Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
No_452.pdf
Thai Journal of Obstetrics and Gynaecology June 2001, Vol.13, No.3, pp. 179-188
REVIEW
Leptin and female reproductive function Nares Sukcharoen MD.
Department of Obstetrics and Gynecology, Faculty of Medicine, Chulalongkorn University, Bangkok 10330, THAILAND
Abstracts
Leptin is mainly synthesized by adipocytes and might represent the connecting link
between fatty tissue and brain. It informs neuroendocrine pathways about the status of energy stores in adipose tissue. The integration of this peripheral signal in hypothalamic networks results in activation of peripheral pathways that control energy build-up and expenditure. It is also linked to a variety of reproductive processes in both animals and humans. The relationships between leptin and obesity, puberty, polycystic ovary syndrome, endometriosis, assisted fertility, and menopause are discussed. The role of leptin in fetal physiology and in normal and abnormal fetal growth as well as its role in diabetes, pregnancy, and pregnancy-induced hypertension are also reviewed.
Leptin is a protein produced mainly by adipose tissue and plays an important role in
the regulation of body weight and food intake.(1) Leptin suppresses the appetite, increases the metabolic rate and is correlated with fat mass.(2) It has been proposed to be involved in the control of the reproductive function and the pathophysiology of reproductive process e.g. anorexia nervosa, polycystic ovary syndrome (PCOS), etc.(3) The present review concentrates on the basic knowledge of letpin and its implication in the reproductive process. Leptin, leptin receptor and signal transduction
Leptin is a 16 kDa non-glycosylated polypeptide of 146 amino acids discovered in
1994.(4) Leptin (from Greek leptos : thin) is a product of the ob gene, 18 kb long(5), located in the long arm of chromosome 7 (7q31).(6) This gene encodes a 167 amino acids activated by cleavage of a 21 amino acid residues.(4) Three-dimensional structure of leptin resembles that of cytokines and lactogenic hormones.(7) It is produced mainly by adipose tissue(4), but also by placenta(8), stomach(9) and skeletal muscle.(10) It circulates in the blood (at concentrations paralleling the amount of fat reserves), and acts at the hypothalamic level as a satiety factor. Leptin circulates in biological fluids both as a free protein and in a form that is bound to the soluble isoform of its receptor (Ob-Re)(11). It has a half-life of 30 minutes.(12) Its secretion is pulsatile and shows a circadian rhythm, with a nocturnal rise reaching its peak between 1-2 a.m.(13) This pulsatile pattern is synchronized with that of luteinizing hormone (LH).(14) It is liberated as 3.6 pulses every 24 hours, usually 2 to 3 hours after meals. The main elimination route for leptin is via the kidney.(15)
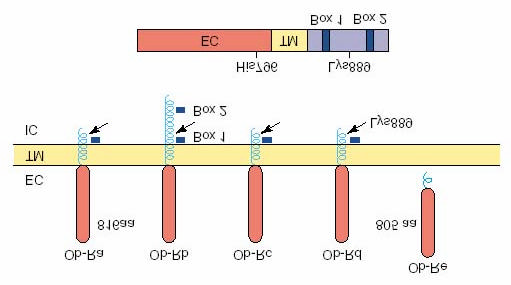
Leptin receptors are the products of the db gene and belongs to the class I cytokine
superfamily of receptors. It encodes a protein of variable length. Five different types of receptors have been identified, with ubiquitous locations among tissues, e.g., Ob-Ra, Ob-Rb, Ob-Rc, Ob-Rd, and Ob-Re.(16) (Figure 1) Only Ob-Rb contains a long intracellular domain and carries both of the protein motifs that are necessary for the activation of the Janus
kinase–signal transducers and activators of transcription (JAK–STAT) pathway. Ob-Rb is mainly expressed in the hypothalamus, and its expression is much lower in peripheral tissues, where the prevalent isoform is Ob-Ra.(17) Leptin receptors are found in many areas of the brain, including the hypothalamus, cerebellum, cortex, hippocampus, thalamus, choroid plexus, and brain capillary endothelium. Leptin receptors are also expressed in peripheral tissues, including the lung, kidney, liver, pancreas, adrenals, ovaries, hematopoietic stem cells, and skeletal muscle, whereas the soluble leptin receptor isoform that circulates in the serum functions as a leptin-binding protein.(18)
Fig. 1. Schematic representation of leptin receptor (Ob-R) isoforms. The gene encodes five different splice variants (Ob-Ra, Ob-Rb, Ob-Rc, Ob-Rd and Ob-Re). Only Ob-Rb contains both of the protein motifs (Box 1 and Box 2) that are capable of activating the Janus kinase (JAK)-signal transducers and activators of transcription (STAT) pathway. (aa : amino acids, EC : extracellular, IC : intracellular, TM : transmembrane)(17) Regulation of leptin synthesis and secretion
The regulation of leptin synthesis and secretion is dependent on multiple factors.
(Table 1) Women seem to have higher leptin levels than men.(19,20) The gender difference in leptin levels seems to be explained by differential effects of sex hormones, in particular an inhibition by testosterone, in addition to the differences in body composition, with women having more subcutaneous fat, secreting more leptin. Leptin levels increase exponentially with increasing fat mass(2), and leptin production is higher in subcutaneous fat than in visceral fat depot.(21) Table 1. Factors that influence leptin levels Decrease leptin levels Prolonged fasting(22) Isoproterenol, Somatostatin(23) Cigarette smoking(24) Thiazolidinediones(25) Metformin(26) Diazoxide(27) Increase leptin levels Fat mass(2) Overfeeding(28) Prolonged insulin infusions or supraphysiologic insulin levels (29-31) Glucocorticoid administration(32-34) Before puberty and at the onset of puberty(35,36) Estrogen(37)
During food excess, energy balance is usually positive, causing anabolic pathways to
be activated and glycogen synthesis and triglyceride deposit to occur. Such an energy state enhances leptin synthesis and liberation from adipocytes. Leptin receptors in hypothalamic arcuate nuclei induce a satiety state and augment energy expenditure with heat production.(38) In contrast, during starvation, a negative energy balance ensues with limited amounts of available substrates. Catabolic pathways are activated that generate glucose from glycogen, amino acids from proteins, and free fatty acids and glycerol from triglycerides. In this state, leptin synthesis and secretion are decreased, and the hypothalamus induces food-seeking behavior. This response is accompanied by a reduction in metabolic rate and heat-generating mechanisms. These changes enhance energy and substrate preservation in adverse conditions. (39) The role of leptin in female reproductive physiology
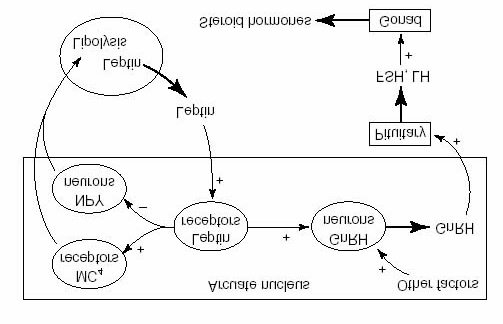
Leptin and adipose tissue are systemic modulators of the hypothalamus–pituitary–
gonadal (HPG) axis. (Figure 2) Leptin acts at multiple levels of the reproductive axis, eliciting different effects on reproduction depending on its concentrations in the blood. The saturable system of leptin transport through the blood–brain barrier prevents high levels of leptin reaching hypothalamic receptors, where leptin exerts stimulatory actions on gonadotropin-releasing hormone (GnRH) and in turn gonadotropin secretion. By contrast, excess levels of leptin have the potential to act on peripheral leptin receptors and exert inhibitory actions on testicular and ovarian steroidogenesis.
Fig. 2. Model for the dual roles of leptin in the regulation of adipose mass and reproduction. Leptin is secreted from adipocytes and finds its way to the arcuate region of the hypothalamus where it activates leptin-receptor-expressing neurons. Projections from these neurons will in turn stimulate melanocortin MC4 receptors and neuropeptide Y (NPY)- containing neurons to activate the sympathetic nervous system, which controls lipolysis in white adipose tissue. The firing of gonadotrophin releasing hormone (GnRH)-containing neurons and secretion of GnRH to the pituitary is elicited by leptin mediated activation of leptin-receptor-expressing neurons and by other factors, such as growth hormone (GH), NPY, insulin and others that control the reproductive axis. The ultimate consequences of leptin activation are the regulation of lipolysis and the firing of the reproductive system. This oversimplification does not show the projections of other neurons, which might impact on either pathway stimulated by leptin. Abbreviations: FSH, follicle-stimulating hormone; LH, luteinizing hormone.(40) Leptin in childhood and puberty
Because a critical threshold in fat mass has to be reached to initiate puberty and
maintenance of menstrual cycles and reproductive ability, leptin may be the signal from energy storage to the reproductive axis to elicit sexual development.(41,42) In normal children, leptin levels increase before puberty as body fat mass increases and reach their peak at the onset of puberty, suggesting that leptin may trigger puberty in humans.(36,43) In contrast, persons with inactivating mutations of the leptin receptor are morbidly obese, remain prepubertal, and have hypogonadotrophic hypogonadism.(44) However, leptin may not be essential to this process; puberty, sexual development, and pregnancy have been observed in patients with lipoatrophic diabetes.(45) Leptin levels during the menstrual cycle
Longitudinal studies have found a physiological fluctuation of leptin levels during the
menstrual cycle, with lower circulating leptin levels in the early follicular phase, an increase in leptin in the luteal phase of the cycle, and a pre-ovulatory peak in leptin.(46-48) It may increase in the follicular phase of superovulated cycles.(49) The changes in leptin are associated with changes in progesterone(46,47), estrogens(37,50) and LH.(13,51) It is important to be aware of this variation when studying leptin levels in women, in order to measure leptin at the same moment of the cycle. In women taking oral contraceptives, leptin levels remain unchanged throughout the cycle(52), but levels are not different from normally cycling females.(53) Leptin in menopause
It has been proposed that a decrease in leptin levels found at menopause was due to
the fall in estrogen levels.(54) However, most other studies found no differences in leptin levels between pre- and postmenopausal women, when matched for BMI.(19,53,55,56) Hormone replacement therapy (with estrogens and progesterone) does not seem to affect leptin levels in post-menopausal women either.(53,55,57,58) Leptin in female reproductive problems Leptin in polycystic ovarian disease
Women with the polycystic ovary syndrome (PCOS) are hyperandrogenic, with
increased plasma androstenedione and testosterone levels, are often characterized by visceral obesity, hyperinsulinaemia, insulin resistance, and anovulation. Leptin status in these women is not clear. Several studies found leptin levels in women with PCOS to be higher than expected for their BMI(59-61), but other studies found leptin levels comparable with age- and weight-matched control women.(62-64)
A possible explanation for these different findings could be that the phenotype of
PCOS can vary considerably, and that not all women with PCOS are to the same degree (abdominally) obese. The variability in leptin levels can possibly be explained in part by
differences in body composition. But even with similar leptin levels, the activity could differ in women with PCOS, for example by a different proportion of bound leptin circulating in the blood, differences in leptin pulsatility, or a reduced sensitivity of the hypothalamic-pituitary-ovary axis in women with PCOS.(65) Furthermore, recent data indicate that locally acting leptin may be more important than circulating leptin in the pathogenesis of the polycystic ovary syndrome and type 2 diabetes.(66,67)
To evaluate the importance of leptin in female fertility, serum and follicular fluid leptin
values have been measured in different categories of patients – women who succeeded (and women who failed) in becoming pregnant after assisted reproductive cycles, and patients with PCOS. It was found that lower follicular fluid leptin concentrations are a predictor of pregnancy success, both in normal women and in those with PCOS, possibly through direct ovarian actions resulting in impaired oocyte quality and/or early embryo development.(68,69) Leptin in endometriosis
Leptin levels in plasma and peritoneal fluid from patients who have endometriosis is
higher than normal women, especially peritoneal endometriosis. This may be due to its angiogenic activity and ability to modulate the immune response through receptors in T cells (CD4).(71-73) Leptin in eating disorders
Serum leptin levels in patients with anorexia nervosa, bulimia, nonspecific eating
disorders(74,75), and depression(76) are similar to those of healthy persons with comparable body mass index. However, decreased serum leptin was recently found to be associated with alterations in eating patterns, metabolic rate, and neuroendocrine regulation in bulimia nervosa.(77) Anorexia nervosa
In anorexia nervosa, severe undernutrition is associated with extremely low plasma
and cerebrospinal fluid leptin levels, low and apulsatile gonadotropins, altered menstrual function and amenorrhea.(78) Leptin values below 1.85 ng/ml have been found to associate with amenorrhea in underweight females with eating disorders(79); in addition, the resumption of menses is associated with leptin levels above this threshold. However, in underweight patients the rapid increment in serum leptin with weight gain is not concomitant with menstruation, which suggests that the normalization of menstrual periods might depend on additional factors such as the GH–insulin-like growth factor I (IGF-I) axis. These observations indicate that leptin values above a certain threshold might be necessary, but not sufficient, for the resumption of menses in anorexia nervosa patients.(80) Mutations of the genes encoding leptin and its receptor
Mutations of the genes encoding leptin and its receptor have also been found in
humans. In adult patients, homozygous missense mutations of the gene encoding the leptin receptor determine severe early-onset obesity, failure to enter puberty, primary amenorrhoea in females and clinical features of hypogonadism in males (no beard, scanty pubic and axillary hair, small penis and testes), with a prepubertal pattern of gonadotropin secretion.(81) The treatment of a nine-year-old patient with congenital leptin deficiency with recombinant leptin for 12 months led to a marked reduction in weight and fat mass, and the appearance of a nocturnal pulsatile secretory pattern of gonadotropins, which is characteristic of early puberty.(82) Similarly, female patients have been described who are homozygous for missense mutations in the db gene that encode a truncated leptin receptor lacking both the transmembrane and the intracellular domains. These patients do not spontaneously enter puberty, have no apparent mammary glands, sparse pubic hair and amenorrhoea, with low basal and human chorionic gonadotropin (hCG)-stimulated concentrations of estradiol, LH and folliclestimulating hormone (FSH). These data clearly indicate that correct signaling through Ob-R is necessary for sexual maturation in women.(83)
Leptin during pregnancy
During pregnancy, plasma leptin levels are elevated(84,85), rising especially during the
second trimester(86,87), and dropping sharply after delivery.(88) This increase is correlated with gestational weight gain, and absolute leptin levels are correlated with BMI.(85,86) This hyperleptinemia during pregnancy occurs with the appearance of a circulating form of the leptin receptor, functioning as a binding protein.(87) Another factor contributing to the rise in leptin levels is the production of leptin by placenta(8) and fetus (89), partly secreted into the maternal circulation.
During pregnancy, insulin levels are increased during pregnancy, and also gestational
hormones like human chorionic gonadotrophin and estrogen can stimulate leptin production by adipocytes. It is not clear whether leptin synthesized by placenta acts as a growth factor for the fetus or as a signal of energy status between mother and fetus. However, no correlation between maternal leptin levels and birth weight was found(86,90), in contrast to cord serum leptin concentrations and leptin levels in infants at birth, which are correlated with birth weight.(90,91) Female fetuses have higher levels than males. These differences persist until early neonatal life.(92) Leptin concentrations also correlate with weight gain.(93) Levels vary with time of day (higher in morning hours) and seasons (higher in spring and summer).(94) The drop in leptin levels seen after delivery could play a role in the reduced fertility during the period of lactation. Leptin in complicated pregnancy
Fetuses with intrauterine growth retardation have lower leptin levels due to a
reduction in fat tissue accretion. In insulin-dependent diabetic pregnancies, leptin receptors are increased as an expression of leptin resistance.(95) In pregnancy-induced hypertension, patients have higher leptin levels(96), and placental production of leptin is increased. Trophoblastic cells that were cultured under hypoxic conditions secreted more leptin than cultures in a normoxic environment. Leptin may be useful in the future as a marker of placental ischemia.(97) Leptin in the neonate
The level of leptin in cord blood derived from both the placenta and fetal tissues, is
positively associated with the body weight and fat mass of the neonate, decrease in response to maternal smoking, is lower in preterm infants and those who are small for gestational age, and is higher in those who are large for gestational age.(91,98) Apart from signaling energy reserves to the brain, leptin may regulate growth(99) and promote hematopoiesis and lymphopoiesis in newborn infants.(100,101) Infants of diabetic mothers(102) or those with a family history of obesity on the paternal side(94) also have higher leptin levels.
Immunoreactive leptin has been identified in human milk and in mammary epithelial
cells. It is well known that many cytokines and growth factors are present in human milk. Thus, it is possible that leptin plays a role in infant development and growth.(103,104)
In conclusions Leptin, an adipocyte-derived hormone known to play an important role
in body-weight regulation, has been shown to be expressed differentially in men and women. These observations are potentially important for the understanding of differences between men and women in regulation of food intake, weight gain, and body fat distribution. Leptin is also involved in female reproduction and pregnancy, especially a trigger of puberty, and might play a predominant role in conditions with abnormally low plasma concentrations, such as in subjects with very low BMI (anorexia nervosa) or in patients with homozygous mutations of the ob gene. Although the exact mechanisms and interactions with sex steroids are not yet fully established, it is clear that leptin plays a role as an endocrine mediator in sexual development, reproduction and pregnancy.
References 1. Messinis IE, Milingos SD. Leptin in human reproduction. Hum Reprod Update
2. Considine RV, Sinha MK, Heiman ML, Kraiauciunas A, Stephens TW, Nyce MR, et al.
Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N Engl J Med 1996;334:292-5.
3. Sabogal JC, Munoz L. Leptin in obstetrics and gynecology: a review. Obstet Gynecol
4. Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Positional cloning of
the mouse obese gene and its human homologues. Nature 1994;372:425-32.
5. Gong DW, Bi S, Pratley RE, Weintraub BD. Genomic structure and promoter analysis of
the human obese gene. J Biol Chem 1996;271:3971-4.
6. Green ED, Maffei M, Braden VV, Proenca R, DeSilva U, Zhang Y, et al. The human
obese (ob) gene: RNA expression pattern and mapping on the physical, cytogenetic, and genetic maps of chromosome 7. Genome Res 1995;5:5-12.
7. Kline AD, Becker GW, Churgay LM, Landen BE, Martin DK, Muth WL, et al. Leptin is a
four-helix bundle: secondary structure by NMR. FEBS Lett 1997;407:239-42.
8. Masuzaki H, Ogawa Y, Sagawa N, Hosoda K, Matsumoto T, Mise H, et al. Non-adipose
tissue production of leptin: leptin as a novel placenta derived hormone in humans. Nat Med 1997;3:1029-33.
9. Bado A, Levasseur S, Attoub S, Kermrgant S, Laigneau JP, Bortoluzzi MN, et al. The
stomach is a source of leptin. Nature 1998;394:790-3.
10. Wang J, Liu R, Hawkins M, Barzilai N, Rossetti L. A nutrient-sensing pathway regulates
leptin gene expression in muscle and fat. Nature 1998;393:684-8.
11. Sinha MK, Opentanova I, Ohannesian JP, Kolaczynski JW, Heiman ML, Hale J, et al.
Evidence for free and bound leptin in human circulation. Studies in lean and obese subjects and during short-term fasting. J Clin Invest 1996;98:1277-82.
12. Licinio J, Mantzoros C, Negrao AB, Cizza G, Wong ML, Bongiorno PB, et al. Human
leptin levels are pulsatile and inversely related to pituitary-adrenal function. Nat Med 1997;3:575-9.
13. Saad MF, Riad-Gabriel MG, Khan A, Michael R, Jinagouda SD, Boyadjian R, et al.
Diurnal and ultradian rhythmicity of plasma leptin: Effects of gender and adiposity. J Clin Endocrinol Metab 1998;83:453-9.
14. Licinio J, Negrao AB, Mantzoros C, Kaklamani V, Wong ML, Bongiorno PB, et al.
Synchronicity of frequently sampled, 24-h concentrations of circulating leptin, luteinizing hormone, and estradiol in healthy women. Proc Natl Acad Sci USA 1998;95:2541-6.
15. Cumin F, Baum HP, de Gasparo M, Levens N. Removal of endogenous leptin from the
circulation by the kidney. Int J Obes Relat Metab Disord 1997;231:495-504.
16. Tartaglia L, Dembski M, Weng X. Identification and expression cloning of a leptin
17. Caprio M, Fabbrini E, Isidori AM, Aversa A, Fabbri A. Leptin in reproduction. Trends
18. Auwerx J, Staels B. Leptin. Lancet. 1998;351:737-42. 19. Saad MF, Damani S, Gingerich RL, Riad-Gabriel MG, Khan A, Boyadjian R, et al. Sexual
dimorphism in plasma leptin concentration. J Clin Endocrinol Metab. 1997;82:579-84.
20. Ostlund RE Jr, Wang JW, Klein S, Gingerich R. Relation between plasma leptin
concentration and body fat, gender, diet, age, and metabolic covariates. J Clin Endocrinol Metab. 1996;81:3909-13.
21. Lonnqvist F, Nordfors L, Jansson M, Thorne A, Schalling M, Arner P. Leptin secretion
from adipose tissue in women. Relationship to plasma levels and gene expression. J Clin Invest 1997;99:2398-404.
22. Kolaczynski JW, Considine RV, Ohannesian J, Marco C, Opentanova I, Nyce MR, et al.
Responses of leptin to short-term fasting and refeeding in humans. Diabetes. 1996;45:1511-5.
23. Donahoo WT, Jensen TR, Yost TJ, Eckel RH. Isoproterenol and somatostatin decrease
plasma leptin in humans: a novel mechanism regulating leptin secretion. J Clin Endocrinol Metab 1997;82:4139-43.
24. Mantzoros CS, Liolios AD, Tritos NA, Kaklamani VG, Doulgerakis DE, Griveas I, et al.
Circulating insulin concentrations, smoking and alcohol intake are important independent predictors of leptin in young healthy men. Obes Res. 1998;6:179-86.
25. Kallen CB, Lazar MA. Antidiabetic thiazolidinediones inhibit leptin (ob) gene expression in
3T3-L1 adipocytes. Proc Natl Acad Sci USA. 1996;93:5793-6.
26. Morin-Papunen LC, Koivunen RM, Tomas C, Ruokonin A, Martikainen HK. Decreased
serum leptin concentrations during metformin therapy in obese women with polycystic ovary syndrome. J Clin Endocrinol Metab 1998;83:2566-8.
27. Krassas GE, Kaltsas TT, Pontikides N, Jacobs H, Blum W, Messinis I. Leptin levels in
women with polycystic ovary syndrome before and after treatment with diazoxide. Eur J Endocrinol 1998;139:184-9.
28. Kolaczynski JW, Ohannesian JP, Considine RV, Marco CC, Caro JF. Response of leptin
to short-term and prolonged overfeeding in humans. J Clin Endocrinol Metab 1996;81:4162-5.
29. Utriainen T, Malmstrom R, Makimattila S. Yki-Jarvinen H. Supraphysiological
hyperinsulinemia increases plasma leptin concentrations after 4 h in normal subjects. Diabetes 1996;45:1364-6.
30. Ryan AS, Elahi D. The effects of acute hyperglycemia and hyperinsulinemia on plasma
leptin levels: its relationships with body fat, visceral adiposity, and age in women. J Clin Endocrinol Metab 1996;81:4433-8.
31. Malmstrom R, Taskinen MR, Karonen SL, Yki-Jarvinen H. Insulin increases plasma leptin
concentrations in normal subjects and patients with NIDDM. Diabetologia 1996;39:993-6.
32. Miell JP, Englaro P, Blum WF. Dexamethasone induces an acute and sustained rise in
circulating leptin levels in normal human subjects. Horm Metab Res 1996;28:704-7.
33. Larsson H, Ahren B. Short-term dexamethasone treatment increases plasma leptin
independently of change in insulin sensitivity in healthy women. J Clin Endocrinol Metab 1996;81:4428-32.
34. Papaspyrou-Rao S, Schneider SH, Petersen RN, Fried SK. Dexamethasone increases
leptin expression in humans in vivo. J Clin Endocrinol Metab 1997;82:1635-7.
35. Garcia-Mayor RV, Andrade MA, Rios M, Lage M, Dieguez C, Casanueva FF. Serum
leptin levels in normal children: relationship to age, gender, body mass index, pituitary-gonadal hormones, and pubertal stage. J Clin Endocrinol Metab 1997;82:2849-55.
36. Mantzoros CS, Flier JS, Rogol AD. A longitudinal assessment of hormonal and physical
alterations during normal puberty in boys. V. Rising leptin levels may signal the onset of puberty. J Clin Endocrinol Metab. 1997;82:1066-70.
37. Mannucci E, Ognibene A, Becorpi A, CremascoF, Pellegrini S, Ottanelli S, et al.
Realtionship between leptin and oestrogens in healthy women. Eur J Endocrinol 1998;139:198-201.
38. Cusin I, Zakrzewska KE, Boss O, Muzzin P, Giacobino JP, Ricquier D, et al. Chronic
central leptin infusion enhances insulin-stimulated glucose metabolism and favors the expression of uncoupling proteins. Diabetes 1998;47:1014-9.
39. Magni P, Motta M, Martini L. Leptin. A possible link between food intake, energy
expenditure, and reproductive function. Regul Pept 2000;92:51-6.
40. Chehab FF. Leptin as a regulator of adipose mass and reproduction. Trends Pharmacol
41. Rosebaum M, Leibel RL. Role of gonadal steroids in the sexual dimorphisms in body
composition and circulating concentrations of leptin. J Clin Endocrinol Metab 1999;84:1784-9.
42. Hassink SG, Sheslow DV, de Lancey E, Opentanova I, Considine RV, Caro JF. Serum
leptin in children with obesity: relationship to gender and development. Pediatrics. 1996;98:201-3.
43. Garcia-Mayor RV, Andrade MA, Rios M, Lage M, Dieguez C, Casanueva FF. Serum
leptin levels in normal children: relationship to age, gender, body mass index, pituitary-gonadal hormones, and pubertal stage. J Clin Endocrinol Metab 1997;82:2849-55.
44. Clement K, Vaisse C, Lahlou N, Cabrol S, Pelloux V, Cassuto D, et al. A mutation in the
human leptin receptor gene causes obesity and pituitary dysfunction. Nature. 1998;392:398-401.
45. Andreelli F, Hanaire-Broutin H, Laville M, Tauber JP, Riou JP, Thivolet C. Normal
reproductive function in leptin-deficient patients with lipoatropic diabetes. J Clin Endocrinol Metab 2000;85:715-9.
46. Hardie L, Trayhurn P, Abramovich D, Fowler P. Circulating leptin in women: a longitudinal
study in the menstrual cycle and during pregnancy. Clin Endocrinol 1997;47:101-6.
47. Riad-Gabriel MG, Jinagouda SD, Sharma A, Boyadjian R, Saad MF. Changes in plasma
leptin during the menstrual cycle. Eur J Endocrinol 1998;139:528-31.
48. Paolisso G, Rizzo MR, Mazziotti G, Rotondi M, Tagliamonte MR, Varricchio G, et al. Lack
of association between changes in plasma leptin concentration and in food intake during the menstrual cycle. Eur J Clin Invest 1999;29:490-5.
49. Messinis IE, Milingos S, Zicopaulos K, et al. Leptin concentrations in the follicular phase
of spontaneous cycles and cycles superovulated with follicle stimulating hormone. Hum Reprod 1998;13:1152-6.
50. Shimizu H, Shimomura Y, Nakanishi Y, Futawatari T, Ohtani K, Sato N, et al. Estrogen
increases in vivo leptin production in rats and human subjects. J Endocrinol 1997;154:285-92.
51. Teirmaa T, Luukkaa V, Rouru J, Koulu M, Huupponen R. Correlation between circulating
leptin and luteinizing hormone during menstrual cycle in normal weight women. Eur J of Endocrinol 1998;139:190-4.
52. Cella F, Giordano G, Cordera R. Serum leptin concentrations during the menstrual cycle
in normal-weight women: effects of an oral triphasic estrogen±progestin medication. Eur J Endocrinol 2000;142:174-8.
53. Castracane VD, Kraemer RR, Franken MA, Kraemer GR, Gimpel T. Serum leptin
concentration in women: effect of age, obesity, and estrogen administration. Fertil Steril 1998;70:472-7.
54. Rosenbaum M, Nicholson M, Hirsch J, Heymsfield SB, Gallagher D, Chu F, et al. Effects
of gender, body composition and menopause on plasma concentrations of leptin. J Clin Endocrinol Metab 1996;81:3424-7.
55. Haffner SM, Mykkanen L, Stern MP. Leptin concentrations in women in the San Antonio
Heart Study: effect of menopausal status and postmenopausal Hormone Replacement Therapy. Am J Epidemiol 1997 146 581-5.
56. Sumner AE, Falkner B, Kushner H, Considine RV. Relationship of leptin concentration to
gender, menopause, age, diabetes, and fat mass in African Americans. Obesity Research 1998;6:128-33.
57. Kohrt WM, Landt M, Birge SJ. Serum leptin levels are reduced in response to exercise
training, but not hormone replacement therapy, in older women. J Clin Endocrinol Metab 1996;81:3980-5.
58. Baumgartner RN, Waters DL, Morley JE, Patrick P, Montoya GD, Garry PJ. Age-related
changes in sex hormones affect the sex difference in serum leptin independently of changes in body fat. Metabolism 1999;48:378-84.
59. Brzechffa PR, Jakimiuk AJ, Agarwal SK, Weitsman SR, Buyalos RP, Magoffin DA. Serum
immunoreactive leptin concentrations in women with Polycystic Ovary Syndrome. J Clin Endocrinol Metab 1996;81:4166-9.
60. Vicennati V, Gambineri A, Calzoni F, Casimirri F, Macor C, Vettor V, et al. Serum leptin in
obese women with polycystic ovary syndrome is correlated with body weight and fat distribution but not with androgen and insulin levels. Metabolism 1998;47:988-92.
61. Micic D, Macut D, Popovic V, Sumarac-Dumanovic M, Kendereski A, Colic M, et al.
Leptin levels and insulin sensitivity in obese and non-obese patients with polycystic ovary syndrome. Gynecol Endocrinol 1997;11:315-20.
62. Mantzoros CS, Dunaif A, Flier JS. Leptin concentrations in the Polycystic Ovary
Syndrome. J Clin Endocrinol Metab 1997;82:1687-91.
63. Laughlin G, Morales A, Yen S. Serum leptin levels in women with polycystic ovary
syndrome: the role of insulin resistance/hyperinsulinemia. J Clin Endocrinol Metab 1997;82:1692-6.
64. Rouru J, Anttila L, Koskinen P, Penttila T-A, Irjala K, Huupponen R, et al. Serum leptin
concentrations in women with Polycystic Ovary Syndrome. J Clin Endocrinol Metab 1997;82:1697-700.
65. Caro JF. Leptin is normal in PCOS - an editorial about three ‘negative’ papers. J Clin
66. Spicer LJ, Francisco CC. The adipose obese gene product, leptin: evidence of a direct
inhibitory role in ovarian function. Endocrinology 1997;138:3374-9.
67. Zachow RJ, Magoffin DA. Direct intraovarian effects of leptin: impairment of the
synergistic action of insulin-like growth factor-I on follicle-stimulating hormone-dependent estradiol-17 beta production by rat ovarian granulosa cells. Endocrinology 1997;138:847-50.
68. Mantzoros CS, Cramer DW, Liberman RF, Barbieri RL. Predictive value of serum and
follicular fluid leptin concentration during assisted reproductive cycles in normal women and in women with the polycystic ovarian syndrome. Hum Reprod 2000;15:539-44.
69. Brannian JD, Schmidt SM, Kreger DO, Hansen KA. Baseline non-fasting serum leptin
concentration to body mass index ratio is predictive of IVF outcomes. Hum Reprod 2001;16:1819-26.
70. Matarese G, Alviggi C, Sanna V, Howard JK, Lord GM, Carravetta C, et al. Increased
leptin levels in serum and peritoneal fluid of patients with pelvic endometriosis. J Clin Endocrinol Metab 2000;85:2483-7.
71. Matalliotakis IM, Koumantaki YG,Neonaki MA, Goumenou AG, Koumantakis GE,
Kyriakou DS, et al. Increase in serum leptin concentrations among women with endometriosis during danazol and leuprolide depot treatments. Am J Obstet Gynecol 2000;183:58-62.
72. De Placido G, Alviggi C, Carravetta C, Pisaturo ML, Sanna V, Wilding M, et al. The
peritoneal fluid concentration of leptin is increased in women with peritoneal but not ovarian endometriosis. Hum Reprod 2001;16:1251-4.
73. Gogacz M, Polak G, Jakowicki J, Kotarski J. Peritoneal fluid leptin concentration in
infertile patients. J Reprod Immunol 2001;51:159-65.
74. Grinspoon S, Gulick T, Askari H, Landt M, Lee K, Anderson E, et al. Serum leptin levels
in women with anorexia nervosa. J Clin Endocrinol Metab 1996;81:3861-3.
75. Ferron F, Considine RV, Peino R, Lado IG, Dieguez C, Casanueva FF. Serum leptin
concentrations in patients with anorexia nervosa, bulimia nervosa and non-specific eating disorders correlate with the body mass index but are independent of the respective disease. Clin Endocrinol 1997;46:289-93.
76. Deuschle M, Blum WF, Englaro P, Schweiger U, Weber B, Pflaum CD, et al. Plasma
leptin in depressed patients and healthy controls. Horm Metab Res 1996;28:714-7.
77. Jimmerson DC, Mantzoros C, Wolfe BE, Metzger ED. Decreased serum leptin in bulimia
nervosa. J Clin Endocrinol Metab 2000;85:4511-4.
78. Mantzoros C, Flier JS, Lesem MD, Brewerton TD, Jimerson DC. Cerebrospinal fluid
leptin in anorexia nervosa: correlation with nutritional status and potential role in resistance to weight gain. J Clin Endocrinol Metab 1997;82:1845–51.
79. Kopp W, Blum WF, von Prittwitz S, Ziegler A, Lubbert H, Emons G, et al. Low leptin
levels predict amenorrhea in underweight and eating disordered females. Mol Psychiatry 1997;2:335–40.
80. Audi L, Mantzoros CS, Vidal-Puig A, Vargas D, Gussinye M, Carrascosa A. Leptin in
relation to resumption of menses in women with anorexia nervosa. Mol Psychiatry 1998;3:544–7.
81. Strobel A, Issad T, Camoin L, Ozata M, Strosberg AD. Aleptin missense mutation
associated with hypogonadism and morbid obesity. Nat Genet 1998;18:213–5.
82. Farooqi IS, Jebb SA, Langmack G, Lawrence E, Cheetham CH, Prentice AM, et al.
Effects of recombinant leptin therapy in a child with congenital leptin deficiency. N Engl J Med 1999;341:879-84.
83. Clement K, Vaisse C, Lahlou N, Cabrol S, Pelloux V, Cassuto D, et al. A mutation in the
human leptin receptor gene causes obesity and pituitary dysfunction. Nature 1998;392:398-401.
84. Butte N, Hopkinson J, Nicholson M. Leptin in human reproduction: serum leptin levels in
pregnant and lactating women. J Clin Endocrinol Metab 1997;82:585-9.
85. Highman T, Friedman J, Huston L, Wong W, Catalano P. Longitudinal changes in
maternal serum leptin concentrations, body composition, and resting metabolic rate in pregnancy. Am J Obstet Gynecol 1998;178:1010-5.
86. Tamas P, Sulyok E, Szabo I, Vizer M, Ertl T, Rascher W, et al. Changes of maternal
serum leptin levels during pregnancy. Gynecol Obstet Invest 1998;46:169-71.
87. Tamura T, Goldenberg R, Johnston K, Cliver S. Serum leptin concentrations during
pregnancy and their relationship to fetal growth. Obstet Gynecol 1998;91:389-95.
88. Matsuda J, Yokota I, Iida M, Murakami T, Yamada M, Saijo T, et al. Dynamic changes in
serum leptin concentrations during the fetal and neonatal periods. Pediatr Res 1999;45:71-5.
89. Lepercq J, Challier JC, Guerre-Millo M, Cauzac M, Vidal H, Hauguel-de Mouzon S.
Prenatal leptin production: evidence that fetal adipose tissue produces leptin. J Clin Endocrinol Metab 2001;86:2409-13.
90. Lewandowski K, Horn R, O'Callaghan CJ, Dunlop D, Medley GF, O'Hare P, et al. Free
leptin, bound leptin, and soluble leptin receptor in normal and diabetic pregnancies. J Clin Endocrinol Metab 1999;84:300-6.
91. Schubring C, KiessW, Englaro P, RascherW, Dotsch J, Hanitsch S, et al. Levels of leptin
in maternal serum, amniotic fluid, and arterial and venous cord blood: relation to neonatal and placental weight. J Clin Endocrinol Metab 1997;82:1480-3.
92. Jaquet D, Leger J, Levy-Marchal C, Oury JF, Czernichow P. Ontogeny of leptin in
human fetuses and newborns: Effect of intrauterine growth retardation on serum leptin concentrations. J Clin Endocrinol Metab 1998;83:1243-6.
93. Harigaya A, Nagashima K, Nako Y, Morikawa A. Relationship between concentration of
serum leptin and fetal growth. J Clin Endocrinol Metab 1997;82:3281-4.
94. Tarquini B, Tarquini R, Perfetto F, Cornelissen G, Halberg F. Genetic and environmental
influences on human cord blood leptin concentration. Pediatrics 1999;103:998-1006.
95. Lewandowski K, Horn R, O’Callaghan CJ, Dunlop D, Medley GF, O’Hare P, Brabant G.
Free leptin, bound leptin and soluble leptin receptor in normal and diabetic pregnancies. J Clin Endocrinol Metab 1999;84:300-6.
96. MacCarthy JF, Misra DN, Roberta JM. Maternal plasma leptin is increased in
preeclampsia and positively correlates with fetal cord concentration. Am J Obstet Gynecol 1999;180:731-6.
97. Mise H, Sagawa N, Matsumoto T, Yura S, Nanno H, Itoh H, et al. Augmented placental
production of leptin in preeclampsia: Possible involvement of placental hypoxia. J Clin Endocrinol Metab 1998;83:3225-9.
98. Mantzoros CS, Varvarigou A, Kaklamani VG, Beratis NG, Flier JS. Effect of birth weight
and maternal smoking on cord blood leptin concentrations of full-term and preterm newborns. J Clin Endocrinol Metab 1997;82:2856-61.
99. Carro E, Senaris R, Considine RV, Casanueva FF, Dieguez C. Regulation of in vivo
growth hormone secretion by leptin. Endocrinology 1997;138:2203-6.
100. Bennett BD, Solar GP, Yuan JQ, Mathias J, Thomas GR, Matthews W. A role for
leptin and its cognate receptor in hematopoiesis. Curr Biol 1996;6:1170-80.
101. Mikhail AA, Beck EX, Shafer A, Barut B, Gbur JS, Zupancic TJ, et al. Leptin
stimulates fetal and adult erythroid and myeloid development. Blood 1997;89:1507-12.
102. Gross GA, Solemberg T, Philpott T, Holcomb WL Jr, Landt M. Plasma leptin
concentrations in newborns of diabetic and nondiabetic mothers. Am J Perinatol 1998;15:243-7.
103. Smith-Kirwin SM, O’Connor DM, Johnston J, Lancey ED, Hassink SG, Funanage VL.
Leptin expression in human mammary cells and breast milk. J Clin Endocrinol Metab 1998;83:1810-4.
104. Casabiell X, Pineiro V, Tome MA, Peino R, Dieguez C, Casanueva FF. Presence of
leptin in colostrum and/or breast milk from lactating mothers: a potential role in the regulation of neonatal food intake. J Clin Endocrinol Metab 1997;82:4270-3.
Sicherheitsdatenblatt gemäß 1907/2006/EG/Artikel 31 1 Bezeichnung des Stoffs bzw. des Gemischs und des Unternehmens · Produktidentifikator · Handelsname: Tretinoin Tretinoinum · Artikelnummer: · CAS-Nummer: · EINECS-Nummer: · Relevante identifizierte Verwendungen des Stoffs oder Gemischs und Verwendungen, von denen abgeraten · Verwendung des St
(Incorporated in the Republic of South Africa)Notice is hereby given that the ninth annual general meeting of shareholders (“AGM”) of Lewis Group Limited for the year ended 31 March 2013 will be held at Lewis Group head office, 53A Victoria Road, Woodstock, Cape Town at 08:30 on Friday, 16 August 2013. registration will start at 08:00. The board of directors of the Company determined that
 kinase–signal transducers and activators of transcription (JAK–STAT) pathway. Ob-Rb is mainly expressed in the hypothalamus, and its expression is much lower in peripheral tissues, where the prevalent isoform is Ob-Ra.(17) Leptin receptors are found in many areas of the brain, including the hypothalamus, cerebellum, cortex, hippocampus, thalamus, choroid plexus, and brain capillary endothelium. Leptin receptors are also expressed in peripheral tissues, including the lung, kidney, liver, pancreas, adrenals, ovaries, hematopoietic stem cells, and skeletal muscle, whereas the soluble leptin receptor isoform that circulates in the serum functions as a leptin-binding protein.(18)
kinase–signal transducers and activators of transcription (JAK–STAT) pathway. Ob-Rb is mainly expressed in the hypothalamus, and its expression is much lower in peripheral tissues, where the prevalent isoform is Ob-Ra.(17) Leptin receptors are found in many areas of the brain, including the hypothalamus, cerebellum, cortex, hippocampus, thalamus, choroid plexus, and brain capillary endothelium. Leptin receptors are also expressed in peripheral tissues, including the lung, kidney, liver, pancreas, adrenals, ovaries, hematopoietic stem cells, and skeletal muscle, whereas the soluble leptin receptor isoform that circulates in the serum functions as a leptin-binding protein.(18)
 Decrease leptin levels
Decrease leptin levels