Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
102397 a comparison of sustained-release bupropion
S U STA I N E D - R E L E AS E B U P RO P I O N VS. P L AC E B O FO R S M O K I N G C E S SAT I O N
A COMPARISON OF SUSTAINED-RELEASE BUPROPION AND PLACEBO
RICHARD D. HURT, M.D., DAVID P.L. SACHS, M.D., ELBERT D. GLOVER, PH.D., KENNETH P. OFFORD, M.S.,
J. ANDREW JOHNSTON, PHARM.D., LOWELL C. DALE, M.D., MOISE A. KHAYRALLAH, PH.D., DARRELL R. SCHROEDER, M.S.,
PENNY N. GLOVER, M.ED., C. ROLLYNN SULLIVAN, M.D., IVANA T. CROGHAN, PH.D., AND PAMELA M. SULLIVAN, M.D. ABSTRACT
nicotine may act as an antidepressant in some smok-
ers.3,4 The development of a depressed affect or de-
medications for smoking cessation have had mixed
pression after smoking cessation may lead to re-
results. We conducted a double-blind, placebo-con-
trolled trial of a sustained-release form of bupropion
Results of clinical trials of antidepressant therapy
for smoking cessation. We excluded smokers with
for smoking cessation have been mixed. The initial
current depression, but not those with a history of
experience with doxepin was promising; however, no
major depression. The 615 subjects were randomly
large trials have been reported.8 The results of trials
assigned to receive placebo or bupropion at a dose
of fluoxetine have not been published. A serotonin-
of 100, 150, or 300 mg per day for seven weeks. The
uptake inhibitor had no effect on smoking rates in
target quitting date (or “target quit date”) was one
week after the beginning of treatment. Brief counsel-
heavy smokers. An immediate-release form of bu-
ing was provided at base line, weekly during treat-
propion (300 mg per day for 12 weeks) showed ef-
ment, and at 8, 12, 26, and 52 weeks. Self-reported
ficacy in two double-blind, placebo-controlled trials,
abstinence was confirmed by a carbon monoxide
one with 42 male smokers and the other with 190
concentration in expired air of 10 ppm or less.
smokers.10 On the basis of these results, we evaluated
the efficacy and safety of a sustained-release form of
the rates of smoking cessation as confirmed by car-
bupropion (Zyban, Glaxo Wellcome) as an aid to
bon monoxide measurements were 19.0 percent in
smoking cessation. This form of bupropion was re-
the placebo group, 28.8 percent in the 100-mg group,
cently approved by the Food and Drug Administra-
38.6 percent in the 150-mg group, and 44.2 percent
tion as a prescription drug for the indication of
in the 300-mg group (PϽ0.001). At one year the re-spective rates were 12.4 percent, 19.6 percent, 22.9
percent, and 23.1 percent. The rates for the 150-mggroup (Pϭ0.02) and the 300-mg group (Pϭ0.01) —
but not the 100-mg group (P ϭ0.09) — were signif-
Subjects
icantly better than those for the placebo group. Among the subjects who were continuously absti-
This randomized, double-blind, placebo-controlled, dose–
nent through the end of treatment, the mean abso-
response study was performed at three sites (Mayo Clinic, Roch-
lute weight gain was inversely associated with the
ester, Minn.; the Palo Alto Center for Pulmonary Disease Preven-
dose (a gain of 2.9 kg in the placebo group, 2.3 kg in
tion, Palo Alto, Calif.; and West Virginia University, Morgantown)and approved by each center’s institutional review board. Recruit-
100-mg and 150-mg groups, and 1.5 kg in the 300-
ment was conducted through advertisements and press releases.
mg group; Pϭ0.02). No effects of treatment were ob-
A total of 742 volunteers who were interested in stopping smok-
served on depression scores as measured serially by
ing were evaluated, of whom 615 met the study criteria and un-
the Beck Depression Inventory. Thirty-seven subjects
derwent randomization. After an initial screening interview con-
stopped treatment prematurely because of adverse
ducted by telephone, subjects attended an informational meeting
events; the frequency was similar among all groups.
at which the study was explained, questionnaires completed, and
on was effective for smoking cessation and was ac-
The subjects were eligible for inclusion if they were at least 18
years of age, had smoked an average of 15 cigarettes or more per
companied by reduced weight gain and minimal side
day for the past year, were motivated to stop smoking, and were
effects. Many participants in all groups were smok-
in generally good health. Only one smoker per household was al-
ing at one year. (N Engl J Med 1997;337:1195-202.)
lowed in the study. Exclusion criteria included the presence or a
1997, Massachusetts Medical Society.
From the Nicotine Research Center (R.D.H., L.C.D., I.T.C.), the Sec-
otine-replacement therapy have been shown
tion of Biostatistics (K.P.O., D.R.S.), and the Division of Community In-ternal Medicine (R.D.H., L.C.D.), Mayo Clinic and Mayo Foundation,
to help smokers stop smoking. Using a med-
Rochester, Minn.; the Palo Alto Center for Pulmonary Disease Prevention,
ication that does not contain nicotine, such
Palo Alto, Calif. (D.P.L.S.); Robert C. Byrd Health Sciences Center, WestVirginia University, Morgantown (E.D.G., P.N.G., C.R.S., P.M.S.); and
as an antidepressant, has intrigued investigators for
Glaxo Wellcome, Inc., Research Triangle Park, N.C. (J.A.J., M.A.K.). Ad-
several reasons. Smokers are more likely to have a
dress reprint requests to Dr. Hurt at the Mayo Clinic, 200 First St. SW,
history of major depression than nonsmokers,1,2 and
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
family history of a seizure disorder, a history of severe head trau-
ppm or less. To be classified as continuously abstinent, the sub-
ma, predisposition to seizures (such as a history of brain tumor
jects had to be confirmed as not smoking on the basis of carbon
or stroke), a history or current diagnosis of anorexia nervosa or
monoxide measurement at each visit. In all cases, an intention-to-
bulimia, the presence of an unstable medical or psychiatric con-
treat analysis was performed. Subjects who missed a follow-up vis-
dition, pregnancy, lactation, a history of dependence on alcohol
it were considered to be smoking. Randomization of subjects was
or a non-nicotine substance within the past year, current use of
stratified according to site to ensure that similar numbers of sub-
psychotropic medications, previous use of bupropion, current use
jects were assigned to each group at each site. However, to verify
of tobacco products other than cigarettes, and current use of any
the assumption that the effect of treatment was not dependent
nicotine-replacement therapy, fluoxetine, clonidine, buspirone, or
on the study site, the efficacy of smoking cessation was first eval-
doxepin. Subjects with current depression as assessed by the phy-
uated with logistic-regression modeling. In these models, the de-
sician were also excluded. Those with a history of major de-
pendent variable was smoking status, as confirmed by carbon
pression as assessed by a structured clinical interview were not ex-
monoxide measurement, and the independent variables were dose
(placebo vs. 100 mg vs. 150 mg vs. 300 mg of bupropion) and
At the base-line visit subjects were randomly assigned to receive
study site (California vs. Minnesota vs. West Virginia). We includ-
either a sustained-release form of bupropion at a dose of 100 mg
ed an interaction term to assess whether the effect of dose was
per day (50 mg twice a day), 150 mg per day (150 mg each morn-
dependent on the study site. After verifying that the effect of
ing and placebo each evening), or 300 mg per day (150 mg per
treatment was not dependent on the study site, we performed a
day for three days, followed by 150 mg twice a day) or placebo
logistic-regression analysis to assess differences between groups
(twice a day). All the tablets were identical in appearance. Subjects
including site as a covariate. The comparisons of placebo with
set a target quitting date (or “target quit date”) after one week of
100 mg of bupropion, placebo with 150 mg of bupropion, and
medication (usually the eighth day). They returned weekly during
placebo with 300 mg of bupropion were identified a priori to be
the 7-week treatment phase, then at 8, 12, 26, and 52 weeks for
follow-up. The subjects were telephoned 3 days after the target
Body weight was analyzed among subjects who were continu-
quitting date and at 4, 5, 7, 8, 9, 10, and 11 months. At the base-
ously abstinent during the treatment phase. The absolute change
line physical examination, each subject received a brief, personal-
in weight from base line was calculated weekly from the start of
ized message to stop smoking from the physician and self-help
medication through the end of treatment. The effect of dose was
material based on the National Cancer Institute program.12 In this
evaluated with a two-factor repeated-measures analysis of variance
program, which has been validated as an effective intervention for
model, with dose as an independent continuous cross-classifica-
smoking cessation, the physician asks each patient whether he or
tion factor and time as the repeated factor. We included an inter-
she smokes, advises all smokers to stop smoking, helps the patient
action term to assess whether the effect of dose was consistent
set a quitting date, and arranges a follow-up visit.
over time. Linear regression and pairwise dose comparisons were
Subjects underwent chest roentgenography, laboratory testing,
electrocardiography, and physical examination. We obtained data
Withdrawal symptoms were assessed daily with a composite
on smoking history, asked subjects to keep a daily diary to record
withdrawal score computed as the mean of the nine items includ-
smoking rates and symptoms of nicotine withdrawal,13 and ad-
ed in the daily diary. Symptoms of nicotine withdrawal included
ministered several questionnaires.14-16 The eight-item Fagerström
craving for a cigarette; depressed mood; difficulty falling asleep;
Tolerance Questionnaire is a widely used measure of nicotine de-
awakening at night; irritability, frustration, or anger; anxiety; dif-
pendence with a score ranging from 0 to 11; a score of 6 or great-
ficulty concentrating; restlessness; and increased appetite. The se-
er indicates higher levels of dependence.17 The Beck Depression
verity of each symptom was scored by the subject on a five-point
Inventory is a 21-item questionnaire completed by the subject
scale as absent (0), slight (1), mild (2), moderate (3), or severe
that assesses the severity of depressive symptoms.15 Total scores
(4). For each subject a base-line withdrawal score was calculated
range from 0 to 63, with scores of 9 or below considered to be
with data from all diaries completed before the start of medica-
within the normal range. Scores of 10 to 18 indicate mild-to-
tion, during which time the subjects were instructed to continue
moderate depression, scores of 19 to 29 indicate moderate-to-
smoking their usual number of cigarettes. Withdrawal-symptom
severe depression, and scores of 30 or higher indicate severe de-
scores obtained after the target quitting date were analyzed as the
pression. Each week we collected the subjects’ daily diaries and
change from base line. The data were summarized daily for the
recorded concomitant medication use, adverse events, vital signs,
first week after the target quitting date and as weekly means for
and the carbon monoxide content of expired air. Self-reported ab-
each of the next five weeks. For each group, the mean change in
stinence was considered validated by a carbon monoxide level in
the withdrawal score was compared with zero by the one-sample
expired air of 10 ppm or below. Brief individual counseling (ap-
t-test. The effect of treatment was evaluated with a two-factor re-
proximately 10 to 15 minutes) was provided by a study assistant
peated-measures analysis of variance model in which change in
the withdrawal score was the dependent variable, treatment groupwas an independent cross-classification factor, and time was the
Statistical Analysis
repeated factor. Separate analyses were performed for the daily
The sample size was based on the ability to detect a difference
summary of week 1 and the weekly summary of the entire treat-
between active treatment and placebo at the end of treatment,
ment phase. In addition to the overall model, separate pairwise
given a projected abstinence rate of 40 percent in the bupropion
analyses were performed that compared each active-treatment
groups and 24 percent in the placebo group. Approximately 130
subjects were needed for each treatment group, in order to have
Symptoms of depression were assessed with the Beck Depres-
a two-sided alpha level of 0.05 and a power of 0.80 to detect such
sion Inventory15 at base line and at weeks 2 and 6 after the target
a difference. To ensure an adequate sample, 150 subjects were en-
quitting date. Depression scores were analyzed in terms of the
change from base line. For each group, the mean change in the
The base-line characteristics of the four groups of subjects were
depression score was compared with zero by the one-sample t-test.
compared by analysis of variance for continuous variables and chi-
The effect of treatment was evaluated with a two-factor repeated-
square analysis for categorical variables. The efficacy of smoking
measures analysis of variance model in which change in the de-
cessation was evaluated with the use of weekly point-prevalence
pression score was the dependent variable, treatment group was
abstinence rates and rates of continuous abstinence. For the
an independent cross-classification factor, and time was the re-
point-prevalence rates, subjects were classified as abstinent if they
peated factor. Fisher’s exact test was used to compare the rates of
reported not smoking during the previous seven days and this re-
adverse events for each active-treatment group with those in the
port was confirmed by an expired carbon monoxide value of 10
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
S U STA I N E D - R E L E AS E B U P RO P I O N VS. P L AC E B O FO R S M O K I N G C E S SAT I O N
shown in Table 2. At the end of the treatment phase
The base-line characteristics of the subjects are
(week 6 after the target quitting date), the cessation
presented in Table 1. There were no significant dif-
rate for each of the three active-treatment groups was
ferences among the groups. A total of 219 subjects
significantly better than for the placebo group. Sub-
(148 during the treatment phase and 71 subse-
jects who received 300 mg of bupropion per day had
quently) did not complete the 12-month study. Of
a significantly better (Pϭ0.005) cessation rate than
these subjects, 196 (89 percent) withdrew their con-
those who received 100 mg per day. The respective
sent for various reasons (e.g., scheduling difficulties
point-prevalence smoking-cessation rates at six weeks
or perceived lack of benefit); 15 stopped participat-
and one year were 19.0 percent and 12.4 percent in
ing because of an adverse event, 6 because of pro-
the placebo group and 44.2 percent and 23.1 per-
tocol deviations, and 1 for administrative reasons;
cent in the group that received 300 mg of bupropi-
1 subject died. The rate of completion of the study
on. At one year, the smoking-cessation rates for the
increased with the dose and was 57 percent, 65 per-
150-mg and 300-mg groups — but not the 100-mg
cent, 64 percent, and 71 percent for the placebo,
group — were significantly better than that for the
100-mg, 150-mg, and 300-mg groups, respectively
placebo group. When dose was treated as a continu-
(Pϭ0.01 by logistic-regression analysis in which dose
ous variable, a significant dose effect was detected
was treated as a continuous variable).
at all periods (PϽ0.001 at week 6, Pϭ0.003 at
The biochemically confirmed point-prevalence
3 months, Pϭ0.03 at 6 months, and Pϭ0.02 at 12
smoking-cessation rates according to treatment are
TABLE 1. BASE-LINE CHARACTERISTICS OF THE SUBJECTS.* OF BUPROPION OF BUPROPION OF BUPROPION CHARACTERISTIC (N؍153) (N؍153) (N؍153) (N؍156)
No. of cigarettes smoked/day in past year
No. of previous serious attempts to quit‡
*Plus–minus values are means ϮSD. Because of rounding, not all percentages total 100. †The range for the Fagerström score is 0 to 11; a score of 6 or greater indicates higher levels of
nicotine dependence.14,17 Data were missing for two subjects in the 100-mg group and one subjectin the 300-mg group.
‡Data were missing for two subjects in the 300-mg group.
§The scores on the Beck Depression Inventory can range from 0 to 63, with scores of 9 or below
considered to be within the normal range. Scores of 10 to 18 indicate mild-to-moderate depression,scores of 19 to 29 moderate-to-severe depression, and scores of 30 or higher severe depression.15 Datawere missing for four subjects each in the placebo and 300-mg groups and two subjects each in the100-mg and 150-mg groups.
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
TABLE 2. POINT-PREVALENCE SMOKING-CESSATION RATES CONFIRMED BY CARBON MONOXIDE MEASUREMENT.* TIME AFTER TARGET QUITTING DATE PERCENTAGE OF SUBJECTS NOT SMOKING P VALUE†
*Point prevalence was estimated weekly.
†The P values given are from analyses that did not include site as a covariate; therefore, they can be obtained directly from the given
cessation rates. In logistic-regression analyses that included site as a covariate the same differences were found to be statistically significant. The overall P value is for the simultaneous comparison of all four groups treated categorically. When dose was treated as a continuous variable,a significant dose effect was detected at all times (PϽ0.001 at week 6, Pϭ0.003 at 3 months, Pϭ0.03 at 6 months, and Pϭ0.02 at 12months). The pairwise dose comparisons presented were identified a priori, and the corresponding P values are unadjusted.
‡Week 6 was the final week of study medication.
Figure 1 shows the rates of continuous abstinence
phase is shown in Figure 2. At the end of treatment,
from the target quitting date through the end of
the subjects had gained a mean of 2.9 kg in the pla-
treatment (10.5 percent in the placebo group, 13.7
cebo group (16 subjects), 2.3 kg in the 100-mg
percent in the 100-mg group, 18.3 percent in the
group (21 subjects) and the 150-mg group (28 sub-
150-mg group, and 24.4 percent in the 300-mg
jects), and 1.5 kg in the 300-mg group (38 sub-
group). The rate of continuous abstinence was sig-
jects). Weight change was negatively associated with
nificantly better in the group that received 300 mg
the dose (Pϭ0.003, by repeated-measures analysis
of bupropion than in the placebo group (Pϭ0.001)
of variance), with evidence of an interaction be-
and in the group that received 100 mg of bupropion
tween dose and time (Pϭ0.04) that indicated a
larger disparity between doses at later periods. Foreach of the first six weeks after the target quitting
Weight Change
date, weight change was negatively associated with
The mean change in weight from the start of
dose, with less weight gain found with higher doses
medication (base line) for the 103 subjects who
of bupropion. Of the 59 subjects who were contin-
were continuously abstinent during the treatment
uously abstinent from the target quitting date to thesix-month follow-up visit, the mean weight gain wasnot significantly associated with dose: 5.5 kg in theplacebo group (9 subjects), 6.6 kg in the 100-mggroup (10 subjects), 4.4 kg in the 150-mg group
(21 subjects), and 4.5 kg in the 300-mg group (19
Symptoms of Depression and Withdrawal
During the medication phase, there was no evi-
dence of a difference in change among treatment
groups in the mean scores on the Beck Depression
Inventory. In addition, the change in scores from base
line was not significantly different from zero for anygroup either two weeks after the target quitting date
(mean ϮSD change, Ϫ0.3Ϯ4.7 in the placebo group
[121 subjects], ϩ0.4Ϯ4.1 in the 100-mg group [124
subjects], ϩ0.6Ϯ4.9 in the 150-mg group [123 sub-
Figure 1. Rates of Confirmed Continuous Abstinence from the
jects], and ϩ0.3Ϯ5.0 in the 300-mg group [128 sub-
Target Quitting Date through the End of Treatment.
jects]) or at the end of treatment (Ϫ0.8Ϯ4.7 [103
Self-reported abstinence was confirmed by a finding of an ex-
subjects]; ϩ0.5Ϯ5.5 [115 subjects]; Ϫ0.4Ϯ5.7 [110
pired carbon monoxide concentration of 10 ppm or less. The
subjects], and ϩ0.8Ϯ5.2 [128 subjects], respec-
asterisks (0.01ϽPр0.05), daggers (0.001ϽPр0.01), and doubledaggers (P
р0.001) indicate significant differences from place-
bo. All subjects are included at all time points.
The mean changes from base line in the compos-
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
S U STA I N E D - R E L E AS E B U P RO P I O N VS. P L AC E B O FO R S M O K I N G C E S SAT I O N
stopped treatment prematurely because of adverse
events (8 in the placebo group [5 percent], 9 in the
100-mg group [6 percent], 7 in the 150-mg group
[5 percent], and 13 in the 300-mg group [8 per-
cent]). Tremor, headaches, rash, and urticaria werethe most common reasons for stopping treatment.
Three serious adverse events were reported during
or immediately after the medication phase. A 23-
year-old man assigned to receive 300 mg of bupropi-
on per day reported extreme irritability, restlessness,
anger, anxiety, and cravings soon after he stopped
smoking. The study medication was stopped, and he
began treatment with a nicotine patch. Two days lat-
er he was doing well. A 66-year-old woman assigned
to the 300-mg group had an allergic reaction mani-
fested by a pruritic rash, angioedema, dyspnea, and
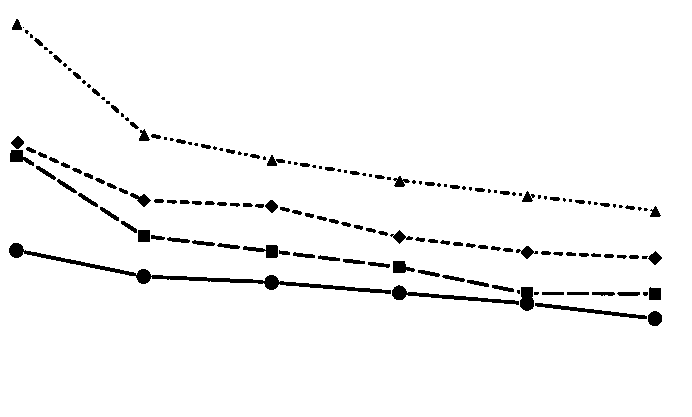
Figure 2. Mean Change in Weight from Base Line through the
petechiae. She had received bupropion for 24 days,
End of Treatment among 103 Subjects Who Were Continuously
but had begun taking amoxicillin–clavulanate for the
treatment of bronchitis 8 days before the onset of
Weight was analyzed at the end of each week. The mean
the reaction. The bupropion and amoxicillin–clavu-
weight change was significantly greater than zero (PϽ0.05 by
lanate were stopped, and the reaction resolved after
the one-sample t-test) at weeks 1 through 6 in the placebogroup, at weeks 2 through 6 in the 100-mg and 150-mg groups,
treatment with antihistamines, epinephrine, and cor-
and at weeks 3 through 6 in the 300-mg group. The P values
ticosteroids. The reaction was judged to be most
shown are for the effect of dose assessed with a linear regres-
likely related to amoxicillin–clavulanate. A 63-year-
sion model in which absolute change in weight was the de-
old woman with preexisting cardiomyopathy and hy-
pendent variable and dose was the independent variable.
pertension had cardiac and pulmonary arrest four
Asterisks (0.01ϽPр0.05), daggers (0.001ϽPр0.01), and thedouble dagger (Pр0.001) indicate a significant difference (by
days after completing the treatment phase (300-mg
the two-sample t-test) from placebo. The number of subjects
with data available is the same for all periods except week 5,for which data were missing for one subject in the 150-mg
group. Treatment was started at base line.
We found that the sustained-release form of bu-
propion was an effective treatment for smoking ces-sation, although many participants in all groups
ite withdrawal scores are shown in Figure 3. For each
were smoking at one year. There was a significant
group, the mean change from base line was signifi-
dose response at all periods. Furthermore, the rates
cantly greater than zero (i.e., withdrawal symptoms
of abstinence at one year were significantly better
increased) at all periods. For the first week after the
in the 150-mg group (Pϭ0.02) and the 300-mg
target quitting date, the change in the withdrawal
group (Pϭ0.01) than in the placebo group. Al-
scores was not significantly different among the four
though the 300-mg dose was the most effective ini-
treatment groups. In the analysis of the weekly means,
tially, its effects were not significantly different from
a significant treatment effect was detected (PϽ0.001).
those of the 150-mg dose at the end of treatment
From the pairwise comparisons of the active-treat-
or at one year. Nonetheless, the 300-mg dose was
ment groups with the placebo group, only the 100-
the only one to show a difference in the rates of con-
mg group had significantly more withdrawal symp-
tinuous abstinence from the target quitting date
toms (Pϭ0.008) than the placebo group. There
through the end of treatment. Thus, we would rec-
were no significant interactions between time and
ommend using the 300-mg dose (150 mg twice a
day) as the target dose for most patients, given the
Despite explicit instructions to the contrary, seven
favorable side-effect profile and the fact that there
subjects used nicotine-replacement products during
was less weight gain during the medication phase
the study, only one of whom stopped smoking at
with this dose. Because steady-state plasma levels of
any point. That subject chewed one piece of nicotine
bupropion are usually reached within eight days, we
gum on day 17 before remembering he was not
started the medication at least seven days before the
target quitting date in order to ensure that these lev-els were attained.18 We used bupropion for seven
weeks on the basis of pilot studies and experience
All adverse events reported one or more times by
with nicotine-patch therapy, which showed that ex-
at least 10 percent of subjects in any given treatment
tending treatment beyond eight weeks does not ap-
group are shown in Table 3. A total of 37 subjects
pear to increase efficacy.19 Although this duration of
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Figure 3. Mean Change from Base Line in the Withdrawal Score.
For each group, the mean change from base line was significantly greater than zero (PϽ0.05 by the one-sample t-test)in all periods. Asterisks (0.01ϽPр0.05) and daggers (0.001ϽPр0.01) indicate a significant difference from placebo (bythe two-sample t-test). The numbers of subjects for whom data were available are listed below the figure. TABLE 3. ADVERSE EVENTS AMONG SUBJECTS.* OF BUPROPION OF BUPROPION OF BUPROPION ADVERSE EVENT (N؍153) (N؍153) (N؍153) (N؍156)
*Adverse events that were experienced one or more times by at least 10 percent of subjects in any
group are listed in decreasing order according to overall frequency. No significant differences werefound between any bupropion groups and placebo for adverse events reported by less than 10 percentof subjects in all groups with the exception of bronchitis and vasodilatation, which each occurred insix subjects in the 100-mg group and no subjects in the placebo group (Pϭ0.03).
†Pϭ0.008 for the comparison with placebo by Fisher’s exact test. ‡Pϭ0.01 for the comparison with placebo by Fisher’s exact test.
therapy may be adequate, a longer duration may be
smaller weight gain in subjects who continuously ab-
appropriate if relapse is a concern. Antidepressants
stained from smoking and who were receiving higher
are commonly used for several months to treat de-
doses of bupropion. The typical weight gain associ-
pression or chronic pain and have little potential for
ated with successful smoking cessation is 3 to 4 kg,20
abuse. We did not, however, study a longer duration
and it is a concern that inhibits many smokers (espe-
cially women) from attempting to stop.21 Nicotine-
Another important finding was the significantly
replacement therapy has had mixed results in con-
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
S U STA I N E D - R E L E AS E B U P RO P I O N VS. P L AC E B O FO R S M O K I N G C E S SAT I O N
trolling weight gain after smoking cessation,22-27 with
The strengths of our study are the sample size, the
nicotine gum and nicotine nasal spray showing the
use of multiple centers, the dose response, and the
greatest benefit. A medication effective for smoking
efficacy demonstrated by point-prevalence rates and
cessation that is also capable of minimizing the asso-
rates of continuous abstinence. However, subjects
ciated weight gain would offer a major advantage.28
who enroll in clinical trials are motivated to stop
Bupropion seems to have that potential, even though
smoking and may not be representative of the gen-
the differences observed were moderate, and the ef-
eral population of smokers. Much remains to be
fect seems to be limited to the time the drug is used.
learned, such as the optimal duration of treatment,
The effect of a longer treatment period on weight
the potential role of combination therapy with nico-
tine-replacement products, and the use of bupropion
Nicotine activates central nervous system path-
for smoking cessation in smokers with depression.
ways to release norepinephrine, dopamine, and otherneurotransmitters29,30 and elevates dopamine levels
Supported by a grant from Glaxo Wellcome.
in areas of the brain associated with the reinforce-ment of the effects of amphetamines, cocaine, and
We are indebted to the following people for their hard work and
opiates.31-33 Bupropion is a weak inhibitor of the
assistance in completing this project: Marilyn Eischen, Karen Hur-
neuronal uptake of norepinephrine and dopamine
tis, and Troy Wolter from the Mayo Clinic; Paul M. Maloney,Lynne D. Rowe, R.N., Alicia B. Gonzales, Susan L. Winget, Carol
but has no effect on serotonin.34 Its dopaminergic
A. Sontag, R.N., and Barbara Newman from the Palo Alto Cen-
and noradrenergic activities could be responsible for
ter for Pulmonary Disease Prevention; and Connie Cerullo and
its efficacy in smoking cessation, with the dopamin-
Anna Greco from the West Virginia University Health Sciences
ergic activity affecting areas of the brain having to
do with the reinforcement properties of addictive
drugs and the noradrenergic activity affecting nico-tine withdrawal.34 We observed no treatment effects
1. Glassman AH, Helzer JE, Covey LS, et al. Smoking, smoking cessation,
on depression scores as measured serially by the
and major depression. JAMA 1990;264:1546-9. 2. Hall SM, Munoz R, Reus V. Smoking cessation, depression and dys-
Beck Depression Inventory; thus, the mechanism for
phoria. NIDA Res Monogr 1991;105:312-3.
bupropion’s efficacy is unlikely to be through its an-
3. Glass RM. Blue mood, blackened lungs: depression and smoking. JAMA 1990;264:1583-4.
tidepressant effects. However, subjects with current
4. Hughes JR. Dependence potential and abuse liability of nicotine re-
depression were excluded from this study. Further
placement therapies. In: Pomerleau O, Pomerleau C, eds. Progress in clin-
study is needed for a full understanding of the re-
ical evaluation. New York: Alan R. Liss, 1988:261-77. 5. Covey LS, Glassman AH, Stetner F. Depression and depressive symp-
toms in smoking cessation. Compr Psychiatry 1990;31:350-4.
Bupropion was well tolerated, with the most fre-
6. Hall SM, Munoz RF, Reus VI. Cognitive-behavioral intervention in-
quent adverse effects being headache, insomnia, and
creases abstinence rates for depressive-history smokers. J Consult Clin Psy-chol 1994;62:141-6.
dry mouth. Antidepressants are associated with a
7. Shiffman S. Relapse following smoking cessation: a situational analysis.
small risk of seizure.35 For sustained-release bupro-
J Consult Clin Psychol 1982;50:71-86. 8. Edwards NB, Murphy JK, Downs AD, Ackerman BJ, Rosenthal TL.
pion used for the treatment of depression, this risk
Doxepin as an adjunct to smoking cessation: a double-blind pilot study.
is 0.1 percent for doses of up to 300 mg per day
(i.e., one seizure per 1000 subjects receiving bupro-
9. Sellers EM, Naranjo C, Kadlec K. Do serotonin uptake inhibitors de- crease smoking? Observations in a group of heavy drinkers. J Clin Psycho-
pion for varying periods of time — from a few weeks
to more than a year).36 Our study lacked adequate
10. Ferry LH, Burchette RJ. Efficacy of bupropion for smoking cessation
power to evaluate seizures at these low rates. None
in non-depressed smokers. J Addict Dis 1994;13:249. 11. Spitzer RL, Williams JBW, Gibbon M, First MB. User’s guide for the
of the 462 subjects in this study who received bu-
structured clinical interview for DSM-III-R: SCID. Washington, D.C.:
propion had a seizure. However, we excluded poten-
American Psychiatric Press, 1990. 12. Glynn TJ, Manley MW. How to help your patients stop smoking: a
tial subjects who had a personal or family history of
National Cancer Institute manual for physicians. Bethesda, Md.: National
seizures, a history of severe head trauma, eating dis-
Cancer Institute, 1990. (NIH publication no. 90-3064.)
orders, or active alcoholism. In clinical practice,
13. Hughes JR, Hatsukami D. Signs and symptoms of tobacco withdrawal. Arch Gen Psychiatry 1986;43:289-94.
patients should be screened for the possibility of sei-
14. Fagerström KO. Measuring degree of physical dependence to tobacco
zure before they start treatment with bupropion.
smoking with reference to individualization of treatment. Addict Behav
Even though relief of nicotine-withdrawal symp-
1978;3:235-41. 15. Beck AT, Steer RA. Beck Depression Inventory. Philadelphia: Center
toms is not a prerequisite for smoking cessation, we
were puzzled by the finding that subjects who re-
16. Swenson WM, Morse RM. The use of a self-administered alcoholism screening test (SAAST) in a medical center. Mayo Clin Proc 1975;50:204-
ceived 100 mg of bupropion a day had a higher
mean score for withdrawal symptoms. A possible ex-
17. Fagerström KO, Schneider NG. Measuring nicotine dependence: a re-
planation is that a dose of 50 mg twice a day was
view of the Fagerström Tolerance Questionnaire. J Behav Med 1989;12:159-82.
sufficient to produce side effects that could be inter-
18. Ferris RM, Cooper BR. Mechanism of antidepressant activity of bu-
preted as similar to withdrawal symptoms, but was
propion. J Clin Psychiatry Monogr 1993;11:2-14.
not sufficient to reduce the severity of true with-
19. Fiore MC, Smith SS, Jorenby DE, Baker TB. The effectiveness of the nicotine patch for smoking cessation: a meta-analysis. JAMA 1994;271:
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
20. Williamson DF, Madans J, Anda RF, Kleinman JC, Giovino GA, Byers
trolled trial of nasal nicotine spray in smoking cessation. Lancet 1992;
T. Smoking cessation and severity of weight gain in a national cohort.
28. Perkins KA. Issues in the prevention of weight gain after smoking ces- 21. Klesges RC, Somes GW, Pascale R, et al. Knowledge and beliefs
sation. Ann Behav Med 1994;16:46-52.
regarding the consequences of cigarette smoking and their relationships
29. Gilman AG, Rall TW, Nies AS, Taylor P, eds. Goodman and Gilman’s
to smoking status in a biracial sample. Health Psychol 1988;7:387-
the pharmacological basis of therapeutics. 8th ed. New York: Pergamon
22. Tønnesen P, Fryd V, Hansen M, et al. Effect of nicotine chewing gum 30. Wise RA. Brain neuronal systems mediating reward processes. In:
in combination with group counseling on the cessation of smoking.
Smith JE, Lane JD, eds. Neurobiology of opiate reward mechanisms. New
York: Elsevier Biomedical Press, 1983:405-38. 23. Nides M, Rand C, Dolce J, et al. Weight gain as a function of smoking 31. Di Chiara G, Imperato A. Drugs abused by humans preferentially in-
cessation and 2-mg nicotine gum use among middle-aged smokers with
crease synaptic dopamine concentrations in the mesolimbic system of freely
mild lung impairment in the first 2 years of the Lung Health Study. Health
moving rats. Proc Natl Acad Sci U S A 1988;85:5274-8. 32. Pontieri FE, Tanda G, Orzi F, Di Chiara G. Effects of nicotine on the 24. Leischow SJ, Sachs DPL, Bostrom AG, Hansen MD. Effects of differ-
nucleus accumbens and similarity to those of addictive drugs. Nature 1996;
ing nicotine-replacement doses on weight gain after smoking cessation.
33. Clarke PB. Nicotine dependence — mechanisms and therapeutic strat- 25. Transdermal Nicotine Study Group. Transdermal nicotine for smoking
egies. Biochem Soc Symp 1993;59:83-95.
cessation: six-month results from two multicenter controlled clinical trials.
34. Ascher JA, Cole JO, Colin JN, et al. Bupropion: a review of its mech-
anism of antidepressant activity. J Clin Psychiatry 1995;56:395-401. 26. Sachs DPL, Sawe U, Leischow SJ. Effectiveness of a 16-hour transder- 35. Davidson J. Seizures and bupropion: a review. J Clin Psychiatry 1989;
mal nicotine patch in a medical practice setting, without intensive group
counseling. Arch Intern Med 1993;153:1881-90. [Erratum, Arch Intern
36. Johnston JA, Lineberry CG, Ascher JA, et al. A 102-center prospective
study of seizure in association with bupropion. J Clin Psychiatry 1991;52:
27. Sutherland G, Stapleton JA, Russell MA, et al. Randomized con-
Downloaded from www.nejm.org on March 7, 2008 . Copyright 1997 Massachusetts Medical Society. All rights reserved.
Gränslösa läkemedelsproblem – vem orkar bry sig? Vi orkar bry oss, eller? Inledde moderator Fredrik Hed programmet på Läkemedelskongressen som anordnats av sektionen för Läkemedelsinformation. Enligt en undersökning som Läkemedelsverket utfört (2010) uppger 70 procent av svenskarna att man de kan tänka sig att handla läkemedel på Internet. Hela 20 procent uppger att de har g
Aesthetic Dermatology S K I N & A L L E R G Y N E W S • J u l y 2 0 0 8 Photo at left shows a patient before treatment / with the OLDG ENTER photopneumatic device. Photo at ICHAEL right shows . M improvement of the patient’s acne B Y S H A R O N W O R C E S T E R after receiving TESTY L
 T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
TABLE 2. POINT-PREVALENCE SMOKING-CESSATION RATES CONFIRMED BY CARBON MONOXIDE MEASUREMENT.*
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
TABLE 2. POINT-PREVALENCE SMOKING-CESSATION RATES CONFIRMED BY CARBON MONOXIDE MEASUREMENT.*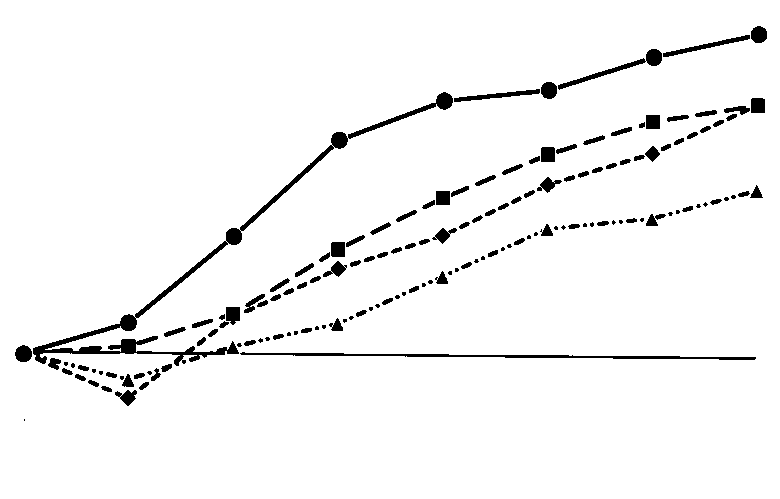 S U STA I N E D - R E L E AS E B U P RO P I O N VS. P L AC E B O FO R S M O K I N G C E S SAT I O N
S U STA I N E D - R E L E AS E B U P RO P I O N VS. P L AC E B O FO R S M O K I N G C E S SAT I O N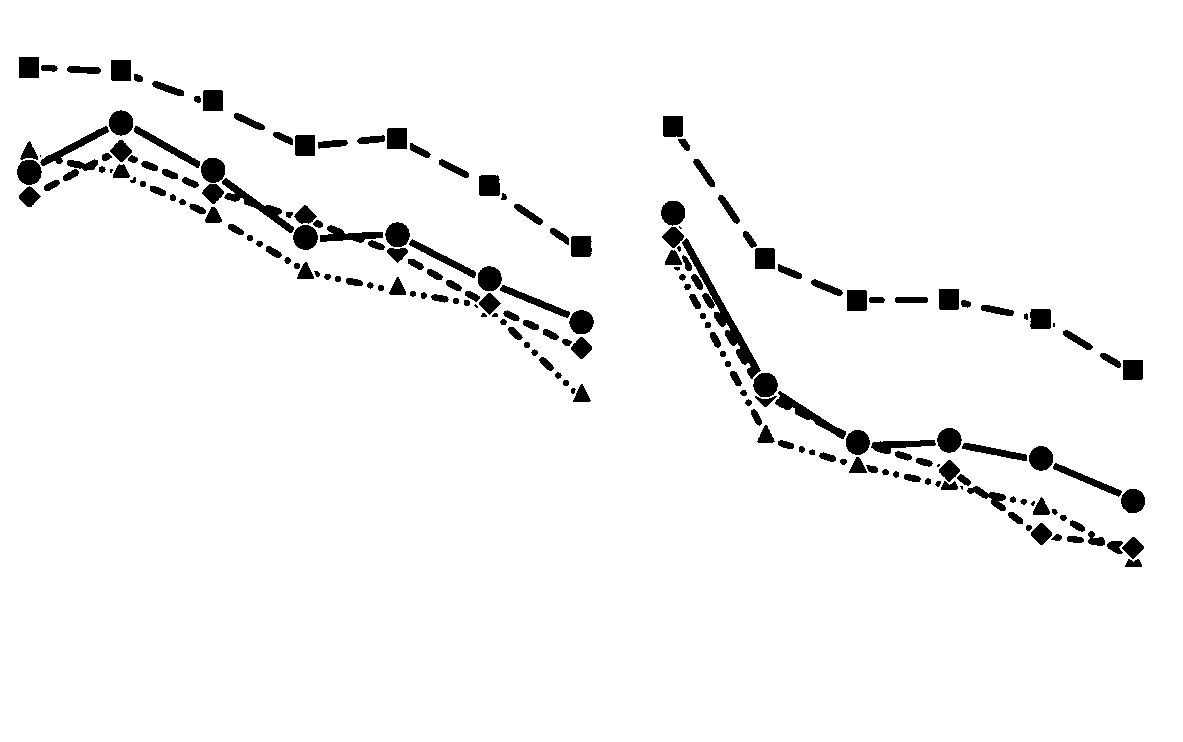 T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Figure 3. Mean Change from Base Line in the Withdrawal Score.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
Figure 3. Mean Change from Base Line in the Withdrawal Score.