Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Bay area endo info
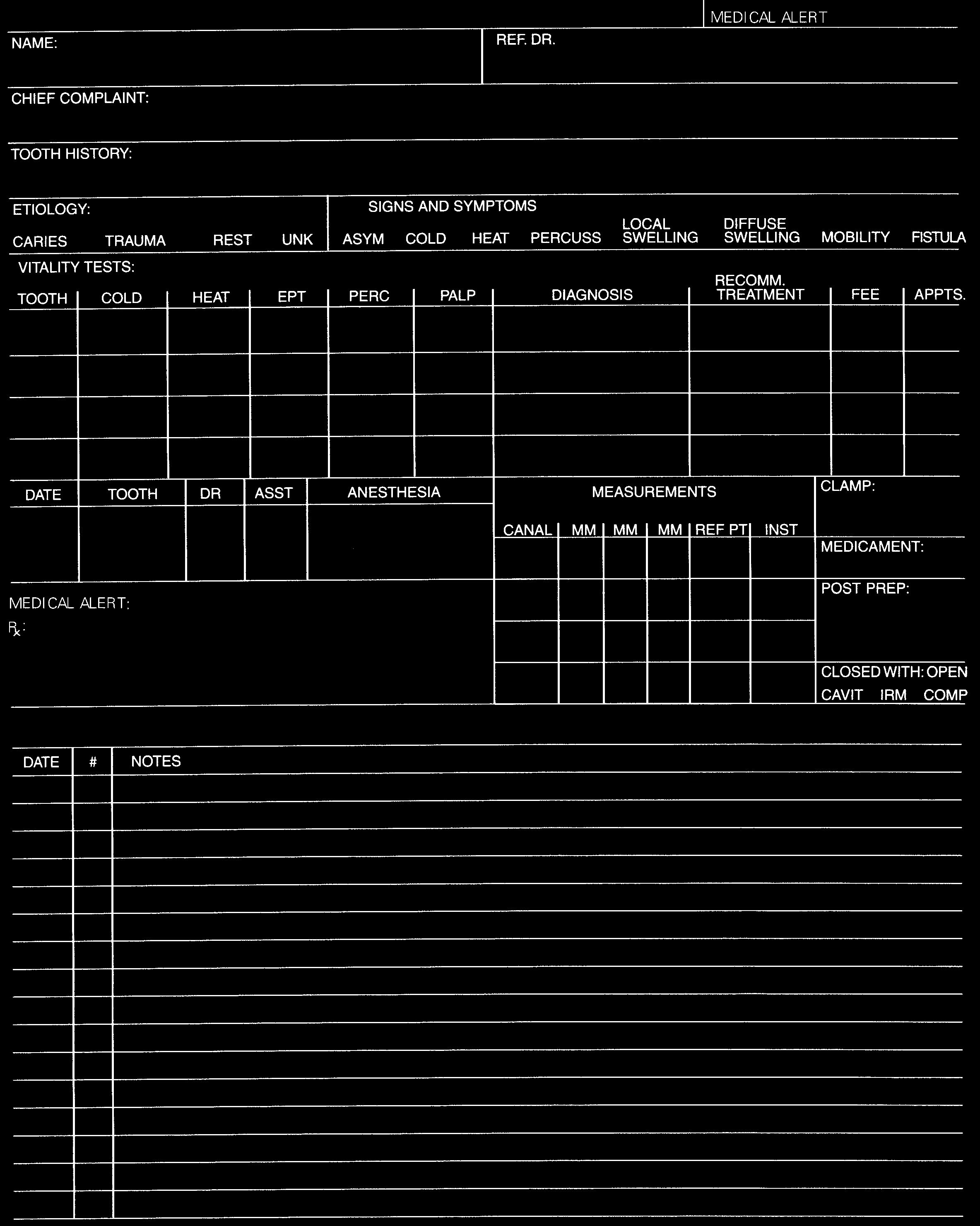
BAY AREA ENDODONTICS, LLP
1550 S. HIGHLAND AVENUE, SUITE A • CLEARWATER, FL 33756 • TELEPHONE (727) 443-3231
PLEASE PRINT THE FOLLOWING INFORMATION
Patient ________________________________________________________________________________Dr.
Home Address __________________________________________________________________________________________________
_______________________________________________________________________________________________________________
Other Address __________________________________________________________________________________________________
Employed by _______________________________________________ Occupation ______________________ Dept. ___________
Name of General Dentist _____________________________ Referred by (if different than general dentist): _____________________
Name of Spouse, Parent / Guardian _________________________________________
__________ S.S. No. _____________________
Employed by _______________________________________ Occupation ___________________ Bus. Phone # ________________
Name of Medical Physician _________________________________________________________ Phone ( _____ ) ______________
Cash ____ Check ____ Credit Card ____ Dental Insurance ____
Dental Insurance Information: Subscriber’s Name ___________________________ Birthdate __________ S.S. No. ______________
Insurance Company _____________________________ Policy No. __________ Group No. ___________ Phone ( _____ ) _____________
Insurance Address _______________________________________________________________________________________________
Secondary Insurance: Subscriber’s Name _________________________________ Birthdate __________ S.S. No. ______________
Insurance Company _________________________ Policy No. _____________ Group No. ____________ Phone ( ____ ) __________
Insurance Address ___________________________________________________________________________________________
In case of Emergency Notify ___________________________________ Relationship _____________ Phone _______________
PLEASE ANSWER ALL QUESTIONS
1. Are you now or have you been under the care of a physician in the past 2 years? .
2. Have you ever been hospitalized or had any operations? .
4. Do you need to premedicate with antibiotics before dental treatment for medical reasons? .
5. Have you experienced any unfavorable reaction to previous dental treatment? .
6. Please list any medications you are currently taking: __________________________________________________
7. Birth Control Pill users must use additional methods while taking antibiotics and for 72 hours afterward. 8. Check any you have had or currently have:
___ PENICILLIN OR OTHER ANTIBIOTICS (if yes, describe) ________________________________________________________________ XYLOCAINE OR OTHER DENTAL ANESTHETICS (if yes, describe) _______________________________________________________ CODEINE OR OTHER PAIN MEDICATION (if yes, describe) ___________________________________________________________
Date ______________ Signature __________________________________________________________________________________
Maßnahmen beim Auftreten einer Influenza-Pandemie im Landkreis Güstrow (Influenza-Pandemieplan Gü) Stand: November 2008 Inhaltsverzeichnis Ziel, Zweck Influenza-Pandemiephasen Surveillance und Meldeweg Zusätzliche Surveillance in der Pandemiephase Sachverständigengruppe Einzuleitende Maßnahmen Allgemeine seuchenhygienische Maßnahmen Schut
Tel.: 07 61 / 47 50 45 INRESA REZEPTURSUBSTANZEN Fax. 07 61 / 4 76 51 77 Preisliste Quartal III / 2013 Artikelnr. Pack. Einheit Preis neu 4-Aminopyridin 34,80 € Adenosin für orale Anwendung oder Infusionslösung a. Anfrage Adenosin für orale Anwendung oder Infusionslösung a. Anfrage Adenosin für orale Anwendung oder Infusionslösung a. Anfrage