 on 60 mg. At visit 9, abstinent smokers comprised 21.7%of the placebo group, 14% of the 30 mg group, and 24.9%of the 60 mg group.
on 60 mg. At visit 9, abstinent smokers comprised 21.7%of the placebo group, 14% of the 30 mg group, and 24.9%of the 60 mg group.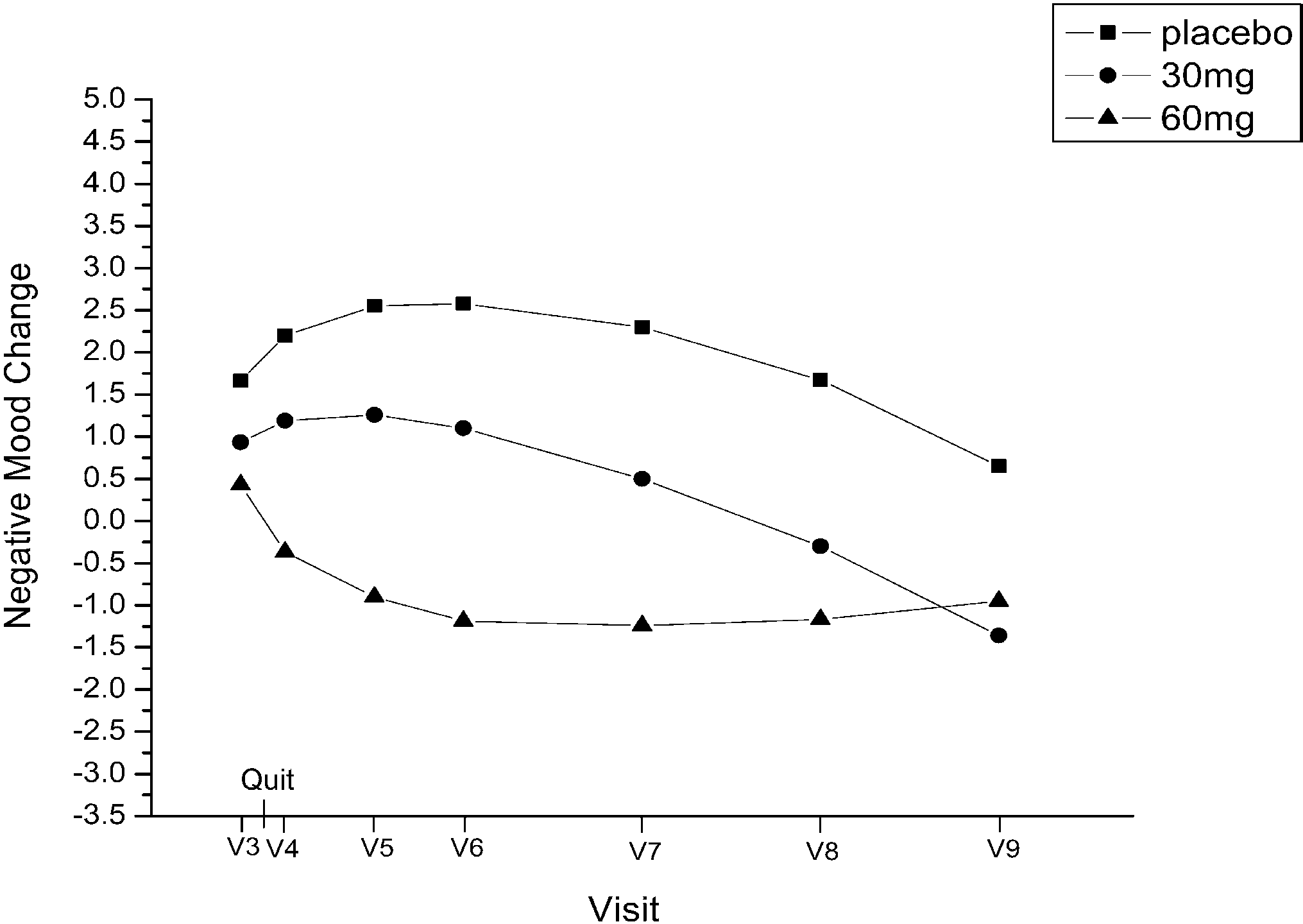 negative affect from visit 3through visit 9, determined by
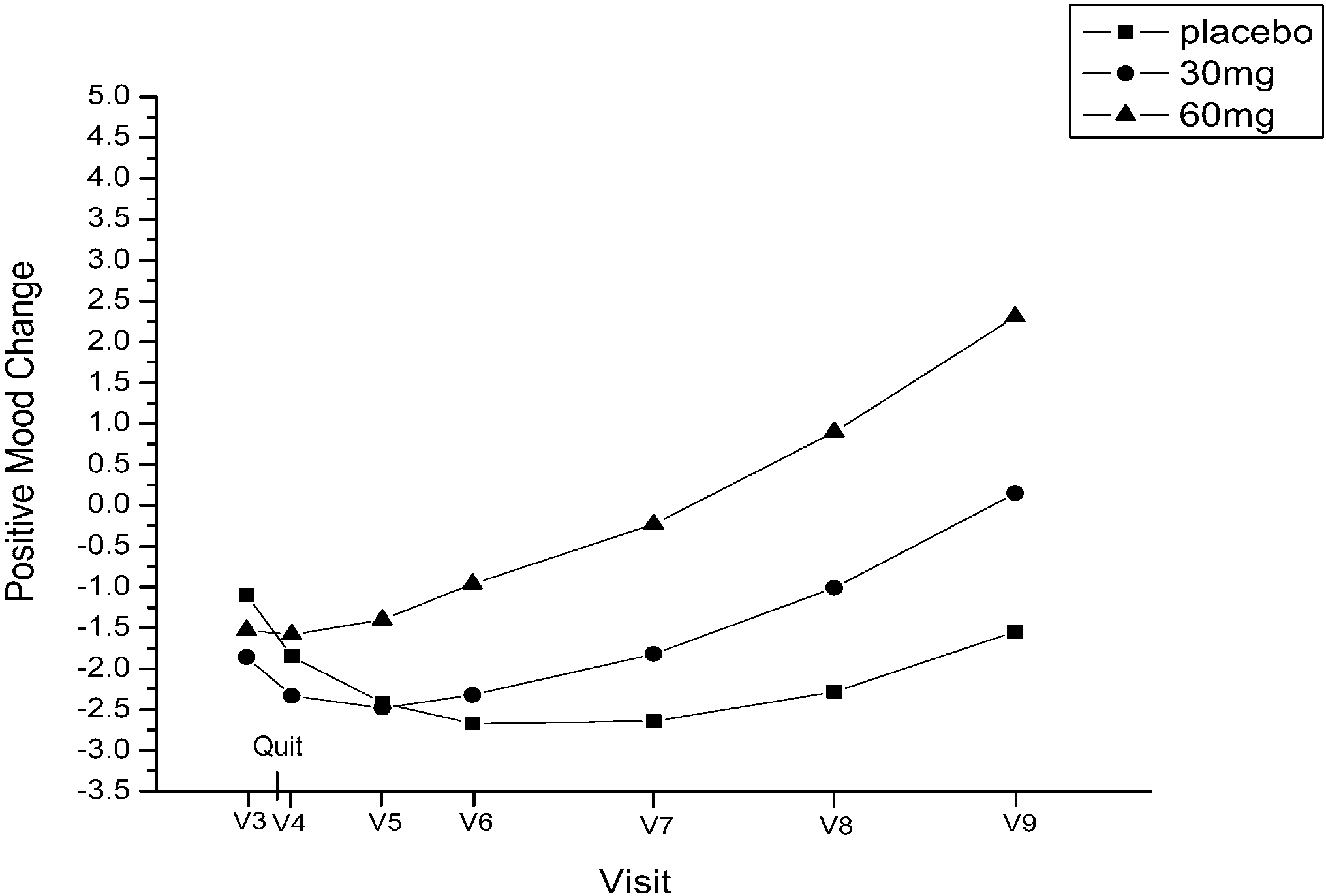
negative affect (linear, P=0.04; quadratic, P=0.04). Re-sults suggest that positive and negative affect changes areinfluenced by fluoxetine rather than feelings of successafter quitting smoking.
negative affect from visit 3through visit 9, determined by
negative affect (linear, P=0.04; quadratic, P=0.04). Re-sults suggest that positive and negative affect changes areinfluenced by fluoxetine rather than feelings of successafter quitting smoking.The road to optimal hemostasis:
The Road to Optimal Hemostasis: Avoiding Misadventures in Bleeding & Thrombosis Bibliography Braunwald E, Antman EM, Beasley JW, et al, for the American College of Cardiology; American Heart Association. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction— summary article: a report of the Ameri