Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Bcr.03.2011.4036.indd
Unusual association of diseases/symptoms
Progressive multi-focal leukoencephalopathy as a rare lethal complication in untreated sarcoidosis
Sabine K Hohlfeld, 1 Huldrych F Günthard, 2 Jonas Zeitz,1 Pascal Locher, 1 Esther Bachli 3
1 Department of Internal Medicine, University Hospital Zurich, Zurich, Switzerland ; 2 Division of Infectious Diseases and Hospital Epidemiology, University Hospital Zurich, Zurich, Switzerland ; 3 Department of Internal Medicine, Uster Hospital, Uster, Switzerland
Correspondence to PD Dr Esther Bachli, [email protected] Summary Progressive multi-focal leukoencephalopathy (PML) is a demyelinating disease of the central nervous system caused by reactivation of John Cunningham virus. It is an opportunistic infection affecting patients who are severely immunocompromised due to an underlying disease or secondary to immunosuppressive therapy. To date, no effective antiviral therapy has been established, though several substances are being investigated. The authors present the case of a 39-year-old previously healthy patient who was diagnosed with PML and sarcoidosis stage III without having received prior immunosuppressive treatment. The patient did not respond to treatment with mirtazapine, which has been used empirically, and deceased shortly after diagnosis. BACKGROUND
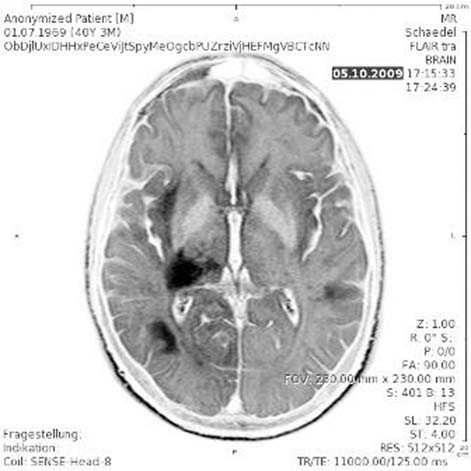
ter of the right temporal and occipital lobe as well as in the
Generally, progressive multi-focal leukoencephalopathy
thalamus and adjacent structures ( fi gure 1 ).
(PML) occurs as an opportunistic infection in severely
Normal cell counts, protein and glucose levels were
immunosuppressed patients. It is seen mostly in untreated
measured in the cerebrospinal fl uid (CSF) and no oligo-
HIV-infected patients (AIDS defi ning illness) and also in
clonal bands were detected. PCR testing for cytomegalovi-
transplant patients and recently it has also been described
rus, Epstein–Barr virus, herpes simplex virus and varicella
in patients with multiple sclerosis treated with natalizu-
zoster virus replication was negative. Yet John Cunningham
mab. In our case, however, we did not have a classical
virus (JCV)-specifi c DNA was detected repeatedly in the
state of immunodefi ciency. Thus, it represents a very rare
CSF, without JCV replication in blood or urine samples.
case and should remind physicians to think of PML also in atypical diseases.
CASE PRESENTATION A 39-year-old Portuguese patient presented with left-sided weakness and hypoesthesia, which had developed over a period of days. Additionally, he had lost 13% of his body- weight during the past 2 months and suffered from non- productive cough for several weeks. To date, he had been healthy and had not received any medication. The family history was non-contributory. Neurological examination revealed mild paresis and hypoesthesia of the left limb, left-sided hyperrefl exia, gait ataxia, left haemianopsia and hemineglect. INVESTIGATIONS Chest x-ray and a CT scan showed a pronounced medi- astinal lymphadenopathy and reticulo-nodular lung tissue densities consistent with advanced sarcoidosis (stage III) as well as a marked splenomegaly (22 cm). The bronchoalve- olar lavage displayed an elevated CD4+/CD8+ ratio (factor 5.6). Lung and bone marrow biopsies showed non-caseat- ing granulomas, suggestive of sarcoidosis. Other granulo- Figure 1 MRI fl uid attenuated inversion recovery scans showed
matous diseases were ruled out by serological testing.
an area of hyperintense signal in the subcortical white matter of
Cranial MRI revealed large hyper dense areas on
the right temporal and occipital lobe as well as in the thalamus
T2-weighted images, located in the subcortical white mat-
BMJ Case Reports 2012; doi:10.1136/bcr.03.2011.4036
A stereotactic brain biopsy was performed, showing
mirtazapine has been used empirically showing improve-
neuropathological changes characteristic of PML, namely
focal white matter destruction with JCV-infected oli-
In summary, in HIV negative patients with PML as well
godendrocytes (as confi rmed by immunohistochemistry).
as in patients who are not receiving immunosuppressive
Laboratory tests revealed an elevated level of ACE,
therapy, no established treatment exists. The mechanisms
polyclonal gammopathy, a reduced lymphocyte count
leading to symptomatic PML in patients without a docu-
(600 cells/μl) and severely suppressed CD4+ lymphocyte
mented immune defect remain unknown. Considering
fraction (171 cells/μl), whereas the CD4+/CD8+ ratio was
the sarcoidosis as underlying cause we even discussed a
normal. No autoantibodies could be detected and HIV
treatment with immunosuppressive therapy to eventu-
infection was ruled out by repetitive screening, HIV RNA
ally improve the patient’s immune response. Because of
and p24 ag tests as well as a particle associated elevated
possibly aggravating JC-infection by this measurement
reverse transcriptase test to detect potential retroviral
we fi nally opted for a treatment with mirtazapine alone.
activity not detected by standard HIV tests.
Unfortunately, the patient experienced rapid deterioration after initiation of therapy and died 2 months later.
DIFFERENTIAL DIAGNOSIS
We describe a case of disseminated sarcoidosis with-
out prior immunosuppressive therapy and histologically proven symptomatic PML that did not respond to mirta-zapine therapy. The pathophysiologic mechanisms leading
TREATMENT
to PML in this case remain to be established.
A treatment with mirtazapine was initiated (15 mg/d). Clinically, and confi rmed by follow-up MRI of the brain 4 weeks after the initial imaging, no progression of the dis-
Learning points
ease was noted. Concerning sarcoidosis, the patient was asymptomatic apart from a slight restrictive ventilatory
▶ Whereas PML is well known in patients with
impairment. Corticosteroids were not administered.
AIDS and can also rarely occur in patients with immunosuppressive therapy such as for example,
OUTCOME AND FOLLOW-UP
natalizumab in patients with multiple sclerosis, in HIV-
Six weeks after diagnosis, the left-sided hemiparesis had
negative patients it is still a rare but serious disease.
worsened and the patient showed severe altered mental
▶ Sarcoidosis represents an atypical cause of PML
status and had suffered a generalised seizure.
because it is not necessarily associated with a
Progression of PML was confi rmed in a CT scan. Given the
classical immunosuppressive state or therapy, as
profound clinical deterioration no further treatment was under-
taken and the patient died 1 month later, that is, 2 months
▶ While treating HIV with antiretroviral therapy and
after diagnosis. Permission for autopsy was not granted.
removing immunosuppressive therapy represent therapeutic options in other cases, PML in sarcoidosis
DISCUSSION
is even more diffi cult to manage since there is no
The clinical and virological fi ndings and pathologic changes
specifi c treatment of JC-virus and immunosuppression
on neuroimaging in this patient were consistent with the
cannot be improved in this case of sarcoidosis.
diagnosis of PML, a brain biopsy ruled out other potentially
▶ PML is a differential diagnosis which has to be
treatable diseases. Simultaneously, our patient was found to
considered also in supposedly immunocompetent
have sarcoidosis stage III. PML in association with sarcoido-
patients for example, with sarcoidosis and neurological
sis has mostly been described in patients receiving immuno-
suppressive therapy, but cases of PML as fi rst manifestation in patients with sarcoidosis have rarely been reported. 1 2
There is no specifi c treatment for JCV infection. In HIV-
Acknowledgements The authors thank PD Dr Urs Schwarz, consultant in
positive patients with PML, highly active antiretroviral
Neurology, University Hospital Zurich, Switzerland and Professor Dr Hans Hirsch, University Hospital Basel, Switzerland for helpful discussions.
therapy is the best therapeutic option. In patients receiving immunosuppressive medication, a discontinuation or dose
Competing interests None. Patient consent Obtained.
Cytarabine has been shown to decrease JCV replication
invitro and appeared to stabilise the clinical status of HIV
REFERENCES
negative patients with PML. 3 Cidofovir alone or in com-
1. Rosenbloom MA, Uphoff DF . The association of progressive multifocal
bination with mirtazapine has been effective in vivo and
leukoencephalopathy and sarcoidosis. Chest 1983 ; 83 : 572 – 5 .
in cases of patients suffering from PML and sarcoidosis. 2
2. De Raedt S, Lacor P, Michotte A, et al . Progressive multifocal
leukoencephalopathy as fi rst manifestation of sarcoidosis. Clin Neurol
Nevertheless, several clinical studies have reported no ben-
Neurosurg 2008 ; 110 : 186 – 9 .
efi t from treatment with cidofovir. Mefl oquine is currently
3. Tan CS, Koralnik IJ . Progressive multifocal leukoencephalopathy and other
being evaluated in a multi-centre trial. 3
disorders caused by JC virus: clinical features and pathogenesis. Lancet
Since the 5-hydroxytryptamine-2a serotonin receptor
Neurol 2010 ; 9 : 425 – 37 .
4. Elphick GF, Querbes W, Jordan JA, et al . The human polyomavirus, JCV, uses
has been identifi ed as being a cellular receptor for JCV, 4
serotonin receptors to infect cells. Science 2004 ; 306 : 1380 – 3 . BMJ Case Reports 2012; doi:10.1136/bcr.03.2011.4036
This pdf has been created automatically from the fi nal edited text and images.
Copyright 2012 BMJ Publishing Group. All rights reserved. For permission to reuse any of this content visit http://group.bmj.com/group/rights-licensing/permissions. BMJ Case Report Fellows may re-use this article for personal use and teaching without any further permission.
Please cite this article as follows (you will need to access the article online to obtain the date of publication).
Hohlfeld SK, Günthard HF, Zeitz J, Locher P, Bachli E. Progressive multi-focal leukoencephalopathy as a rare lethal complication in untreated sarcoidosis. BMJ Case Reports 2012;10.1136/bcr.03.2011.4036, Published XXX
Become a Fellow of BMJ Case Reports today and you can:▶ Submit as many cases as you like▶ Enjoy fast sympathetic peer review and rapid publication of accepted articles▶ Access all the published articles▶ Re-use any of the published material for personal use and teaching without further permission
For information on Institutional Fellowships contact [email protected]
Visit casereports.bmj.com for more articles like this and to become a Fellow
Keep up to date with all published cases by signing up for an alert (all we need is your email address) http://casereports.bmj.com/cgi/alerts/etoc
BMJ Case Reports 2012; doi:10.1136/bcr.03.2011.4036
General Information for Coral Reef Ecology - 2008 Flight Information Departure We are leaving on TACA flight TA431on May 31, 2008 from Houston, Texas (Bush International IAH), which is scheduled to leave at 15:10. We will assemble at the TACA desk at 9:30 AM . Do not be late! Dr. Kesler already has enough gray hair. If there is an emergency, call Dr. Kesler’s cell phone at 901
Society of Nuclear Medicine Procedure Guideline for C-14 Urea Breath Test version 3.0, approved June 23, 2001 Authors: Helena R. Balon, MD (William Beaumont Hospital, Royal Oak, MI); Eileen Roff, RN, MSA, (William BeaumontHospital, Royal Oak, MI); John E. Freitas, MD (St. Joseph Mercy Hospital, Ann Arbor, MI); Vanessa Gates, MS (WilliamBeaumont Hospital, Royal Oak, MI); and Howard J. Dworkin,
 Unusual association of diseases/symptoms
Progressive multi-focal leukoencephalopathy as a rare lethal complication in untreated sarcoidosis
Sabine K Hohlfeld, 1 Huldrych F Günthard, 2 Jonas Zeitz,1 Pascal Locher, 1 Esther Bachli 3
1 Department of Internal Medicine, University Hospital Zurich, Zurich, Switzerland ; 2 Division of Infectious Diseases and Hospital Epidemiology, University Hospital Zurich, Zurich, Switzerland ; 3 Department of Internal Medicine, Uster Hospital, Uster, Switzerland
Correspondence to PD Dr Esther Bachli,
Unusual association of diseases/symptoms
Progressive multi-focal leukoencephalopathy as a rare lethal complication in untreated sarcoidosis
Sabine K Hohlfeld, 1 Huldrych F Günthard, 2 Jonas Zeitz,1 Pascal Locher, 1 Esther Bachli 3
1 Department of Internal Medicine, University Hospital Zurich, Zurich, Switzerland ; 2 Division of Infectious Diseases and Hospital Epidemiology, University Hospital Zurich, Zurich, Switzerland ; 3 Department of Internal Medicine, Uster Hospital, Uster, Switzerland
Correspondence to PD Dr Esther Bachli,