Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
89nu7006003
[99mTc]TRODAT-1 Evaluation of ear ly Par kinson’s Disease with [99mTc]TRODAT- 1/SPECT Imaging
The etiology of idiopathic Parkinson’s disease (PD) is unknown. There is no
effective method to prevent the occurrence of this neurodegenerative disorder at the
present time. The most important and practical approach to the management of these
patients is to make the diagnosis at an early stage and introduce an intervention that
protects the vulnerable neurons and slows or stops disease progression.
The major neuropathological feature in (PD) is severe degeneration of the
dopamine (DA) neurons in the substantia nigra. Dopamine transporter (DAT) is an
important protein in the presynaptic uptake sites which is important in terminating
synaptic dopamine action and maintaining dopamine homeostasis Specific binding to
dopamine transporters may serve as a tool to detect early loss of nigrostriatal
dopaminergic neurons in patients with Parkinson's disease.
Recently, single photon emission computed tomography (SPECT) imaging of
-CIT is shown to be an alternative to positron
emission tomography (PET) or postmortem studies for in vivo evaluation of
presynaptic dopaminergic function. However, the production of [123I] is limited by
the availability of cyclotron, which makes its routine clinical application difficult.
The staff of INER (Institution of Nuclear Energy Research, Taiwan) has the honor to
work with Dr. Kung and is permitted to produce domestic [99mTc] TRODAT-1, a
highly selective and safe dopamine transporter ligand.
The aim of this study is to investigate striatal DAT binding in early PD with
[99mTc]TRODAT-1 and single photon emission computed tomography (SPECT). SUBJ ECTS
Twenty-six sequential patients with early untreated Parkinson's disease (Hoehn
and Yahr stages I [n = 10] and II [n = 16] [symptom duration, <2 years]; mean age,
63.2 years; range, 36-83 years) who gave the informed consent were recruited. We
followed the inclusion and exclusion criteria set by the CAPIT committee for clinical
diagnosis of PD. Patients who had psychiatric disorders, alcohol or substance abuse,
or unstable medical problems were also excluded. Written informed consent was
obtained from each patient. This study was approved by the institutional review
board of National Cheng Kung University Hospital.
The basic demographic data, mean duration of illness, co-morbid factors and
Unified Parkinson’s Disease Rating Scale (UPDRS) motor subscore were collected
in each patient. Every patient received [99mTc]TRODAT-1/SPECT and brain magnetic
resonance imaging (MRI) at the beginning of this study and a second [99mTc]
TRODAT-1/SPECT one year later after Selegiline 5 mg PO bid. Patients who
suffered from severe resting tremor and had the potential for seriously degrading
image quality were given midazolam 15 mg 30 min before MRI and [99mTc]
TRODAT-1/SPECT study. The second UPDRS motor subscore will be done at the
time of the second [99mTc] TRODAT-1/SPECT study.
The primary response variable is the averaged right and left striatum/occipital
lobe ratios. The secondary response variables are the changes in UPDRS motor
subscore and the time interval from randomization to the need of starting or adding
Preparation of Tc-99m TRODAT-1 Injection Descr iption
Each 10 ml vial contained a pre-dispensed sterile, non-pyrogenic, lyophilized
g TRODAT-1⋅3HCl (2-[[2-[[[3-(4-chlorophenyl) -8-methyl -8-
azabicyclo [3.2.1] oct-2-yl] methyl](2-mercaptoethyl) amino]-ethyl]-amino] ethane-
thiolato (3-)-N2, N2’, S2, S2’) oxo- [1R-(exo-exo) hydrogen chloride], 320
g Na ·EDTA·2H O (disodium ethylenediamine
g stannous chloride dihydrate, 20 mg mannitol, 4.1 mg
anhydrous sodium phosphate dibasic and 460
sealed under nitrogen atmosphere with a rubber plug. No bacteriostatic preservative
Gener al Pr epar ation Precautions:
1. A technetium Tc-99m generator was eluted within 24 hours prior to obtaining
any eluate for reconstitution with the INER TRODAT-1 kit.
2. Only sterile 0.9% sodium chloride without bacteriostatic preservative was
allowed to be used for dilution of Tc-99m before reconstitution. Procedure for the Pr epar ation of Technetium Tc-99m TRODAT-1 Injection
1. We placed one vial in a suitable shielding container and disinfected the rubber
plug with an alcoholic sterile swab.
2. Using a 10-mL syringe, we injected into the shielded vial 5 mL of sterile eluate
(1.11~1.48 MBq) from a technetium Tc-99m generator. Before withdrawing the
syringe from the vial, we drew 5 mL of gas from the space above the solution to
normalize the pressure in the vial. The shielded vial was put upside down for 10
seconds to ensure complete dissolution of the contents.
for 30 min to complete the labeling.
4. Following cooling to room temperature, we assayed the total radioactivity and
calculated the volume to be injected.
5. The pH of the prepared injection was 6.5~7.5. Tc-99m TRODAT-1/SPECT Imaging
A dose of 25 mCi of [99mTc] TRODAT-1 was injected intravenously into each
patient. The binding to dopamine transporter was assessed 4 hours after injection
with SPECT. A rotating three-headed gamma camera with fan-beam collimator
(Multi SPECT 3, Siemens, Germany) and a commercially available computer system
were used for data acquisition and processing. Data were collected for 120
projections (360o rotation) in a 128 × 128 matrix. The acquisition time was 40
seconds per projection. Attenuation correction was performed in selected transverse
slices according to a modified Chang’s method. In-plane resolution of the
reconstructed images was 8.5 mm FWHM, and slice thickness was approximately 6
MRI Image
1. T1-weighted axial and sagittal , proton density axial, and T2-weighted axial and
coronal MRI images were obtained by a Magneton 1.5 Tesla scanner (Siemens,
Iselin, NJ). The slice thickness was 3 mm at the level of basal ganglia.
2. Regions of interest (ROI) template derived from co-registered MRI image were
used for analyzing [99mTc]TRODAT-1 activity within the neostriatum. SPECT Quantitative Conventional semiquantitation
The right and left striatum activity in all reconstructed transaxial slices was
summed as total volume activity, and then was divided by total areas as average
activity. The striatum activity was further divided into caudate, and lenticular nucleus
according to the finely adjusted ROI on MRI image registration. The occipital lobe
was chosen for comparison. An elliptical ROI was drawn on occipital lobe in the
transverse slice with striatum activity. The ratio of striatum to occipital lobe was then
New automated quantitative method
A new quantitative method developed by our group in the first year project was
applied to this study (See Quantification of D2-receptor imaging with [123I] IBZM
and Single Photon Emission Tomography; N87-2218-E-006-065-NU. Statistical Analysis
Both the primary and secondary response variables in either group were
S.D. Two-tailed Student’s t-test was applied for comparison
and values of p<0.05 were considered significant.
In patients with early PD, the striatum/occipital ratio was reduced as compared
with normal controls. The decrease was more prominent in the tail of putamen
compared with caudate nucleus. (Figure 1). Striatal TRODAT-1 binding was
significantly reduced in patients with early Parkinson's disease not only
contralaterally to the more severely affected side, but also in the normal or mildly
disturbed side (Figure 2). The striatum/occipital ratio in patients with early PD was
significantly reduced in contralateral striatum (1.73
0.25; range, 1.35-2.19; p = 0.003) (Figure 3)
Striatum/occipital ratios were lower in patients with Hoehn and Yahr stage II
and Yahr stage I (contralateral striatum: 1.80
0.24). However, the difference is not statistically significant (p = 0.324 and 0.185,
respectively) (Figure 4). Twenty-one patients (patient 1-21) showed a more
decreased striatum/occipital ratio on the side contralateral to clinically worse side.
One case (patient 22) showed equal activity bilaterally. Only 4 patients (patient 23-26)
showed a more decreased activity on the ipsilateral side (Figure 5). There is no
significant decline of striatum/occipital ratio with age in early PD, both in ipsilateral
striatum (Figure 6) and contralateral striatum (Figure 7). Striatum/occipital ratios
were not significantly correlated with the severity of clinical symptoms-UPDRS
We found a bilateral decrease of striatum activity in early PD patients, even in
stage 1 PD patients whose clinical symptoms were unilateral. This finding indicates
that [99mTc]TRODAT-1/SPECT imaging is able to detect early subclinical PD patients.
With its clinical availability, [99mTc]TRODAT-1/SPECT imaging is suitable for
clinical screening of high risk patients. In addition, we found that [99mTc]TRODAT-
1/SPECT imaging showed a more decreased or equal striatum/occipital lobe uptake
ratio contralateral to clinically worse side in 85% of the studied patients. These
findings are consistent with previous [18F]DOPA/PET and autopsy reports. Our
preliminary results suggest that [99mTc]TRODAT-1/SPECT imaging is a useful tool
for detecting presynaptic dopaminergic dysfunction. There is a great overlap of
striatum activity between stage I and stage II PD. It is not surprise to expect this
finding, since the clinical differentiation is not clear. We are planning to follow up
these patients longitudinally with both [99mTc] TRODAT-1 and [123I] IBZM/SPECT to
observe the sequential changes of dopamine transporter and receptor in striatum.
This may detect underlying the rate of progression of PD and provide the scientific
explanation for the development of motor fluctuation in late stage PD patients.
There is no correlation between UPDRS motor subscore and the
striatum/occipital ratio. This might imply that clinical evaluation with UPDRS may
not reflect the true status of dopaminergic neurons in the substantia nigra. The items
for tremor evaluation account for more than one-fifth of the total motor subscore
(24/108). As we know, the severity of tremor shows marked fluctuation in a short
period of time and is aggravated by anxiety, nervousness, or any factors increasing
sympathetic activity. Another explanation for the discrepancy between UPDRS
motor subscore and the striatum/occipital ratio is the labeling efficiencies of [99mTc]
TRODAT-1 are different among patients. This hypothesis has been tested and we do
not find significant influence of labeling efficiency on the striatum/occipital ratio.
In early PD, there is apparent reduction of activity in bilateral putamen, while
the activity in caudate nucleus is preserved. For those patients at stage
unilateral symptoms the striatum uptake of [99mTc] TRODAT-1 was decreased
bilaterally, which means [99mTc] TRODAT-1 SPECT is capable to detect pre-clinical
Parkinson’s disease, and has the potential for screening of pre-clinical Parkinson’s
patients. We are planning to collect more data of normal controls as comparable age
groups. This is important for the interpretation of subtle change for any age-matched
individual. We will continue on the protocol to work out if selegiline has
neuroprotective effect after treatment for 1 year. The use of [99mTc] TRODAT-
1/SPECT imaging for differentiating different categories of parkinsonism will also be
tested in the near future. Finally, the TRODAT-1 kit produced by INER is safe and
easy for clinical use. None of the patients reports side effects in this study.
In conclusion, [99mTc] TRODAT-1/SPECT demonstrates a reduction of
dopamine transporter binding in patients with early Parkinson's disease. Significantly
reduced TRODAT-1 binding already observed in the ipsilateral striatum of patients
with Hoehn and Yahr stage I and II demonstrates the potential of this method to
Fig 1. The striatum uptake of [99mTc] TRODAT-1 in normal control and early PD. There is decreased striatum uptake in early PD with
more prominent in the tail of putamen than in caudate nucleus. Fig 2. The striatum uptake of [99mTc] TRODAT-1 in stage I and stage II PD. The patient with stage I PD had unilateral right side
symptoms, while [99mTc] TRODAT-1 SPECT shows a slight decrease of striatum uptake on contralateral side. The patient with
stage II PD had mild left side symptoms and worse on right side. [99mTc] TRODAT-1 SPECT shows a marked decrease of
striatum uptake on contralateral side and a slight decrease on ipsilateral side. Fig 3. The striatum/occipital ratio in patients with early PD was significantly reduced in contralateral striatum (1.73
1.34-2.10) than in ipsilateral striatum (1.80
ip tal Ratio c c ia tr Striatum / S Fig 4. Striatum/occipital ratios in contralateral striatum and ipsilateral striatum in patients with Hoehn and Yahr stage II and Hoehn and
Yahr stage I. The difference is not statistically significant (p = 0.324 and 0.185, respectively)
ip ctal Ratioc
Fig 5. The [99mTc] TRODAT-1 SPECT findings show an excellent correlation with the asymmetry of clinical symptoms, i.e. 21/26 of
patients (81%)show a more decreased striatum / occipital ratio on the side contralateral to the clinically worse side, 1/26 showed
equal uptake bilaterally. Only 4/26 patients showed a more decreased striatum / occipital ratio on the ipsilateral side
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Fig 6. Striatum/occipital ratio in ipsilateral striatum in early PD. There is no significant decline of striatum uptake with age. Fig 7. Striatum/occipital ratio in contralateral striatum in early PD. There is no significant decline of striatum uptake with age. Fig 8. Correlation between striatum/occipital ratios and the severity of clinical symptoms (UPDRS-motor subscore) UPDRS-motor subscore
Jaber M, Jones S, Giros B, et al: The dopamine transporter: a crucial component
regulating dopamine transmission. Mov Disord 1997;12:629-33.
Lesch KP, Balling U, Seemann M, et al: Molecular heterogeneity of
neurotransporters: implications for neurodegeneration. In: Mizuno Y, et al, eds. Advances in Research on Neurodegeneration (volume 3 & 4). Austria: Springer-
Mitilineou C, Radcliffe P, Leonardi EK, et al: L-deprenyl protects
mesencephalic dopamine neurons from glutamate receptor-mediated toxicity. J
Mytilineou C, Cohen G: Deprenyl protects dopamine neurons from the
effect of 1-methyl-4-phenyl-pyridinium ion. J Neurochem
Roy E, Bedard PJ: L-deprenyl increases survival of rat fetal nigral neurones in
culture. Neuroreport 1993;4:1183-6.
Shoulson I: Where do we stand on neuroprotection ? Where do we go from
here ? Mov Disord 1998;13(Suppl 1):46-8.
Burns RS, Chiueh CC, Markey SP, et al: A primate model of parkinsonism:
selective destruction of dopaminergic neurons in the pars compacta of the
substantia nigra by N-methyl-4-phenyl-1,2,3,6-tetrahydropyridine. Proc Natl Acad Sci 1983;80:4546-50.
Chalmers-Redmond RME, Fraeser AD, Ju WYH, et al: Mechanisms of nerve
cell death: apoptosis or necrosis after cerebral ischemia. In: Green AR, Cross AJ
eds. Neuroprotective agents and cerebral ischemia 1996:1-25.
Olanow CW, Mytilineou C, Tatton W: Current status of selegiline as a
neuroprotective agent in Parkinson’s disease. Mov Disord 1998;13(Suppl 1):55-
10. Vingerhoets FJG, Snow BJ, Lee CS, et al: Longitudinal fluorodopa positron
emission tomographic studies of the evolution of idiopathic parkinsonism. Ann
11. Morrish PK, Sawle GV, Brooks DJ: An [18F]dopa-PET and clinical study of the
rate of progression in Parkinson’s disease. Brain 1996;119:585-91.
12. Fahn S, Clarence-Smith KE, Chase TN: Workshop report: Parkinson’s disease:
neurodegenerative mechanisms and neuroprotective interventions-report of a
workshop. Mov Disord 1998;13:759-67.
13. Ishikawa T, Dhawan V, Kazumata K, et al: Comparative nigrostriatum
FDOPA/PET. J Nucl Med 1996;37:1760-5.
14. Seibyl JP, Msrek K, Innis RB: SPECT imaging of dopamine nerve terminals. Am J Psychiatry 1996;153:1131.
15. Kung MP, Stevenson DA, Plossl K, et al: [99mTc]TRODAT-1: a novel
technetium-99m-complex as a dopamine transporter imaging agent. Eur J Nucl
16. Seibyl JP, Marek KL, Quinlan D, et al: Decreased single-photon emission
-CIT striatum uptake correlates with symptom
severity in Parkinson’s disease. Ann Neurol 1995;38:589-98.
17. Innis RB: Single-photon emission tomography imaging of dopamine terminal
innervation: a potential clinical tool in Parkinson’s disease. Eur J Nucl Med
18. Innis RB, Seibyl JP, Scanley BE, et al: Single photon emission computed
tomographic imaging demonstrates loss of striatum dopamine transporters in
Parkinson’s disease. Proc Natl Acad Sci 1993;90:11965-9.
19. Wenning GK, Donnemiller E, Granata R, et al: 123I-
SPECT scanning in levodopa-naïve Parkinson’s disease. Mov Disord 1998;
20. Dresel SHJ, Kung MP, Plossl K, et al: Pharmacological effects of dopaminergic
drugs on in vivo binding of [99mTc]TRODAT-1 to the central dopamine
transporters in rats. Eur J Nucl Med 1998;25:31-9.
21. Meegalla SK, Plossl K, Kung MP, et al: Synthesis and characterization of
technetium-99m-labeled tropanes as dopamine transporter-imaging agents. J
22. Kung HF, Kim HJ, Kung MP, et al: Imaging of dopamine transporters in
humans with technetium-99m TRODAT-1. Eur J Nucl Med 1996;23:1527-30.
23. CAPIT committee: Core Assessment Program for Intracerebral Transplantations
(CAPIT). Mov Disord 1992;7:2-13.
24. Parkinson Study Group: DATATOP: A multicenter controlled clinical trial in
early Parkinson’s disease. Arch Neurol 1989; 46: 1052-60.
25. Kao PF, Tzen KY, Yen TC. Et al. The optimal imaging time for
[99Tcm]TRODAT-1/SPET in normal subjects and patients with Parkinson's
disease. Nucl Med Commun. 2001 Feb;22(2):151-4.
26. Yen TC, Lu CS, Tzen KY. et al. Decreased dopamine transporter binding in
Machado-Joseph disease. J Nucl Med. 2000 Jun;41(6):994-8.
4 Sidhu, A.B. et al. (2002) Chloroquine resistance in Plasmodium15 Mehlotra, R.K. et al. (2001) Evolution of a unique Plasmodiumfalciparum malaria parasites conferred by pfcrt mutations. Sciencefalciparum chloroquine-resistance phenotype in association withpfcrt polymorphism in Papua New Guinea and South America. Proc. 5 Sanchez, C.P. et al. (2003) Trans stimulation provides evidence for aNa
Appendix 22 Guidance for Staff on Medicines used to Treat Common Conditions This guidance is designed to inform and support staff to understand the basic medicines used in their work. The following points apply to all medications that are administered to people 1 Medication can only be given to people by staff who have received and successfully completed level 1 and 2 training, and hav

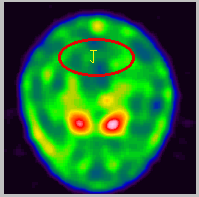 Fig 1. The striatum uptake of [99mTc] TRODAT-1 in normal control and early PD. There is decreased striatum uptake in early PD with
Fig 1. The striatum uptake of [99mTc] TRODAT-1 in normal control and early PD. There is decreased striatum uptake in early PD with
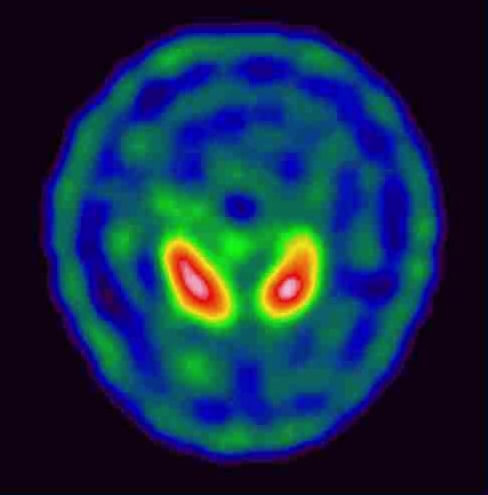 Fig 2. The striatum uptake of [99mTc] TRODAT-1 in stage I and stage II PD. The patient with stage I PD had unilateral right side
Fig 2. The striatum uptake of [99mTc] TRODAT-1 in stage I and stage II PD. The patient with stage I PD had unilateral right side