Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Pii: s0899-9007(98)00063-x
REVIEW ARTICLE
Compatibility and Stability of Additives in
MICHAEL C. ALLWOOD, PHD, AND MELANIE C. J. KEARNEY, PHD
From the Medicines Research Unit, University of Derby, Mickleover, Derby, United Kingdom
The addition of additives (electrolytes, trace elements, and vitamins) to parenteral nutrition (PN) mixtures can lead to
precipitation as a result of physical incompatibilities and can lead to chemical degradation of individual ingredients. The mostsignificant cause of precipitation is excessive concentrations of calcium phosphate. The most significant cause of chemicalinstability is the oxidation of specific vitamins. The factors influencing calcium phosphate solubility include the commercialamino acid source, the calcium and phosphate salts used, temperature, magnesium concentration, and final volume. Precipitationcan be avoided by organic phosphates. Trace element precipitation is most commonly caused by the formation of iron phosphatesalts or copper cysteinate in cysteine-containing amino acid infusions. The least stable nutrient is ascorbic acid, which reacts withoxygen, and is catalyzed by copper ions. Oxygen originates from PN ingredients, the filling process, air remaining in the bag afterfilling, and oxygen permeation through the bag wall. Storage in multilayered bags with reduced gas permeability can protectresidual ascorbic acid. Other chemical losses are caused by the reduction of thiamine by metabisulfite, and photodegradation ofdaylight-sensitive vitamins, especially retinol and riboflavin, during administration. Nutrition 1998;14:697–706. Elsevier
Key words: parenteral nutrition, additives, electrolytes, trace elements, vitamins, precipitation, chemical degradation
viewed include electrolytes, trace elements, and vitamins. Mech-anisms to avoid these unfavorable reactions are considered.
The compounding of parenteral nutrition (PN) admixtures in
large volume plastic containers (“big bags”) leads inevitably to
infusions that are less stable than the constituent components. Theindividual injections used in the compounding of any mixture are
All PN regimens must contain a range of essential electrolytes,
manufactured as relatively stable products with shelf-lives mea-
some of which must be included within a particular concentration
sured in years. Stability is maintained by optimizing both the
range (for example potassium and sodium coincident with theclinical condition of the patient), whereas others must be present
formulation and packaging of the products. Once each injection or
in amounts at least sufficient to provide a minimum daily require-
infusion has been removed from its original container and mixed
ment (for example calcium, magnesium, and phosphate). Individ-
with other parenteral ingredients, the chemical stability of the
ual patient requirements depend on a number of factors, such as
active ingredients and also any excipients will be compromised. In
clinical condition, age, renal function, and their level of physical
addition, the mixing of various compounds may lead to loss of
activity. Electrolytes in PN mixtures normally retain their chem-
physical compatibility by formation of new salts of low aqueous
ical status, although certain electrolytes can cause physical incom-
solubility compared with constituent chemical components, lead-
The monovalent ions do not pose any significant physical
It is the purpose of this review to consider the possible causes
compatibility problems, and high concentrations are generally
for chemical degradation and physical incompatibility in PN ad-
tolerated in PN mixtures. In contrast, precipitation can derive from
mixtures that involve parenteral additives, and to relate the sig-
di- and trivalent ion interactions, in particular calcium and phos-
nificance of these changes to clinical consequences.
phate. Although, in practice, normal daily requirements for adults
For the purpose of this review, the parenteral additives re-
can be included in PN mixtures without causing precipitation,
Correspondence to: Professor M. C. Allwood, PhD, Medicines Research Unit, University of Derby, Mickleover, Derby DE3 5GX, UK. E-mail:[email protected]
Nutrition 14:697–706, 1998Elsevier Science Inc. 1998
Printed in the USA. All rights reserved.
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
FIG. 1. Speciation of inorganic phosphate in parenteral nutrition mixtures.
physical incompatibilities can arise in attempting to achieve the
largely determined by the concentrations of arginine, histidine,
greater daily needs of children and neonates due to the low final
volume (i.e., highly concentrated) typically delivered. An under-standing of the causes of calcium phosphate precipitation can lead
The amino acid concentration in the final mixture.3,6,7
to compounding strategies that maximize the amounts of calcium
will depend on both the amino acid concentration in the original
and phosphate ions that can be added safely to PN mixtures.
infusion and the total volume of the PN mixture, which results inaltering the buffering capacity (increasing the final amino acid
Factors Influencing Calcium Phosphate Compatibility in Total
concentration enhances buffering capacity and vice versa).
In aqueous solutions containing phosphate salts, an equilib-
The type and final concentration of phosphate injection.
rium will be established between the three ionic phosphate spe-
organic phosphate additives are available as a mixture of mono-
cies; the trivalent phosphate ion and its monobasic (H POϪ) and
and dibasic salts with either sodium and potassium as the counter
dibasic (HPOϪ) forms (Fig 1). The pKa values for the two
ion, producing formulations that form strong buffers with pH
equilibria give an indication of the predominant phosphate species
values in the range of 5.0 – 6.5. This pH depends on the ratio of the
at any particular solution pH. The tribasic phosphate species will
two phosphate ions. Alternatively, a monobasic phosphate injec-
not normally be present in PN admixtures because of the extreme
tion can be used, containing, for example, potassium dihydrogen
alkalinity necessary for it to become ionized. Both mono- and
phosphate. The pH of this injection is approximately 5.0. This
dibasic phosphate salts may form a salt with calcium, but the
monobasic phosphate injection can therefore be used to enhance
dibasic salt is the least soluble of the two options. The solubility
the amounts of phosphate and calcium that can be added to total
of the monobasic and dibasic calcium salts are 1.8 and 0.03% w/v,
parenteral nutrition (TPN) mixtures without causing precipita-
respectively.1 For example, at physiologic pH (7.4), approxi-
tion,3,6,8 due to its pH-lowering effect.
mately 60% according to calculations based on the Henderson-Hasselbach equation of the phosphate is in the dibasic form.
Because the dibasic calcium phosphate salt is poorly soluble, this
tion, can reduce the pH of the final PN mixture.
enhances the probability of calcium phosphate precipitation. By
The final concentration of glucose.2
decreasing the pH by 2 U, approximately 95% of the phosphate is
sions are acidic, the buffering capacity of the amino acid infusion
in the monobasic form,1 which is far more soluble. The most
and phosphate additive will predominate as controllers of final pH.
important factor, therefore, governing calcium phosphate compat-
Many other factors influence the physical compatibility of
ibility in any PN mixture is the final pH of the mixture. This will
calcium and phosphate salts in PN mixtures. No single factor can
be determined by range of a factors.
be seen in isolation and the final outcome will be a result of a
These factors that determine the final pH are, in order of
The second important factor effecting calcium phosphate sol-
The commercial source of the amino acid infusion.2–4
ubility is the final concentration of free calcium ion,1,2,6,8,9 because
acid infusions from different manufacturers vary in pH between
the formation of the poorly soluble dibasic phosphate salt is
around approximately 5.0 and 7.4. In addition, each amino acid
dependent on the equilibrium between phosphate and calcium
mixture will vary in buffering capacity (titratible acidity).2 This is
ions. Calcium ion concentration depends on a number of factors:
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
Calcium additives are available as inorganic
phate has also been reported to be effective in providing adequate
salts (calcium chloride) or organic compounds (calcium gluconate
requirements of the two elements in infants.15
or gluceptate). Calcium chloride reduces the solubility of calciumphosphate complexes in PN mixtures compared with calcium
gluconate or gluceptate, because the chloride salt dissociates to a
It has been reported that precipitates may form either during
greater extent.1,9 The two organic salts show similar degrees of
the mixing process or after some time has lapsed after compound-
dissociation, and there appears, therefore, to be no advantage in
ing, referred to as time-mediated precipitation.9 These variations
usage between these two compounds in PN mixtures.1 Organic
relate to the chemistry of the system. A precipitate formed during
salts should be the preferred source of calcium. Calcium gluconate
the compounding process due to poor mixing and layering of
injection is, however, commonly contaminated with aluminum
different ingredients comprises calcium phosphate, whereas the
and a recent study10 indicates it is contra-indicated for use in
time-mediated precipitate is normally caused by dibasic calcium
phosphate crystallization. Although the first type appears as awhite flocculent amorphous precipitate, the latter is identified as
Temperature has a major influence on calcium
semitransparent and well-defined crystals, commonly adhering to
phosphate solubility, in particular if organic calcium salts are
the sides of the container.7,9 In any case, precipitates once formed
employed. This is because temperature effects the dissociation of
are highly unlikely to redissolve.16 Formation of the latter may
the organic calcium salts1,2,8,11 and possibly the equilibria between
take up to 24 – 48 h at 37°C,6 depending on the relative concen-
the different phosphate species.2 Raising temperature causes a
trations of calcium and phosphate salts.
greater dissociation of calcium gluconate to free calcium. This issignificant if temperatures rise from 5 to 37°C. Second, raising the
temperature of a mixture may also shift the phosphate equilibrium
The formation of calcium phosphate precipitates can be iden-
from mono- to dibasic salt. Both effects increase the likelihood of
tifiable by visual inspection, and this approach has been employed
by most investigators. A number of other methods have beenapplied in different studies to identify, in particular, critical points
in the solubility matrix of PN mixtures. These can be categorized
plexation between calcium and specific amino acids has been
as methods to detect particulates or methods to quantify calcium
reported.2,9 Computer simulations have suggested the relative
or phosphate solution concentration changes. Methods to detect
degree of complexation with different amino acids. The amino
particulates include light or electron microscopic examination of
acid most likely to complex with calcium is lysine, although
filter surfaces after filtration of the PN mixture3,11 for particulate
glutamic and aspartic acids, arginine, and histidine also form
counts. Methods to quantify concentration changes include cal-
complexes.9 The degree of complexation is also pH-dependent.9
cium concentration measurement by atomic absorption spectros-
Cysteine, in contrast, shows very low levels of calcium
copy, potentiometric titration,6 or spectrophotometry.1
No method provides complete confidence in ensuring detection
The final concentration of magnesium.
of all incompatible mixtures. The use of relatively simple meth-
the likelihood of precipitation because it forms relatively more
ods, such as visual examination with appropriate illumination and
soluble and stable salts with phosphate ions.4 This effect increases
background, the data from which are then used to construct
with pH. It also depends on the molar ratio of calcium and
solubility diagrams, are probably as reliable as a general screening
magnesium. Ratios of magnesium/calcium less than two exert a
method as the more technical and time-consuming methods used
positive effect on calcium phosphate solubility.4,9
by some laboratories. Particle counting with laser light extinctioncan detect particles down to 1.75 m, as they can be suspended
Other factors have also been reported to influ-
during the analysis with a magnetic stirring bar. Particles have
ence the final outcome. The order of mixing can affect the final
been detected even with time-mediated precipitate formation
solubility profile of calcium phosphate.1,4 The phosphate additive
when sampled at different time intervals. Particle counts, however,
should always be added and the mixture thoroughly mixed before
will only detect precipitation if the particles are suspended in the
adding calcium. An alternative approach has been reported that
mixture, and this may not be the case with time-mediated precip-
also enhances calcium and phosphate additions. Kaminski et al.12
itate formation in which some solid material may adhere to con-
found that mixing the two salts into separate infusions (phosphate
tainer surfaces. Microscopic examination of filter surfaces follow-
into the amino acid, calcium into the glucose) and combining these
ing the isolation of particles by filtration of PN mixtures is
mixtures slowly reduced the likelihood of precipitation.
relatively sensitive but is time-consuming and again depends on
Factors such as the time of storage before administration may
particle suspension before filtration. Particle counts will also not
be significant. Experience indicates that calcium phosphate pre-
differentiate between calcium phosphate microcrystallization and
cipitates do not necessarily form immediately but may take up to
other particles present in the mixture. Filters must also be made
transparent and often the particles may coalesce to form a “carpet”
Finally, it is worth noting that PN mixtures generally have a
on the filter surface, which is difficult to identify. Only electron
greater capacity for phosphate than for calcium ions.6
microscopical x-ray energy dispersive spectroscopy (EDX) anal-ysis, a highly specialized technique, will confirm the presence of
calcium and phosphate in isolated precipitates.17
One method of avoiding the risk of calcium phosphate precip-
Compatibility Assessment of Calcium Phosphate in All-in-One
itation is to use organic phosphate compounds. The disodium salts
of glucose 1-phosphate, glycerophosphate, and arginine glucose
The rate and spectrum of calcium phosphate particulate for-
1-phosphate have been employed. These compounds have been
mation is very different from flexible lipid droplet enlargement
reported to be fully compatible in a range of PN mixtures, and to
(fat emulsion instability). In the case of calcium phosphate par-
be at least equally bioavailable when compared with inorganic
ticulate formation, calcium phosphate precipitates when formed
phosphate,9,13,14 although some dissociation or degradation to
show dramatic increases in the number and size spectrum, whereas
release phosphate ions cannot be ignored. Calcium glycerophos-
in the case of flexible lipid droplet enlargement, enlargement of fat
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
globules is slow, such that the number and size gradually increase
or manganese as contaminants, in some cases significantly con-
from one sampling interval to the next. These characteristics, in
tributing to final concentrations in PN mixtures, an observation
terms of particle growth, may help discern calcium phosphate
also reported by Kartinos,22 who noted that amino acid infusions
from coalesced lipid droplets in these opaque formulations. The
may contain detectable quantities of iron, cobalt, manganese,
technical aspects of this differentiation are difficult and require
molybdenum, fluorine, and iodine. The compatibility of zinc,
further study. Precipitation in all-in-one mixtures cannot readily
manganese, copper, chromium, and iodine in TPN mixtures after
be detected by visual inspection, due to the fat emulsion.18 Light
24 h of storage at ambient temperature or 4°C has been confirmed
microscopy has been employed18 to detect crystalline precipita-
(by M.C.A.). In a longer-term storage study, it has been shown
tion, although the limit of detection with regard to particle size is
that zinc, copper, manganese, and chromium are compatible and
5 m. The sensitivity of the microscopic method was not deter-
stable in PN mixtures containing one particular amino acid source
mined. An alternative approach is to evaluate the compatibility of
(Synthamin, Baxter, Baxter Health Care, Ltd., Wallingford, UK)
the mixture with the exclusion of the fat emulsion, and test for
for 4 mo at 2– 6°C.24 It was, however, noted that copper showed
incompatibility in the normal manner. Because removal of the fat
some evidence of physical incompatibility in Synthamin alone, but
emulsion will reduce the volume and hence increase the concen-
not in PN mixtures containing Synthamin, even after only 2 d
tration of each ingredient, it can be argued that in such an ap-
storage. Copper precipitates have also been recovered from PN
proach the mixture tested is at least as likely to precipitate as the
mixtures containing Novamine as the amino acid source.25 It was
same mixture with fat emulsion. However, this makes the assump-
hypothesized that the precipitate consisted of copper sulfide, due
tion that increasing the concentration of other ingredients does not
to reaction with cysteine.26 A more recent study has also noted
significantly enhance calcium phosphate solubility. This may not
copper and sulfur ions present on in-line filters after delivery of
be true for amino acids, for example. It also assumes that the
PN mixtures containing Vamin (Pharmacia & Upjohn Ltd., Milton
emulsion does not influence calcium phosphate compatibility. The
alternative, therefore, is to replace the fat emulsion with an equiv-
Precipitation of iron added to PN mixtures has been reported.28
This appeared to relate to a specific amino acid infusion used tocompound the mixture. It has been reported that iron dextran28 and
ferrous citrate29 are compatible in PN mixtures, although the study
The recent US incidences have highlighted the consequences
periods were related to infusion times (18 –24 h) only.
of infusing precipitates such as calcium phosphate.15 Knowles et
The stability of selenium has also received some attention
al.19 report a case of pulmonary deposition of calcium phosphate
since Levander30 reported that high concentrations of ascorbic
crystals in a patient on home PN. The patient developed diffuse
acid reduced the soluble selenite ion to insoluble elemental sele-
granulomatous interstitial pneumonitis after approximately a 14-d
nium. This reaction may be further enhanced by the high reduction
infusion of PN. The cause was directly linked to calcium phos-
potential of other cations, such as the cuprous ion. Shils and
phate deposition in the lung. Calcium phosphate precipitation has
Levander31 reported that ascorbic acid 5 g/L induced significant
also been identified as a cause of blocking in-dwelling catheters
selenite reduction, but McGee et al.32 noted that PN mixtures
through which PN was being administered.19
containing 1 g/L ascorbic acid did not cause loss of selenium in
The Federal Drug Administration (FDA) has now recom-
solution, even after extended periods of storage up to 10 wk. A
mended that in-line filters should be used in all TPN administra-
later report indicated that reduction of selenite was only detected
tion to avoid calcium phosphate precipitates entering the patient.15
if the pH of the TPN mixture was Յ 5.0. In mixtures with pH
This recommendation applies to non-fat containing and all-in-one
Ͻ 5.0 ascorbic acid at concentrations as low as 100 mg/L could
cause selenite reduction to elemental selenium.32 It would there-fore appear that reduction of selenite to free selenium is not likely
to occur in PN mixtures, provided the pH remains Ͼ 5.0. Allwood
A wide range of trace elements are necessary to meet the
and Greenwood17 reported evidence of selenium precipitation in
nutritional needs of patients receiving PN. The list of recognized
PN mixtures containing ascorbic acid, after deliberately reducing
requirements has grown with our increasing knowledge of micro-
the pH to Ͻ 5.0, using EDX to analyze filters for precipitated
nutrient functions in nutrition. The list includes such elements as
selenium after filtration of stored PN mixtures.
selenium, molybdenum, chromium, and bromine, as well as the
Other potential losses of trace elements, including, for exam-
more obvious iodine, fluorine, manganese, and copper. Daily
ple, reduction of iodide to iodine, have not been reported in
requirements remain, in many cases, poorly defined, although both
practice, although Allwood and Greenwood17 reported that cal-
the minimum and maximum amounts are defined for most ele-
cium phosphate precipitates in TPN mixtures also contained evi-
ments, because both clinical evidence of deficiencies and toxic
dence of other phosphate salts, including iron and manganese.
levels have become evident (e.g., manganese). There are twoaspects to be considered with regard to the stability of trace
elements in PN mixtures. First, assurance is required that each
The risk of calcium phosphate precipitation is the major prob-
element is chemically stable, and second, that each element is
lem regarding the addition of electrolytes and trace elements to PN
physically compatible with other ingredients. The very low con-
mixtures. The mechanisms and consequences are now well rec-
centrations used in PN mixtures pose analytical challenges to
ognized. Clear strategies are available to avoid this physical in-
determine both of these aspects. This probably accounts for the
compatibility. The most promising development is the availability
fact that there is a sparsity of information on trace element
of organic phosphate injections that provide a means of avoiding
stability and compatibility in PN mixtures.
any risk associated with calcium phosphate precipitation. Our
Investigations into the stability of trace element additives to
limited knowledge of trace element stability in PN mixtures sug-
PN mixtures have, in most studies, relied on analysis of specific
gests that incompatibilities are generally avoided in compounded
trace element concentrations by atomic absorption spectroscopy.
mixtures, and that extended shelf-lives can be assigned to many
Zinc, copper, manganese, and chromium were reported to be
mixtures containing trace elements. However, until further evi-
stable and compatible in PN mixtures for 48 h at ambient tem-
dence is available, caution is necessary when extending shelf-lives
perature, and after passage through a 0.45 m in-line filter.21,22 It
of untested PN mixtures, in particular those with high levels of
was also noted that certain PN ingredients contained copper, zinc,
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
tion.35–38 Photolysis proceeds both in the bag and during passage
Vitamins are commonly believed to be among the least stable
ingredients in PN mixtures, and it is generally recommended that
A light-protecting overwrap to the container and the use of
vitamins be added immediately before commencing infusion or
special light-protecting administration sets is therefore commonly
that infusion should be commenced within 24 – 48 h of addition.
recommended,40 unless the patient is being fed in a position away
This constraint poses severe limitations on the ability of com-
from strong daylight or at night.36 Administration in a room with
pounding units to provide aseptically prepared complete PN mix-
only artificial lighting will lead to minimum degradation. It should
tures. A careful consideration of the stability of vitamins is crucial
also be noted that fat emulsion will protect retinol from photoly-
to the operation of safe and effective compounding services.
sis,32,41 both in the big bags and during infusion, although direct
Stability must be considered in the context of both storage after
sunlight may penetrate the emulsion sufficiently to cause some
compounding and during administration, because some vitamins
can undergo degradation during administration. With the increas-
Sorption of retinol has been reported,39,42 and has also lead to
ing demand for extended storage of complete PN mixtures, espe-
clinical manifestations of vitamin deficiency in long-term PN
cially for home patients, investigation of vitamin stability during
feeding.39 It was shown that substantial amounts of retinol (ace-
storage has become an important development in contributing to
tate) in PN mixtures prepared in glass bottles was lost by absorp-
improving the quality of patient care.
tion to the administration set during simulated infusion.31,39 In
Various vitamins are known to be degraded under particular
contrast, other studies have been unable to confirm retinol binding
conditions and in the presence of specific PN ingredients. The
to plastic bags or sets.36,37 Further investigations have confirmed
major physico-chemical considerations are exposure to light, the
that sorption to PVC depends on the ester used. Whereas the
type of plastic used to manufacture the PN container and infusion
acetate ester (used in most US-manufactured products) binds
equipment, and storage temperature. The chemical parameters of
strongly to PVC bags and administration sets, with losses up to
concern relate to the oxidation or reduction of particular vitamins.
90% being reported,39 the palmitate ester commonly used by
European manufacturers shows no evidence of binding to plasticsused to store and administer PN, in either two-in-one35,43 or
Vitamins most sensitive to photolysis are retinol (vitamin A)
and riboflavin (B ). The nature of the light is extremely important,
because it is exclusively the ultraviolet (UV) component thatcauses chemical photolysis of vitamins.34,35 Most artificial light
sources, including fluorescent light, contain insignificant emis-
All fat emulsions contain some tocopherol, although it will be
sions in the UV range. It is therefore only daylight exposure that
present as a mixture of isomers, some of which are more biolog-
causes serious photolytic losses in practice. Photolysis during
ically active than others.45 However, the proportions of the iso-
storage should be readily avoidable.
mers vary widely, both between batches of the same product, and
Tocopherol appears to be relatively stable in PN mixtures.
The vitamin most liable to bind with plastics is retinol. How-
Billion-Rey et al.37 reported that this vitamin was stable for 20 d
ever, only the acetate ester form has been shown to exhibit
at 4°C, with or without fat emulsion. Dahl et al.35 reported that
sorption to polyvinyl chloride (PVC) bags and administration
total tocopherol in all-in-one PN mixtures was stable for 6 d at
2– 8°C and during simulated infusion over 24 h in normal room
illumination conditions. However, the relative proportions of thedifferent isomers was not assessed.
Chemical degradation is the most important cause of vitamin
Kishi et al.46 reported that tocopherol was stable during sim-
losses in PN mixtures. Although many vitamins are likely to
ulated infusion in PN mixtures, both with and without light-
degrade eventually after addition to TPN mixtures, two particular
protective measures. McGee et al.32 monitored the stability of
reactions are of major concern: the oxidation of ascorbic acid and
␣-tocopherol (5 IU in a 2.5-L mixture) in PN mixtures exposed to
the reduction of thiamine, being the most readily oxidized and
fluorescent light at room temperature in the bag and during sim-
ulated infusion through in-line filters. No significant losses were
The stability of all vitamins added to TPN mixtures will be
reported. No losses were reported by Dahl et al.35 during simu-
considered, both during storage and administration.
lated infusion in fat emulsion. Kishi et al.46 reported similar results
after 24-h storage, although McKenna and Bieri47 reported a 10%loss during infusion. Billion-Rey et al.37 reported that tocopherol
was stable during exposure to sunlight for up to 8 h. In contrast,
Multivitamin additives intended for PN may contain either the
Gillis et al.48 reported that only 63% of the added ␣-tocopherol
acetate or palmitate ester of retinol. The former compound is
was delivered during administration of the PN mixture (monitored
commonly used in formulations originating from the USA.
using a radioactively labeled vitamin source). Drott et al.49 also
The stability of retinol in PN mixtures during storage has been
reported some loss during simulated infusion, amounting to ap-
widely reported. Allwood35 has shown that retinol (palmitate) is
proximately 10% during 20 h of administration. The role of light
stable in two-in-one mixtures for at least 28 d during storage at
(the nature of which was not described) in this reported tocopherol
5°C. Billion-Rey et al.37 reported that retinol (palmitate) was
loss was not clear, as the vitamins were added to the fat emulsion,
stable for 20 d in all-in-one PN mixtures stored at 4°C, although
which was then infused into the same line with mixing only during
degradation was observed in some PN mixtures containing trace
elements, depending on the amino acid source.
It should also be noted that some multivitamin additives con-
Retinol is the most light sensitive of the vitamins. Exposure of
tain tocopherol as the acetate whereas others contain tocopherol
PN mixtures in bags to daylight can show up to 90% loss in 2– 4
base. It is not clear whether this difference has any significance
h, whereas direct sunlight will cause even more rapid degrada-
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
Information on the stability of ergocalciferol in PN mixtures
during storage is sparse. The stability of ergocalciferol duringadministration from PN mixtures has been investigated. Gillis etal.48 reported that average losses amounting to 32% were recordedduring simulated infusion from PN mixtures without fat emulsion. Dahl et al.35 reported that no losses occurred during simulatedinfusion in fat emulsion. Indirect data from bioavailability studiesin children suggest that ergocalciferol delivery from PN mixturesis at least sufficient to maintain vitamin D status.50,51
Commercially available fat emulsions contain some phylloqui-
none. Lennon et al.52 report, for example, that one product con-tained between approximately 30 – 60 g/dL, the quantity beingproportional to fat concentration. The concentration is also fairlyconsistent between batches of fat emulsion. In contrast, otherproducts contain substantially less phylloquinone. This is due tothe type of vegetable oils used.52
Phylloquinone has been reported by Billion-Rey et al.37 to be
stable in PN mixtures, with or without fat emulsion, stored inethylene vinyl acetate (EVA) bags, for 20 d at 4°C.
Phylloquinone losses of between 5 and 17% were reported
during simulated infusion over 24 h in an all-in-one TPN mixtureexposed to indirect daylight or fluorescent light.53 Billion-Rey etal.37 indicated that greater degradation occurred during simulatedinfusion in sunlight, amounting to at least 50% losses over a 12-hperiod, even in all-in-one mixtures.
Phytomenadione was reported to be stable for at least 10 d after
addition to all-in-one PN mixtures, although light protection maybe indicated following a reported 6 – 8.5% degradation after a4.5-h exposure to artificial daylight.55
Riboflavin has been reported to be stable for at least 4 d in
all-in-one PN mixtures stored at 2– 8°C,35 and for 48 h at 5°C orambient temperature in a range of PN mixtures.54 Kearney et al.54
FIG. 2. Ascorbic acid degradation pathway.
reported that riboflavin is relatively stable (Ͼ 80% remaining)after 8 wk of storage at 5°C in two-in-one PN mixtures containingdifferent amino acid infusions.
was relatively stable (Ͻ 25% degradation) in a range of two-in-
Riboflavin is degraded by exposure to daylight,56 although it is
less sensitive than retinol. Chen et al.56 reported total degradation
Direct sunlight causes degradation of pyridoxine. Chen et al.56
of riboflavin after an 8-h exposure to direct sunlight and 47% loss
reported almost 90% losses after 8 h of exposure to sunlight,
during exposure to indirect daylight. In contrast, the vitamin was
although pyridoxine was stable during exposure to indirect day-
not degraded by exposure to fluorescent light. Losses of ribo-
flavin from all-in-one PN mixtures during simulated infusion over24 h can amount to 10 –20% during indirect daylight exposure.40
Nicotinamide, Biotin, Pantothenate, and Cyanocobalamin
Provided direct exposure to sunlight is avoided, light protec-tion during administration is therefore unnecessary to protect
Although there is virtually no information on the stability of
vitamins nicotinamide, biotin, pantothenate, and cyanocobalamin
Riboflavin has been reported to accelerate the photodegrada-
in PN mixtures, Dahl et al.35 reported that these vitamins were all
tion of certain amino acids.57 Enhanced degradation of methio-
stable in an all-in-one PN mixture for 4 d at 2– 8°C.
nine, tryptophan, proline, and tyrosine accelerated in the presenceof riboflavin was reported during simulated infusion over a 24-h
period. The conditions involved extended exposure to intense
Ascorbic acid is the least stable of all the vitamins added to
phototherapy illumination. Riboflavin concentrations decreased
TPN mixtures. The mechanism of degradation is oxidation, and
by approximately 50% after 24 h of exposure to phototherapy
the compound readily reacts with oxygen. The degradation path-
way was described by Tolbert and Ward,58 and is summarized inFigure 2. The first stage of the reaction, to dehydroascorbic acid
(DHA), is reversible. It is also important to note that DHA is
Pyridoxine has been reported to be stable for 4 d at 20°C in an
biologically active, with biological activity similar to that of
all-in-one PN mixture.35 Kearney et al.54 reported that pyridoxine
ascorbic acid. The second and later stages are not reversible,
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
leading to loss of biological activity. The reaction rates are gov-
were always substantial and often greater than ascorbate concen-
erned by temperature and are accelerated rapidly by catalysts,
trations during 7 d of storage at 2– 4°C. The authors conclude that
especially copper ions, but also to a lesser extent by ferric, zinc,
a 7-d shelf-life is acceptable, although the effect of the container
The total quantity of ascorbic acid lost during storage depends
Smith et al.65 examined ascorbic acid degradation (100 mg/PN
on the amount of oxygen present.60 This oxygen originates from a
mixture) in a variety of PN mixtures containing trace elements,
number of sources, including the infusions and additives (but
with or without fat emulsion. Stability was monitored over a 48-h
excluding amino acid and fat emulsion, which are either packed
period at 25°C. Losses accumulated to between 10 and 80%,
under vacuum or are nitrogen-overlaid), aeration during fluid
depending on the amino acid used and the type of container. They
transfer into the bag, any residual headspace in the bag after filling
reported also that no losses were recorded at 5°C.
and sealing, and permeation through the bag wall during storage.
Dahl et al.53 determined the degradation of ascorbic acid (in-
Rates of oxygen transmission of plastic film used to fabricate PN
cluding DHA) in fat emulsion during infusion. The vitamin
bags have been reported as follows (conditions ϭ 100% oxygen,
source, Soluvit N, was added to fat emulsion before administra-
1 atmosphere, RH; conditions ϭ 50% side one, 90% side two):61
tion. Recovery from the infusate fell to approximately 70% after
1. EVA: Approximately 1000 mL ⅐ (m2)Ϫ1 ⅐ 24 hϪ1
8 h and to approximately 50% after 24 h.
2. Multilayered bags (composition commonly consists of a
It should also be noted from this summary that levels of DHA
triple layer of EVA/ethyl vinyl alcohol [EVOH]): Approx-
reported in different PN mixtures during storage appear to vary
widely, although the reasons are not immediately apparent.
Ascorbic acid degradation in PN mixtures during storage in big
Allwood43 investigated the causes of ascorbic acid degradation
bags and during administration has been widely reported and there
in PN mixtures. Results confirmed the importance of copper as a
is general agreement that ascorbic acid is the least stable compo-
catalyst for oxidation of ascorbate. The quantities of ascorbate
nent in any PN mixture. Most studies have measured ascorbate
degraded directly correlated with the amount of oxygen present in
only, and have not reported DHA concentrations. West et al.62
the solution. Removal of oxygen prevented significant degrada-
reported rapid degradation of ascorbic acid in two-in-one PN
tion. It was estimated that the oxygen present in infusions and
mixtures, with Ͼ 80% loss after 24 h at 25°C in one mixture.
additives, together with the oxygenation of solutions during com-
These authors also highlighted the importance of air causing the
pounding, would account for between 30 and 50 mg ascorbic acid
greatest and most rapid losses in PN mixtures. Nordfjeld et al.44
degradation. This loss would occur within 2– 6 h of compounding,
described the degradation of ascorbate in two-in-one PN mixtures
although the rate of degradation was reduced in cysteine-contain-
with trace elements in PVC bags. The vitamin source was either
ing amino acid infusions. A secondary degradation would then
MVI-12 or Soluvit and the initial concentrations were 30 and 9
commence due to the permeability of EVA for oxygen. This could
mg/L respectively. Concentrations of ascorbate in MVI-12 were
account for another 5–10 mg/d. The importance of removing all
reduced by 50%, in 2– 4 hours at 24°C, or 8 h at 4°C.
air from the bag before sealing to minimize ascorbic acid losses
Allwood63 reported ascorbate degradation in a range of two-
was emphasized. Recent studies have shown that this secondary
in-one PN mixtures in PVC bags stored at 5°C. The multivitamin
stage of ascorbic acid degradation can be largely avoided if
source was Multibionta, which contains 500 mg ascorbic acid.
multilayered bags replace the more oxygen-permeable EVA bag.66
Losses of ascorbate without trace elements accumulated to a
PN mixtures with or without fat emulsion stored in multilayered
maximum of 20% after 3 d, 30% after 7 d, and greater than 90%
bags retained up to 80% of added ascorbic acid after 3 mo storage
after 28 d. Losses, however, were influenced to some extent by the
from the vitamin source Multibionta. In EVA bags, the same
amino acid source. In the presence of trace elements, losses weregreater, with up to 80% loss after 3 d, and complete disappearance
mixtures showed complete loss of ascorbic acid after 4 –5 d.
Additional losses will also occur during administration, due to
In a later study,60 it was reported that degradation was deter-
reaction with air (oxygen) present in the administration set.
mined by the amount of oxygen present, and rates of degradation
The final stage of the ascorbate degradation pathway results in
were greatly enhanced in the presence of copper. Degradation
oxalic acid, a potentially toxic compound. Although little is
during storage at 5°C in two-in-one PN mixtures in PVC bags
known about its possible toxic effects, Das Gupta67 reported
containing Multibionta as the vitamin source showed losses of
evidence for calcium oxalate precipitation in a PN mixture during
30 – 40% in 1 d, 60% in 7 d, and 95% in 28 d. Losses during
administration. Perhaps the recommendation to separate vitamin
simulated infusion of a two-in-one TPN mixture with trace ele-
and trace element additives by administration on alternative days
ments amounted to approximately 30% in 3 h, after which deg-
radation proceeded more slowly. DHA concentrations were also
In summary, ascorbic acid is the least stable vitamin, degrading
measured during simulated infusion, never apparently rising above
by direct reaction with oxygen, which originates from infusions
5 g/mL (equivalent to only approximately 2–3% of ascorbic acid
containing dissolved air such as glucose, and additives; by aera-
tion of infusions during transfer from bag or bottle to PN bag; by
Dahl et al.35 also determined the degradation of combined total
residual air in the compounded bag after sealing; and by trans-
ascorbate (ascorbate ϩ DHA) in all-in-one PN mixtures, the
mission through the bag wall. Degradation is accelerated by trace
vitamin source being Soluvit N (Pharmacia Upjohn Ltd.) (which
elements, especially copper, but this effect is reduced by cysteine.
contains 100 mg ascorbic acid), but only one-half vial per bag.
Removal of oxygen will stabilize ascorbic acid in TPN mixtures.
Losses amounted to approximately 40% in 24 h and 60% in 4 d at
The key nutritional point, however, is that the amount of
2– 8°C in EVA bags. However, the DHA levels contributed more
ascorbic acid delivered to the patient depends on the amount of
than half of this total. Degradation during simulated infusion over
oxygen, and is unrelated to the concentration of ascorbic acid
24 h was also monitored. This amounted to an additional 15–20%
added to the bag.60 The oxygen present in any compounded bag
will depend on PN mixture composition, but estimates suggest that
Proot et al.64 examined ascorbic acid and DHA concentrations
typically 10 –50 mg can be degraded by reaction with residual
in an all-in-one PN mixture stored in a variety of containers. The
oxygen. The possible formation of oxalic acid as the final degra-
vitamin additive was Cernevit (Baxter Health Care, Ltd.) (con-
dation product and subsequent formation of calcium oxalate pre-
taining 125 mg ascorbic acid). DHA levels present during storage
cipitate requires further investigation.
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
FIG. 3. Thiamine degradation pathway.
Travasol (Baxter Health Care, Inc., Deerfield, IL, USA), which
Thiamine is degraded by a number of mechanisms.69 The
nominally contained 3 mmol/L bisulfite, showed losses of up to
compound is increasingly unstable as the pH rises and is decom-
25% after 48 h at 25°C. In contrast, thiamine was stable in PN
posed by oxidizing or reducing agents. The predominant cause of
mixtures containing amino acid infusions that did not contain
degradation in TPN mixtures is by reduction, caused in particular
bisulfite. A further study confirmed that bisulfite at concentrations
by sodium metabisulfite, used as an antioxidant in some commer-
above 1 mmol/L caused thiamine degradation.64
cial amino acid infusions.70 The route of degradation is summa-
Because thiamine degradation in PN mixtures is a result of a
rized in Figure 3.69 Sulfite cleaves the molecule into pyrimidine
chemical reaction with metabisulfite, the rates of degradation will
and thiazole moieties. The rate of this cleavage increases with
depend on metabisulfite concentration. As metabisulfite is added
increased pH to a maximum rate of pH 6.70
as an antioxidant, some variable losses of this reducing agent can
The degradation of thiamine in TPN mixtures has been widely
be expected during manufacture of the amino acid infusion. In
investigated. Early work by Scheiner et al.70 indicated that losses
addition, losses can also occur during PN mixture storage after
of thiamine were relatively rapid after addition to amino acid
compounding by reaction with oxygen. This will in turn depend on
infusions containing bisulfite, with almost complete loss recorded
the amount of oxygen in the bag and on the oxygen permeability
after 24 h at ambient temperature. Allwood63 reported that thia-
of the bag wall. Consequently, degradation of thiamine in stored
mine (50 mg/bag, Multibionta) was relatively stable during stor-
PN mixtures will depend on a number of factors and predicting
age in two-in-one PN mixtures, using amino acid infusions with or
losses is, therefore, difficult. For example, recent work in our
without metabisulfite. Greater than 75% remaining after 28 d of
laboratory indicate that thiamine is stable in PN mixtures for
storage at 5°C, although degradation was slightly greater in PN
periods in excess of 28 d in mixtures without metabisulfite.54
Other reducing agents used in amino acid infusions as reducing
It has been suggested, however, that, after dilution of meta-
bisulfite-containing amino acid infusions in PN mixtures, the
agents, such as malic acid, do not degrade thiamine. In contrast,
degradation of thiamine becomes relatively unimportant. For ex-
degradation in mixtures formulated using Freamine III 8.5% show
ample, Bowman et al.71 reported that thiamine in PN mixtures was
approximately 50% loss in 5–7 d and greater than 90% loss in
stable for 22 h at 30°C. It was assumed that dilution of metabisul-
some mixtures after 21 d.72 Because degradation is first order with
fite below 4.8 mmol was sufficient to prevent thiamine reduction.
respect to metabisulphite, degradation rate is independent of thi-
Schmutz et al.55 investigated the effect of fat emulsion, amino
acid, container, and temperature on the stability of thiamine.
Chen et al.56 noted a 26% loss of thiamine in PN mixtures after
Losses were greatest when Freamine III (contains 9.6 mmol/L
8 h of exposure to sunlight, but no significant losses after exposure
bisulfite nominal) was used as the amino acid source. Only 25%
to indirect daylight or fluorescent light. Thiamine in TPN is not
remained after 48 h of storage at 25°C. PN mixtures containing
degraded by exposure to phototherapy light,55 fluorescent, or
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
indirect daylight, but exhibits approximately 26% degradation
Louie and Stennet77 investigated the stability of folic acid in
after 8 h of exposure to direct daylight.56
amino acid dextrose mixtures under light (fluorescent illumina-
As acute thiamine deficiency caused by failure to include
tion) and dark conditions, at 2– 8°C or ambient temperature, and
multivitamin additives in PN has been shown to be fatal,73 it is
reported that the compound was stable for 48 h under any com-
important to ensure that patients receive adequate amounts.
Finally, there is evidence to suggest that certain B vitamins
Folic acid is included in many multivitamin preparations de-
The conflicts in published results make it difficult to reach firm
signed for PN addition. An alternative form is folic acid injection.
conclusions. Results obtained in our laboratory have indicated that
The pH of this product is in the range of 8 –11 to ensure folic acid
folic acid is stable in a range of two-in-one PN mixtures tested in
remains in solution. The compound will precipitate, especially in
multilayered bags, with greater than 80% remaining after 2 mo of
storage (M.C. Allwood and M.C.J. Kearny, unpublished data).
Early reports suggested that folic acid was unstable in PN
mixtures stored in plastic (PVC) bags, leading to losses of between
2 and 33% after 42 d of storage at ambient temperature.75 It wassuggested that losses were due to absorption to the PVC bag. Later
Common practice is to avoid adding vitamins to PN mixtures
studies suggest that folic acid in PN mixtures is compatible with
until immediately before administration, in which case the addi-
tion is commonly made by ward staff at the bedside, without
Nordfjeld et al.44 reported very poor stability of folic acid after
pharmaceutic control. The least stable vitamin is undoubtedly
addition to two-in-one TPN mixtures, with losses of at least 75%
ascorbic acid, and losses during administration can be substantial,
after 24 h of storage. Degradation was even greater if exposed to
although these can, to some extent, be predicted by our knowledge
light (although the nature of this light was not described). In
of the mechanisms involved in ascorbate oxidation. Because deg-
contrast, in another report folic acid was shown to be relatively
radation is directly related to oxygen content of compounded PN
stable in many PN mixtures. Barker et al.74 reported that folic acid
mixtures, the use of the multilayered reduced-gas-permeable bag
in a range of complete PN mixtures was relatively stable when
can prevent substantial ascorbate losses during storage. Paradox-
stored at 4°C. Losses generally amounted to not more than 10%
ically, the presence of ascorbic acid then enhances the overall
after 14 d of storage. However, whereas Nordfjeld et al.44 tested
stability of the PN mixture by creating a highly reduced chemical
two multivitamin preparations containing folic acid (400 g/vial),
environment. Two other important mechanisms lead to vitamin
Barker et al.74 used folic acid injection to supplement the low folic
losses. Thiamine reduction can be rapid in PN mixtures containing
acid content of a multivitamin additive (Solivito, Pharmacia Up-
metabisulfite, but this stabilizer is now absent from most amino
john, Ltd.) to increase final concentrations to between 0.40 and
acid infusions. Photodegradation, especially of retinol, can be
prevented during storage and controlled during administration by
Folic acid has also been shown to be stable in all-in-one
minimizing exposure to daylight. All-in-one mixtures protect
mixtures for 4 d at 4°C or at ambient temperature.77 Chen et al.56
photo sensitive ingredients to all light except direct sunlight.
reported that folic acid in PN mixtures was stable for 8 h of
Retinol absorption to plastic bags and administration equipment
exposure to either florescent light, indirect, or direct daylight.
can be prevented by using the palmitate ester. REFERENCES
1. Dunham B, Marcuard S, Khazaine PG, Meade G, Craft T, Nichols K.
neonatal parenteral nutrient solutions containing aminosyn PF. Am J
The solubility of calcium and phosphorus in neonatal total parenteral
12. Kaminski MV, Harris DF, Collins CF, Sommers GA. Electrolyte
2. Henry RS, Jurgens RW, Stugeon R, Athaniker N, Welco A, van
compatibility in a synthetic amino acid hyperalimantation solution.
Leuvan M. Compatibility of calcium chloride and calcium gluconate
with sodium phosphate in a mixed TPN solution. Am J Hosp Pharm
13. Jimenez-Torres NV, Juan Colomer J, Ronchera-Oms CL, et al. Aporte
de glucosa-l-fosfato en nutricion parenteral total protocolizada. Nutr
3. Poole RL, Rupp CA, Kerner JA. Calcium and phosphorus in neonatal
parenteral nutrition solutions. JPEN 1983;7:358
14. Ronchera-Oms CL, Jimenez-Torres NV, Peidro J. Stability of paren-
4. Schuetz DH, King JC. Compatibility and stability of electrolytes,
teral nutrition admixtures containing organic phosphates. Clin Nutr
vitamins and antibiotics in combination with 8% amino acid solution.
15. Hanning RM, Atkinson SA, Whyte RK. Efficacy of calcium glycer-
5. Driscoll DF, Newton DW, Bistrian BR. Precipitation of calcium
ophosphate vs conventional mineral salts for total parenteral nutrition
phosphate from parenteral nutrient fluids. Am J Hosp Pharm 1994;
in low-birth-weight infants: a randomized clinical trial. Am J Clin
6. Allwood MC. The compatibility of calcium phosphate in paediatric
16. Food and Drug Administration. Safety alert: hazards of precipitation
TPN infusions. J Clin Pharm Ther 1987;12:293
associated with parenteral nutrition. Am J Hosp Pharm 1994;51:1427
7. Lenz GJ, Mikrut BA. Calcium and phosphate solutions in neonatal
17. Allwood MC, Greenwood M. Assessment of trace element compati-
parenteral nutrient solutions containing Aminosyn-PF or Trophamine.
bility in total parenteral nutrition infusions. Pharm Weekbl (Sci)
8. Eggert ID, Rusho WJ, Mackey MW, Chan GM. Calcium and phos-
18. Koorenhof MJC, Timmer JG. Stability of total parenteral nutrition
phorus compatibility in parenteral nutrition solutions for neonates.
supplied as “all-in-one” for children with chemotherapy-linked hy-
perhydration. Pharm Weekbl (Sci) 1992;14:50
9. Jimenez-Torres NV, Ronchera-Oms CL. Calcium and phosphate in
19. Knowles JB, Cusson G, Smith M, Sitrin MD. Pulmonary deposition of
all-in-one mixtures. In: Proceedings 9th Congress ESPEN. Barcelona
calcium phosphate crystals as a complication of home total parenteral
10. Bishop NJ, Morley R, Day JP, Lucas A. Aluminum neurotoxicity in
20. Stennet DJ, Gerwick WH, Egging PK, Christensen JM. Precipitate
preterm infants receiving intravenous-feeding solutions. N Engl J Med
analysis from an in-dwelling total parenteral nutrition catheter. JPEN
11. Fitzgerald AK, Mackey MV. Calcium and phosphate solubility in
21. Shearer CA, Bozian RC. The availability of trace elements in intra-
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
venous hyperalimentation solutions. Drug Intell Clin Pharm 1977;11:
51. Davis AT, Franz FP, Coutney DA, Ullrey DE, Scholten DJ, Dean RE.
Plasma vitamin and mineral status in home parenteral nutrition pa-
22. Kartinos NJ. Trace element formulations in intravenous feeding. In:
Johnson IDA, ed. Advances in parenteral nutrition. Lancaster: MTP
52. Lennon C, Davidson KW, Sadowski JA, Mason JB. The vitamin K
content of intravenous lipid emulsions. JPEN 1993;17:142
23. Boddapati S, Yang K, Murty R. Intravenous solution compatibility
53. Dahl GB, Svensson L, Kinnander NJG, Zander M, Bergstrom UK.
and filter-retention characteristics of trace element preparations. Am J
Stability of vitamins in soybean oil fat emulsion under conditions
simulating intravenous feeding of neonates and children. JPEN 1994;
24. Allwood MC. The compatibility of four trace elements in total par-
enteral nutrition infusions. Int J Pharmaceutics 1983;16:57
54. Kearney MCJ, Martin H, Allwood MC, Hardy G. Stability of vitamins
25. Bates CG, Greiner G, Gegenheimer A. Precipitate in admixtures of
in TPN mixtures after prolonged storage. In: BAPEN conference
new amino acid injection. Am J Hosp Pharm 1984;41:1316
26. Chatterji DC, Kapoor J. Precipitate in admixtures of new amino acid
55. Schmutz CW, Martinelli E, Muhlebach S. Stability of vitamin K
injection, reply. Am J Hosp Pharm 1984;41:1316
assessed by HPLC in total parenteral nutrition. Clin Nutr 1992;
27. Hinchliffe L, Allwood MC. SEM-EDX Assessment of in-line filters
following administration of paediatric TPN mixtures. NTPNG Sym-
56. Chen MF, Boyce W, Triplett L. Stability of B vitamins in mixed
28. Wan KK, Tsallas G. Dilute iron dextran formulation for addition to
parenteral nutrition solution. JPEN 1983;7:462
parenteral nutrient solutions. Am J Hosp Pharm 1980;37:206
57. Bhatia J, Stegink LD, Ziegler EE. Riboflavin enhances photo-oxida-
29. Sayers MH, Johnson DK, Schumann LA, Ivey MF, Young JH, Finch
tion of amino acids under simulated clinical conditions. JPEN 1983;
CA. Supplementation of total parenteral nitrition solutions with fer-
58. Tolbert BM, Ward JB. Dehydroascorbic acid. In: Advances in chem-
30. Levander OA. Considerations in the design of selenium bioavailability
ical series. Washington: American Chemical Society, 1982;200:101
59. Davies MB, Austin J, Partridge DA. Vitamin C: its chemistry and
31. Shils ME, Levander OA. Selenium stability in TPN solutions. Am J
biochemistry. Letchworth: Royal Society of Chemistry Paperback,
32. McGee CD, Mascarwnhas MG, Ostro MJ, Rasallas G, Jeejeebhoy K.
60. Allwood MC. Factors influencing the stability of ascorbic acid in total
Selenium and vitamin E stability on parenteral solutions. JPEN 1985;
parenteral nutrition infusions. J Clin Hosp Pharm 1984;9:75
61. Hardy G, Mari G. The stability of TPN solutions in a new plastic
33. Ganther HE, Kraus RJ. Chemical stability of selenious acid in total
parenteral nutrition solutions containing ascorbic acid. JPEN 1989;13:
62. West KR, Sansom LN, Cosh DG, Thomas MP. Some aspects of the
stability of parenteral nutrition solutions. Pharma Acta Helv 1976;
34. Allwood MC, Plane JH. The wavelength-dependent degradation of
vitamin A exposed to ultraviolet light. Int J Pharmaceutics 1986;31:1
63. Allwood MC. Stability of vitamins in total parenteral nutrition solu-
35. Dahl GB, Jeppson RI, Tengborn HJ. Vitamin stability in a TPN
tions stored in three litre bags. Brit J Int Ther 1982;1:22
mixture stored in an EVA plastic bag. J Clin Hosp Pharm 1986;11:271
64. Proot P, De Pourco L, Raymakers AA. Stability of ascorbic acid in a
36. Allwood MC. Stability of vitamins in TPN solutions stored in 3 litre
standard total parenteral nutrition mixture. Clin Nutr 1994;13:273
65. Smith JL, Canham JE, Kirkland WD, Wells PA. Effect of Intralipid,
37. Billion-Rey F, Guillaumont M, Frederich A, Aulanger G. Stability of
fat-soluble vitamins A (retinol palmitate), E (tocopherol acetate) and
amino acids, container, temperature and duration of storage on vita-
K1 (phylloquinone) in total parenteral nutrition at home. JPEN 1993;
min stability in total parenteral nutrition admixtures. JPEN 1988;12:
38. Shenai JP, Stahlman MT, Chytil F. Vitamin A delivery from paren-
66. Allwood MC, Brown PE, Ghedini C, Hardy G. The stability of
teral alimentation solution. J Ped 1989;99:661
ascorbic acid in TPN mixtures stored in a multilayered bag. Clin Nutr
39. Howard L, Ohu R, Feman S, Mintz H, Ovesen L, Wolf B. Vitamin A
deficiency from long-term parenteral nutrition. Ann Int Med 1980;93:
67. Das Gupta V. Stability of vitamins in total parenteral nutrient solu-
40. Kirk B. The evaluation of a new light-protecting set. Br J Paren Ther
68. Allwood MC. Stability of vitamins in total parenteral nutrient solu-
41. Smith JL, Canham JE, Wells PA. Effect of phototherapy light, sodium
69. Williams RR, Spies TD. Vitamin B1 and its use in medicine. New
bisulfite, and pH on vitamin stability in total parenteral nutrition
York: The Macmillan Company New York, Macmillan Medical
42. Moorhatch P, Chiou WL. Interactions between drugs and plastic
70. Scheiner JM, Araujo MM, DeRitter E. Thiamine destruction by so-
intravenous fluid bags. Part 1: sorption studies on 17 drugs. Am J
dium bisulphite in infusion solutions. Am J Hosp Pharm 1981;38:1911
71. Bowman B, Nguyen P. Stability of thiamine in parenteral nutrition
43. Allwood MC. Compatibility and stability of TPN mixtures in big
72. Kearney MCJ, Allwood MC, Hardy G. The stability of thiamine in
44. Nordfjeld K, Pederson JL, Rasmussen M, Jensen VG. Storage of
TPN mixtures stored in EVA and multilayered bags. Clin Nutr 1995;
mixtures for parenteral nutrition III. Stability of vitamins in TPN
73. Anon. Deaths associated with thiamine deficient parenteral nutrition.
45. Gutcher GR, Lax AA, Farrell PM. Tocopherol isomers in intravenous
lipid emulsions and resultant plasma concentrations. JPEN 1984;8:269
74. Barker A, Hebron BS, Beck PR, Ellis B. Folic acid and total parenteral
46. Kishi HK, Yamaji A, Kataoka K, et al. Vitamin A and E requirements
during total parenteral nutrition. JPEN 1981;5:420
47. McKenna MC, Bieri JC. Loss off vitamin A from total parenteral
75. Almodovar MJ, Hernandez Jaras MV, Leon-Sanz M, et al. Estabilidad
nutrition solutions. Federation Proc 1980;39:561
48. Gillis J, Jones G, Penchardz P. Delivery of vitamins A, D and E in
76. Lee DR, Ware I. Survival of folic acid in TPN solutions. Br J Int Ther
total parenteral nutrition solutions. JPEN 1983;7:11
49. Drott P, Meurling S, Meurling L. Clinical adsorption and photodeg-
77. Louie N, Stennett DJ. Stability of folic acid in 25% dextrose 3.5%
radation of the fat soluble vitamins A and E. Clin Nutr 1991;10:348
amino acids and multi-vitamin solution. JPEN 1984;8:421
50. Hariz MB, De Potter S, Corriol O, et al. Home parenteral nutrition in
78. Biamonte AR, Schneller GH. A study of folic acid stability in solu-
children: bioavailability of vitamins in binary mixtures for 8 days.
tions of the B complex vitamins. J Am Pharmacol Assoc (Sci ed)
Közlemény A Magyar Antidopping Csoport szorosan együttműködve a magyar sportolókkal, és a hazai sportszervezetekkel, tájékoztatást kíván adni, a WADA 2009. október 1-én nyil-vánosságra hozott, 2010. évi új Tiltólistájáról. A változások részletesen megtalálhatók awww.wada-ama.org, illetve a www.antidopping.hu honlapokon. Kiemelt változásoK a 2010-es tiltólistá
Questions - Réponses 1. A quoi sert la bromocriptine ? 2. Quels sont les complications associées à l’utilisation de la bromocriptine dans l’inhibition ou la prévention de la lactation et les facteurs augmentant le risque de complications ? 3. Pourquoi le rapport entre les bénéfices et les risques dans l’indication « inhibition ou prévention de la lactation » (et se
 REVIEW ARTICLE
REVIEW ARTICLE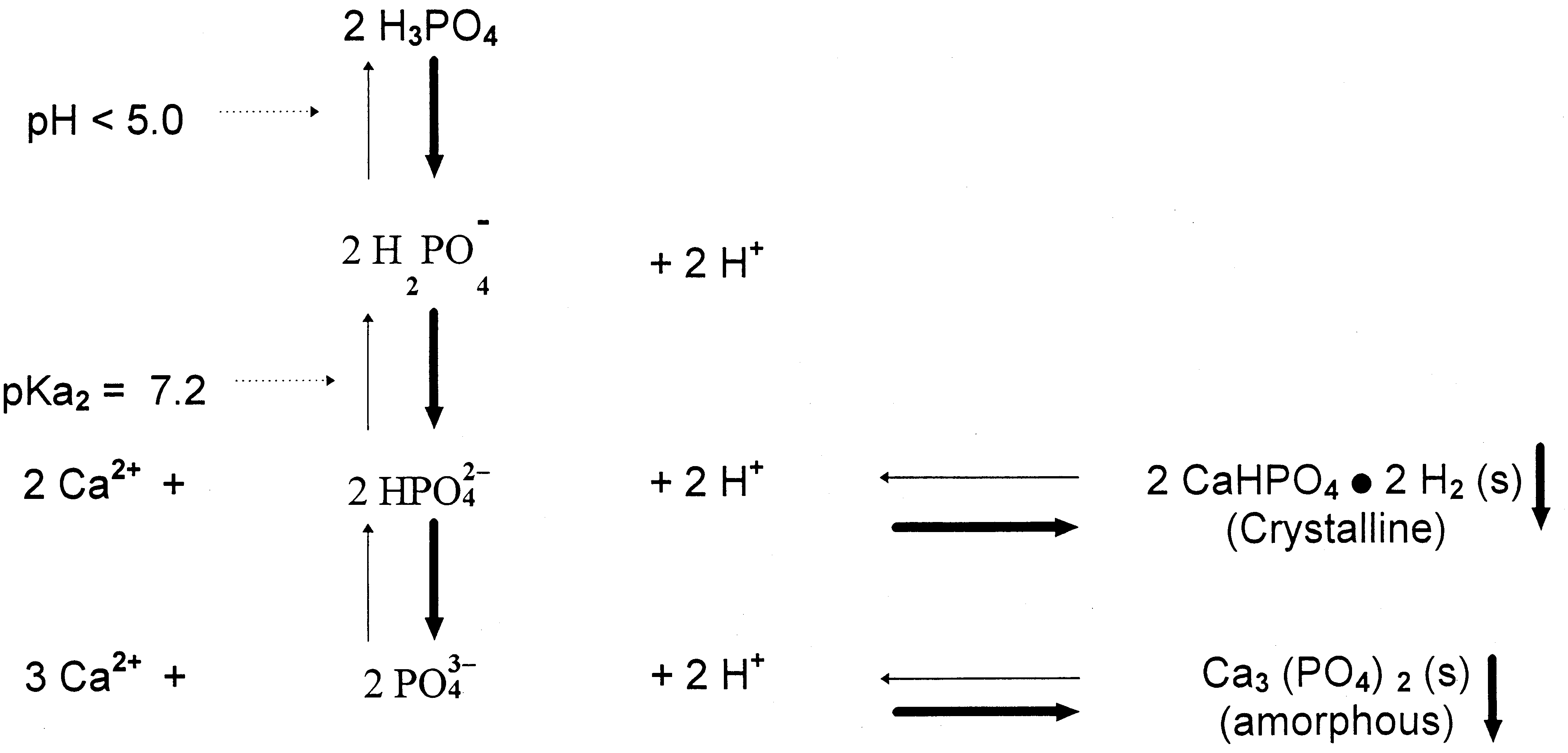 ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
FIG. 1. Speciation of inorganic phosphate in parenteral nutrition mixtures.
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
FIG. 1. Speciation of inorganic phosphate in parenteral nutrition mixtures. ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
Information on the stability of ergocalciferol in PN mixtures
during storage is sparse. The stability of ergocalciferol duringadministration from PN mixtures has been investigated. Gillis etal.48 reported that average losses amounting to 32% were recordedduring simulated infusion from PN mixtures without fat emulsion.
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
Information on the stability of ergocalciferol in PN mixtures
during storage is sparse. The stability of ergocalciferol duringadministration from PN mixtures has been investigated. Gillis etal.48 reported that average losses amounting to 32% were recordedduring simulated infusion from PN mixtures without fat emulsion.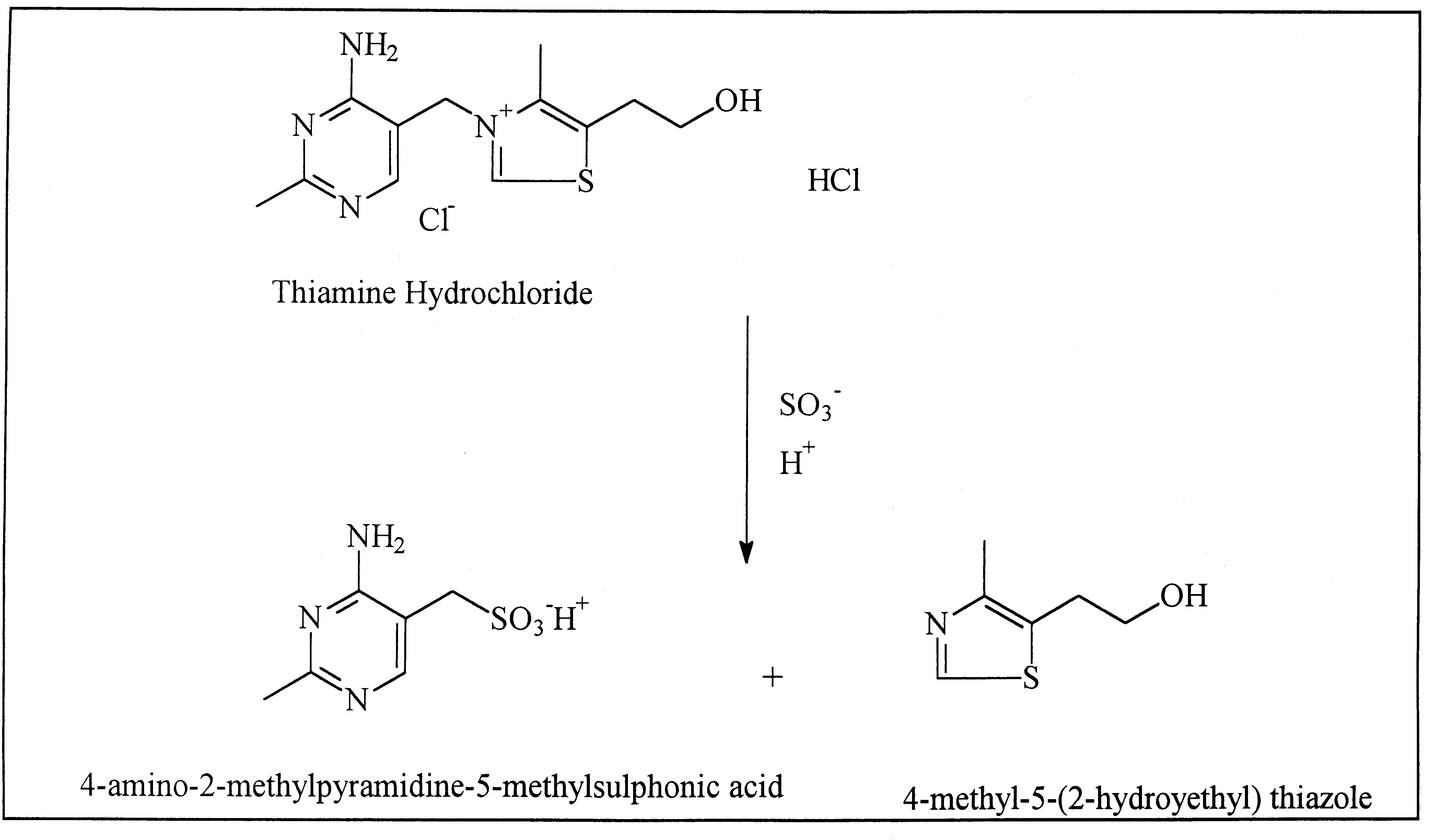 ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
FIG. 3. Thiamine degradation pathway.
ADDITIVES IN PARENTERAL NUTRITION ADMINISTRATION
FIG. 3. Thiamine degradation pathway.