Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
New patient form
PLEASE GIVE US YOUR INSURANCE CARD TO BE PHOTOCOPIED
Please print clearly
Patient’s name: _________________________________________________________ Date: ______________________________________
Address:_______________________________________________________________ Home phone: ________________________________
City: __________________________________________________________________ State: ___________ Zip: ______________________
Patient’s occupation: _____________________________________________________ S.S.#: ______________________________________
Employer:______________________________________________________________ Business phone: _____________________________
Employer’s address: _____________________________________________________ State: ___________ Zip: ______________________
Birthdate: __________________________ Age: ____________ Sex: _____________ Marital status: S M W D Sep (circle one)
If married, name of spouse: ____________________________________________________________________________________________
Person responsible for payment: ____________________________________________ Relationship: ___________ Birthdate: ___________
Address of responsible person: _____________________________________________ State: ___________ Zip: ______________________
Whom may we thank for referring you to us? ______________________________________________________________________________
Family or personal physician: __________________________________________________________________________________________
Whom may we contact in case of emergency? _________________________________ Phone: _____________________________________
INSURANCE INFORMATION (Please check appropriate line)
***We are participating with Medicare and Blue Shield; however, certain plans require patients to pay deductible, co-insurance or eligible services
Insurance company name:_________________________________________________
Group no: ________________________Identification No: ________________________
Subscriber:_____________________________________________________________(name of person carrying insurance)
Subscriber’s SSN (if other than patient): ______________________________________Subscriber’s birthdate: _________________________
Lab to use: _____________________________________________________________
BRIEF MEDICAL HISTORY
(Rash, Acne, Growth, Scalp, Hair, etc.)_______________________________
______________________________________________________________
______________________________________________________________ ______________________________________________________________
When did you first notice this problem?_______________________________
______________________________________________________________ ______________________________________________________________
______________________________________________________________
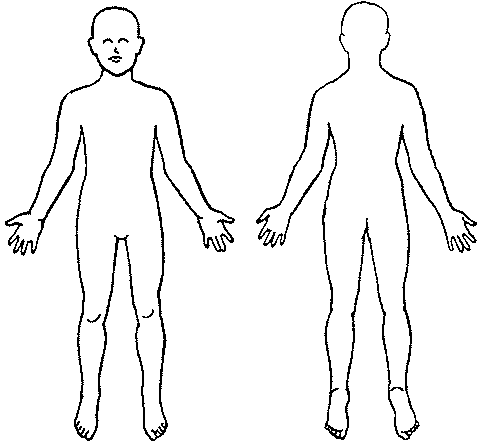
Please indicate on the figures here where your present skin
problem is by marking an “X” on the body sketch Yes
Does your skin react to anything (tape, jewelry, perfume)?
(For female patients only) Are you now pregnant?
PLEASE ANSWER QUESTIONS ON REVERSE SIDE
Allergic reaction to Novocaine or Xylocaine?
Blood transfusion within the past 10 years?
Are you under the treatment of a doctor? _________________________________________________________
Reason: ___________________________________________________________________________________
MEDICINES
Has a doctor given you anything for your skin? If yes, please list t6he names of everything you have been given:
______________________________________________________________________________________________________ ______________________________________________________________________________________________________ ______________________________________________________________________________________________________
Have you put anything else on your skin yourself? (Non-prescription drugs, lotions, creams, etc.) Please list the names of
everything you have used on it: _____________________________________________________________________________ Do you take any of the following? If so, give name of drug:
Steroids? __________________________________________________________________________________
Aspirin or pain pills? _________________________________________________________________________
Nerve pills / sedatives? _______________________________________________________________________
Laxatives? _________________________________________________________________________________
Birth control pills? ___________________________________________________________________________
Anticoagulants (blood thinners)?________________________________________________________________
Please list all other medication that you are presently taking: ______________________________________________________
______________________________________________________________________________________________________ ______________________________________________________________________________________________________
IN ORDER TO SUBMIT A CLAIM TO YOUR INSURANCE CARRIER, IT IS NECESSARY THAT THE PATIENT, OR PERSON
ACTING ON HIS OR HER BEHALF, SIGN THE FOLLOWING AUTHORIZATION:
“I AUTHORIZE ANY HOLDER OF MEDICAL OR OTHER INFORMATION ABOUT ME TO RELEASE TO MY MEDICAL INSURANCE CARRIER OR TO ITS INTERMEDIARIES, OR TO THE BILLING AGENT OF THIS PHYSICIAN OR SUPPLIER
WHICH IS CHERYL D. ACKERMAN, M.D., ANY INFORMATION NEEDED FOR THIS OR A RELATED CLAIM. I PERMIT A
COPY OF THIS AUTHORIZATION TO BE USED IN PLACE OF THE ORIGINAL, AND REQUEST PAYMENT OF MEDICAL
INSURANCE BENEFITS EITHER TO MYSELF OR TO THE PARTY WHO ACCEPTS ASSIGNMENT.”
fusion avec PSEG, s’il était couronné desuccès, pourrait contribuer à ouvrir lavoie à une redéfinition des frontières,des zones d’influence et des capacités Les origines Après avoir présenté un panorama du secteur électrique aux États-Unis (voir Flux n°56/57), nous consacrons ce portrait d’entreprise à l’une des plus anciennes américain, qui joua un rôle central
 PLEASE GIVE US YOUR INSURANCE CARD TO BE PHOTOCOPIED
Please print clearly
PLEASE GIVE US YOUR INSURANCE CARD TO BE PHOTOCOPIED
Please print clearly