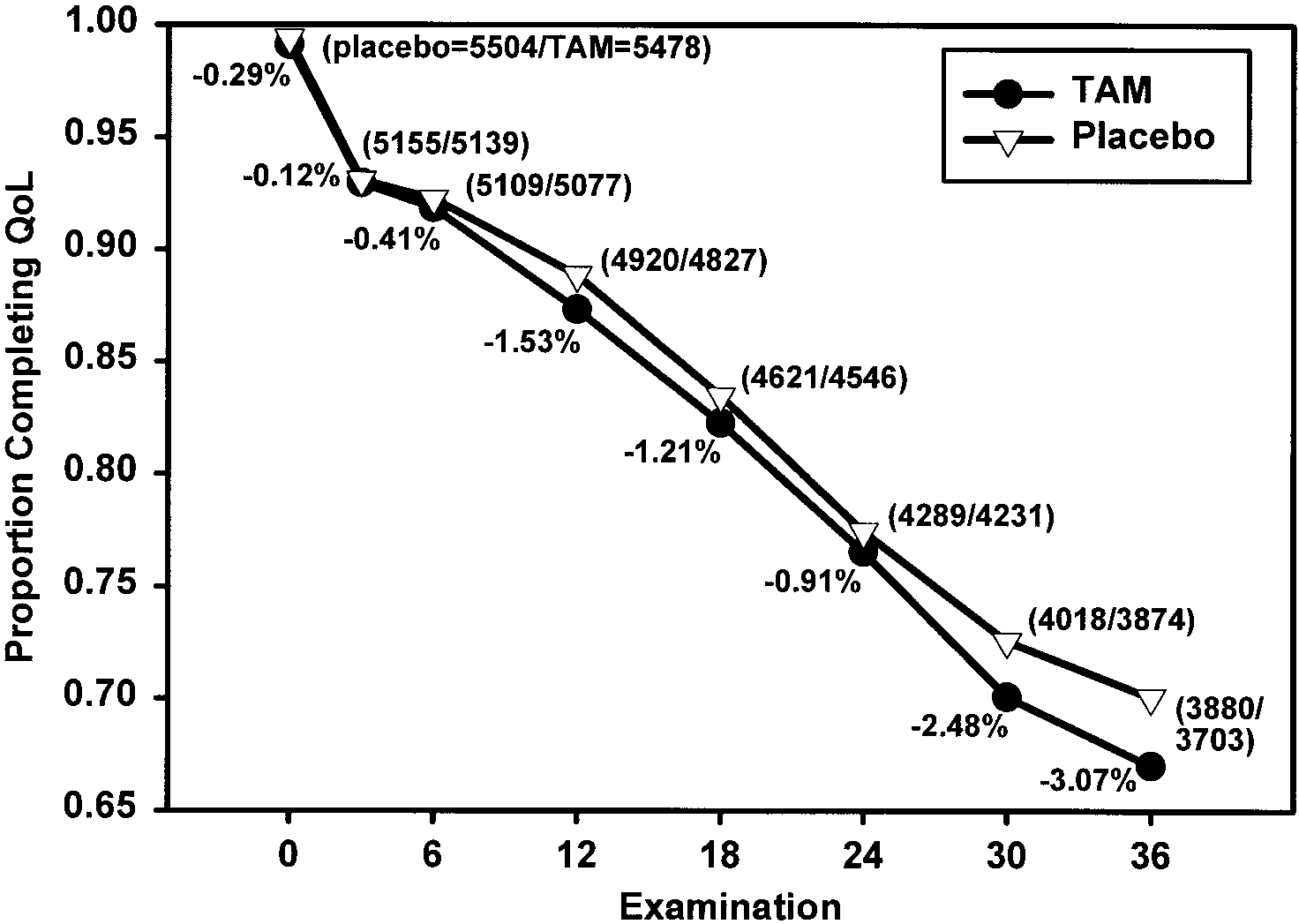 Fig 1. Proportion of participants
Fig 1. Proportion of participants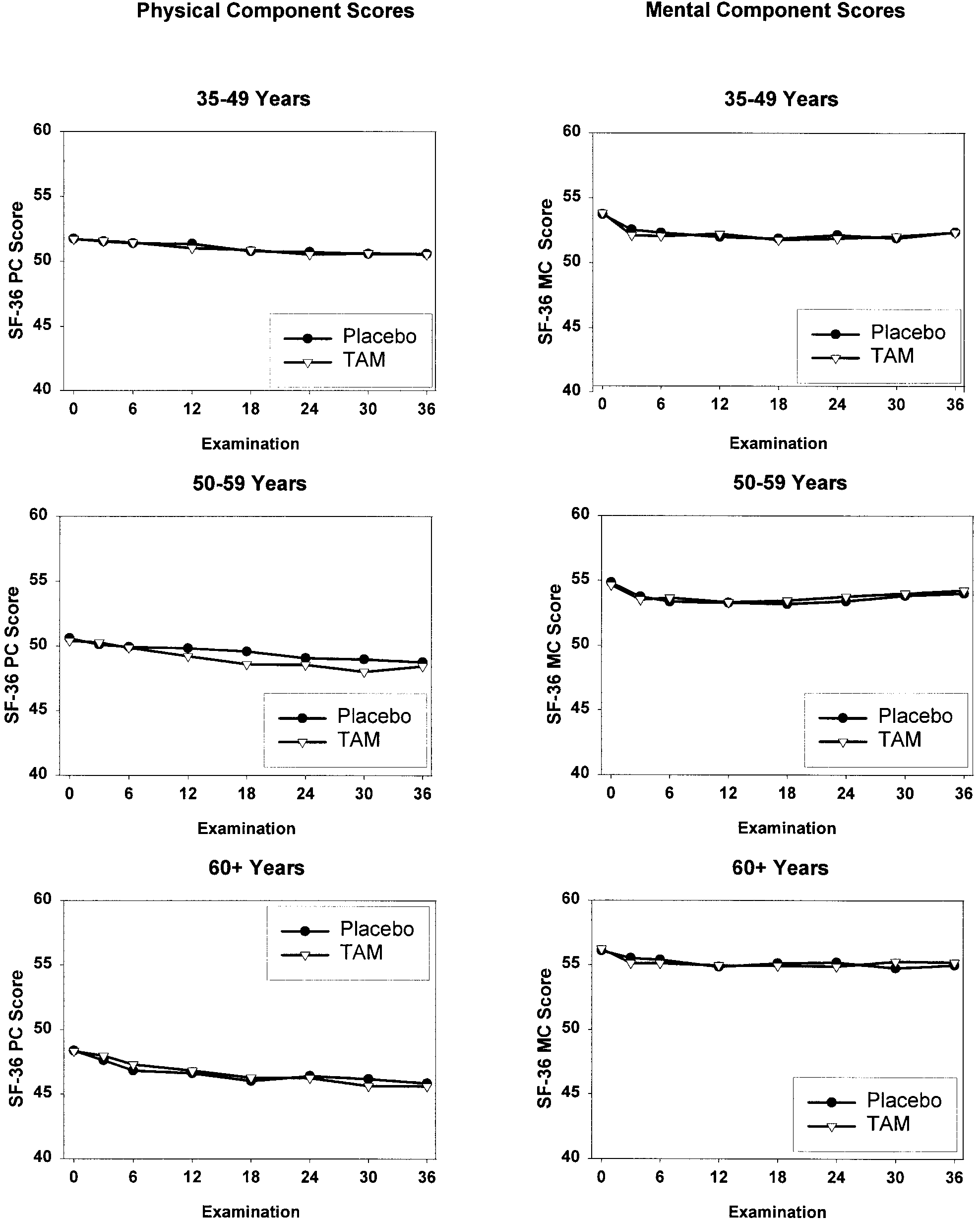 Fig 2. Mean scores by age group and examination on SF-36 physical and mental component scores (higher scores represent better quality of life).
Fig 2. Mean scores by age group and examination on SF-36 physical and mental component scores (higher scores represent better quality of life).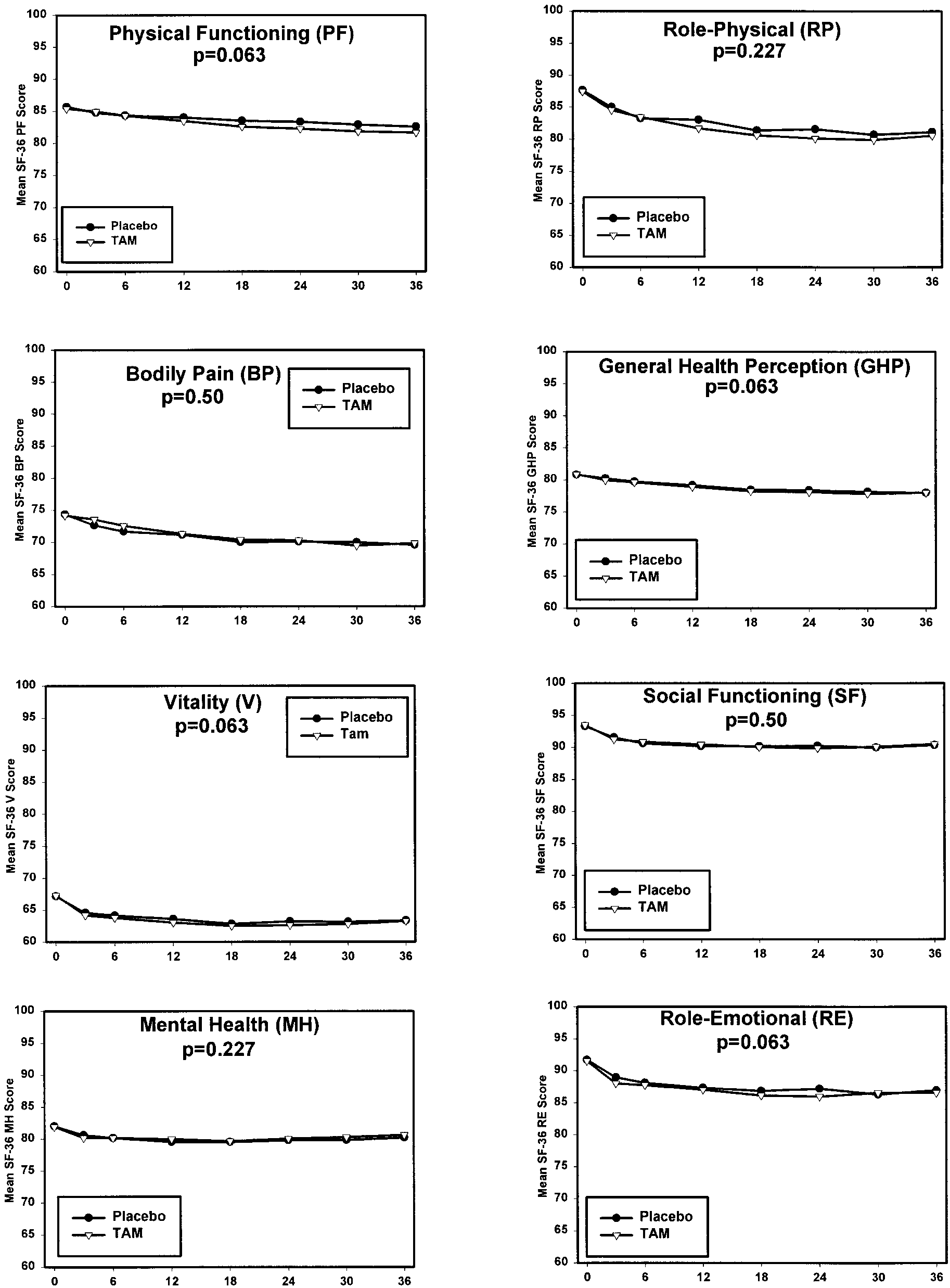 HEALTH-RELATED QUALITY OF LIFE AND TAMOXIFEN
Fig 3. Mean SF-36 subscale scores by examination.
HEALTH-RELATED QUALITY OF LIFE AND TAMOXIFEN
Fig 3. Mean SF-36 subscale scores by examination.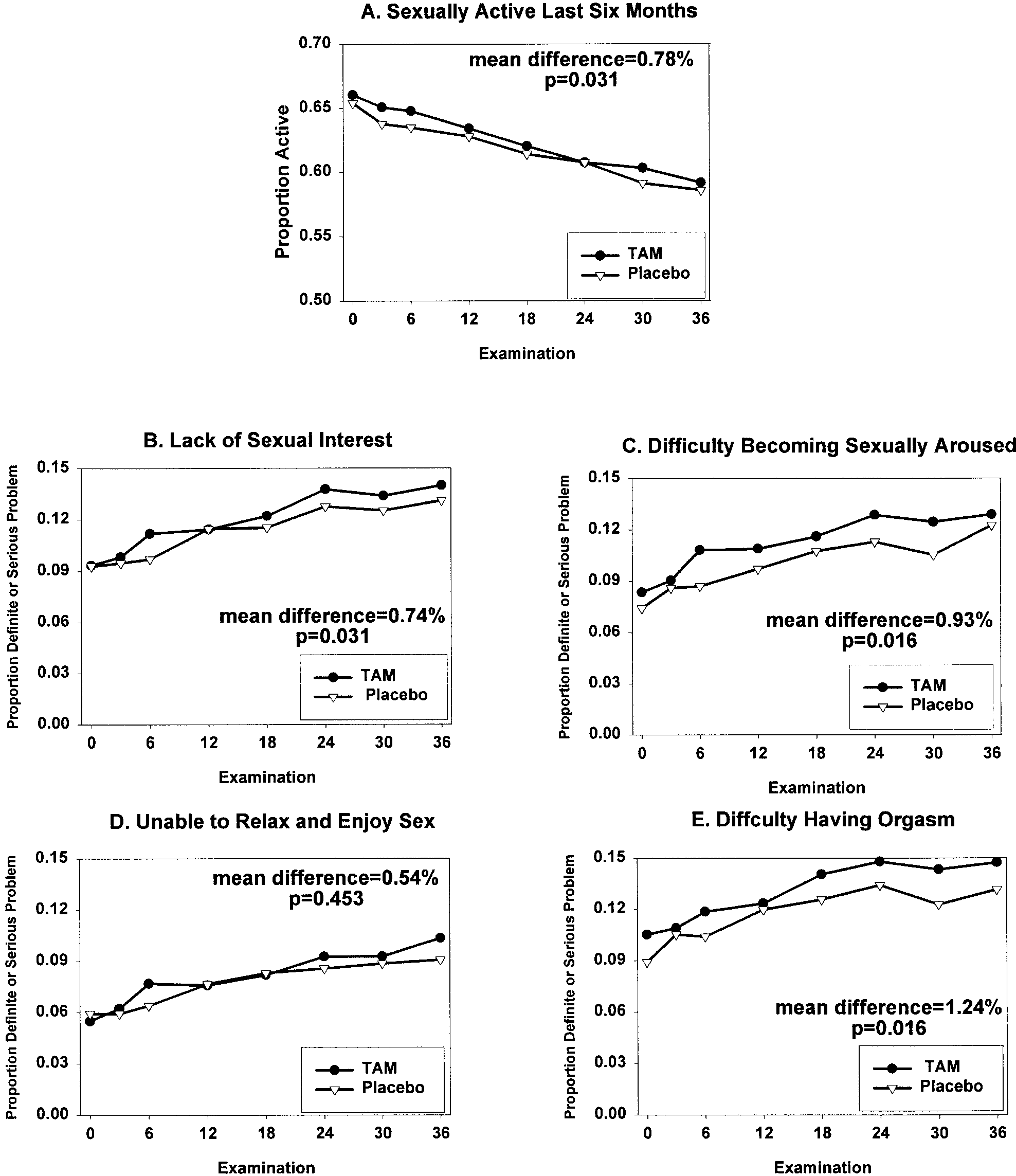 Fig 4. Proportion of women in the tamoxifen group and placebo group reporting a definite or serious problem in past 4 weeks on MOS sexual functioning
Fig 4. Proportion of women in the tamoxifen group and placebo group reporting a definite or serious problem in past 4 weeks on MOS sexual functioning