Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Mini-symposium: the elbow (iv) biomechanic of the elbow
c 2003 Elsevier Science Ltd. All rights reserved.
Biomechanics Section, Mechanical Engineering Department, Imperial College, London SW72BX, UK
cal capitellum laterally. If the elbow is positioned cor-rectly under an X-ray image intensi¢er, so that the view
The upper limb is a complex mechanism with which we
is exactly along the £exion ^ extension axis, it is seen that
interact with the world around us. The joints act in con-
these articulations have approximately circular cross-
cert to position the hand, or to apply force on objects via
sections and that these circles are nested concentrically
the hand. It is the job of the shoulder to move the upper
together. This means that the joint can act as a uniaxial
limb around the body, so that the hand may reach in di-
hinge during £exion ^ extension and that there will be
rections that cover more than a hemisphere. At the
no relative motion between the radius and ulna as this
same time, the £exion ^ extension mobility of the elbow
motion occurs. This has an important practical conse-
allows the hand to reach out to objects, and then to
quence, since it means that elbow prostheses can have a
bring them back to the body.These activities usually also
simple hinge design and do not require complex geome-
require forearm rotation movements, the hand being
try in order to maintain physiological kinematics. There
pronated when picking up an object, and supinated when
are, however, many papers in the literature that have
it is brought close for examination or eating.
sought to complicate the situation, erroneously. They
In addition to mobility, the upper limb must be strong
have described phenomena such as closer contact be-
enough for daily activities. It does not require any sophis-
tween the radius and capitellum during a certain arc of
ticated engineering analysis to realize that the upper limb
elbow £exion, that does not really occur. The underlying
is a relatively long and slender structure, which means
reasons for this have been a lack of understanding of the
that external forces acting on the hand have a long lever
kinematics, relating to the orientation of the £exion ^ex-
arm, while the internal muscles pass close to the joints
tension axis, plus the use of lightly loaded cadaveric spe-
and have short moment arms about their axes.The con-
cimens that have not had their joint surfaces packed
sequence of this mechanical disadvantage is that the in-
ternal muscle forces will inevitably be much greater than
Flexion ^ extension of the forearm does not occur in
the external forces, and this will lead to large elbow joint
the sagittal plane. This is because of the carrying angle
forces. The force analysis later in this paper will show
that causes the forearm to have a valgus angulation in re-
that it is a mistake to consider the elbow to be ‘non-
lation to the humerus when the elbow is extended. The
load-bearing’: not only are the forces sometimes very
carrying angle is larger in females than males, having va-
large, but the bones are small when compared to the
lues of 141 and 111, respectively. This di¡erence is pre-
lower limb, and so the stresses on them are just as high.
sumed to relate to the di¡erent pelvic width and the
The challenges faced by the surgeon dealing with the el-
demands for carrying objects alongside the hips with
bow are compounded by the e¡ects of rheumatoid dis-
the elbow extendedThe characteristic shape given to
ease. Not only are the relatively delicate bones of the
the extended arm by the carrying angle can be lost inad-
upper limb attenuated proportionately more by erosive
vertently by malreduction of humeral supracondylar or
changes, but the demands of weight-bearing through walk-
condylar fractures, giving the unsightly ‘gunstock defor-
ing aids such as elbow crutches must often be allowed for.
mity’ if the forearm moves into varus. This must beguarded against in children, in whom the carrying angleis smaller than in adults, being typically 61. The carrying
angle is largest with the elbow extended and disappears
in full £exion, so that the forearm overlays the upperarm. This carrying angle variation occurs because the
The articular surfaces of the distal humerus consist of
£exion ^ extension axis is inclined away from being med-
the spool-shaped trochlea medially and the part-spheri-
ial ^ lateral so that it is more proximal laterally, bya half of the carrying angleThus, if the carrying angle is
Correspondence to: AAA [email protected]; Tel: 020 -7594 -7062 dir,7046 sec.
121, the £exion ^ extension axis will be 61 from the
the coronoid process and of the rim of the radial headagainst the £oors of the anterior humeral fossae.
Forearm rotation normally yields 801 pronation and
901 supination.If the motion is assessed using a rodgrasped in the hand, then a greater arc of motion will befound, due to movements of the ¢ngers, plus £exion ofthe ¢fth metacarpal in supination. Forearm rotation mo-tion can be described in both anatomical and functionalways.The classic anatomical description is that the radiusswings around the stationary ulna, in the manner of thehandle on a bucket. The anatomical axis of rotationpasses from the centre of the capitellum proximally tothe centre of the ulnar head distally, then on towardsthe little ¢nger. If the forearm is rotated while holdingthe little ¢nger in one place, the position of the hand isseen to move, and this is not the normal situation. Nor-mally, the hand remains in one place as the forearm ro-tates, and this corresponds to the rotation axis passingalong the long ¢nger. When observing this motion it isclear that pronation then entails ulnar abduction, and su-pination causes ulnar adduction. If the other hand iswrapped around the wrist, the motion of the distal ulnacan be felt: it seems to be following a rotary path.This isnot caused by the ulna rotating at the elbow, however, itis circumduction: the curved path in space is accom-plished by combinations of ulnar abduction and £exionduring pronation, and adduction and £exion during supi-nation. This description has been controversial, because
Figure 1 The carrying angle, between the centrelines of the
anatomists have noted the congruence of the humero-ul-
forearm and upper arm, disappears as the elbow £exes, due to
nar joint and clinical examination shows that the elbow
the inclination of the £exion axis, that bisects the angle between
appears to be stable against varus ^ valgus loads, so
it was suggested that there must be complementarymovements of the humerus. This was disproven,however, by experiments in which the humerus wasimmobilized by pins, then double-exposure radiographs
transverse direction. This mechanism can be demon-
taken in pronation and supination: the humero-
strated easily by copying the diagram and folding the
ulnar varus ^ valgus motion of approximately 91 was
paper along the axis. As well as remembering this
orientation when reducing and imaging the reduction of
Forearm rotation clearly involves rotational sliding
fractures, it should be built into the design and placement
motion between the concave endface of the radial head
of elbow prostheses. An incorrect carrying angle will not
and the capitellum; it also causes sliding of the proximal
only look wrong, it will displace the paths of the muscles
radio-ulnar joint. An end view shows that the radial head
across the elbow, altering the balance of joint forces.
is not circular F it is approximately elliptical.This devia-
Elbow £exion ^ extension is normally quoted as from
tion from a circle is caused largely by there being extra
01 to 1451, but females sometimes have slightly greater
material to create the bearing surface that bears against
extension mobility, reaching up to 201 of hyperexten-
the ulna. In the anatomical position, with the elbow supi-
sion.Elbow hyperextension is also more common in
nated, this articulation is seen as a part-cylindrical sur-
some racial groups and this is sometimes in association
face, that is anterior. As the forearm pronates, it passes
with the presence of a supra-trochlear foramen that
medially and then posteriorly. The proximal radio-ulnar
links the olecranon and coronoid fossae.The range of ac-
joint is stabilized by the surrounding annular ligament
tive motion is limited by apposition of the anterior mus-
that attaches strongly to the antero-lateral corner of
cle bulk in £exion, and by impingement of the olecranon
the coronoid and to the supinator ridge of the ulna. In-
process into the £oor of the olecranon fossa, plus tigh-
tegrity of this structure is important in preventing sub-
tening of the anterior joint capsule, in extension. Passive
luxation of the radial head: it resists the anteriorly
movement usually obtains greater elbow £exion, which is
directed tension of the biceps tendon during elbow
then limited by simultaneous impingement of the tip of
The simpli¢ed example was misleading because it con-
centrated solely on a ‘muscle’ that was parallel to the hu-merus, and this is a natural way to think of the situation,
It was noted in the introduction that the elbow muscles
given that the elbow is £exed by muscles such as biceps
work at a large mechanical disadvantage when compar-
and brachialis. It suggests that the joint forces act onto
ing their small moment arms about the joint axis to the
the end of the humerus. However, considering the hand,
large moment arms of loads exerted on the hand. It fol-
it is clear that there are other muscle actions inherent in
lows that the joint forces will be much greater than the
elbow £exion, to grasp the object being lifted, and to sta-
external forces, and also that they will depend almost en-
bilize the wrist. If the ¢st is clenched, even without the
tirely on the muscle tensions. Therefore, a good under-
hand supporting a load, then the tensions in the ¢nger
standing of which muscles act, and of their paths and
£exor muscles compress the humero-ulnar joint, due to
points of attachment, is central to appreciation of the
£exor digitorum super¢cialis originating from the medial
forces on the elbow. The joint forces in£uence many as-
epicondyle. At the same time, the wrist must be held
pects of clinical treatment, providing insight into why
against the £exion moments exerted by the ¢nger £exor
prostheses loosen or why bone fragments may tend not
tensions, and so there is co-contraction of the extensor
to remain in a reduced con¢guration, for example.
carpi muscles.These all cross the lateral aspect of the el-
Most of the elementary introductions to biomecha-
bow and so compress the humero-radial joint.This is gra-
nics (e.g. Nordin and Frankel) use elbow £exion as an
phically demonstrated if the ¢st is clenched after a
example with which to teach the basic fundamentals of
Monteggia lesion, and the wrist imaged by an X-ray im-
joint force calculation, by equilibrium analysis. In this sim-
age intensi¢er: the radius migrates proximally in relation
pli¢ed situation the tensionT in‘the £exor muscle’
to the ulna. The consequence of the forearm muscle ac-
is estimated by considering equilibrium of the moments
tions, for the situation seen in is that they
tending to extend and to £ex the elbow.Thus, the exten-
will now impose an AP force component onto the distal
sion moment exerted by the load in the hand is 20 N
humerus, in addition to the distal ^ proximal action of
times 0.35 m, or 7N m.This must be opposed by an equal
and opposite £exion moment from the muscle. So, if the
Since the muscle forces are dominant, it is clear that a
muscle exerts a moment of 7N m at a moment arm of
joint force analysis depends critically on due allowance
35 mm (0.035 m), the muscle tensionT must equal 7N m
for all of the co-operating muscles. There have been
divided by 0.035 m, or 200 N. In order to predict the joint
many papers on electromyography, aiming to under-
force we use an analysis called resolution of forces, in this
stand the actions of individual muscles, and how the elec-
case in the vertical direction. Summing the forces must
trical signals relate to force output. Much of the early
lead to zero resultant, if the situation is in equilibrium.
work was brought together by Basmajian;in addition,
Thus, the forces acting upwards must be equal and oppo-
Long et showed how the forearm muscles contribute
site to those acting downwards: T equals 20 N plus JF, so
to the function of the hand. In summary, actions that re-
JF is 180 N. Although this is a gross simpli¢cation (be-
quire a large force to be exerted cause all of the available
cause it is rather misleading), this example has been su⁄-
muscles to contract, not just to produce a movement,
cient both to demonstrate the basic fundamentals of
but also to stabilize the joints.Thus, if the ¢st is clenched,
equilibrium analysis, and also to show that most of the
the biceps and triceps also contract, for example. It is
joint force results from the muscle tension, and not di-
clear that, if there are many active muscles crossing the
rectly from the external force itself.
elbow, then the moment equilibrium equations will becomplex. The principal problem is to decide how muchis contributed by each muscle. It can be argued that thelower limb muscles are stimulated in a way that mini-mizes energy expended when walking, which is an activ-ity that does not impose high (fatigue inducing) stresses. In the arm, however, we need to account for maximal ac-tions, such as lifting a heavy weight, or struggling to undoa container. Then it is appropriate to assign tensions inproportion to the sizes of the muscles via the physiologi-cal cross-sectional area, a measure of the number ofmuscle ¢bres.
The size of the joint forces obviously relates to the ex-
ternal load. There was much ergonomics research done
In this simpli¢ed analysis of elbow £exion, the mus-
cle tensionT is 200 N, and so the joint force JF is180 N.The lackof
in the 1950s and 1960s investigating strength when oper-
any muscle actions modelled along the forearm means that JF is
ating machines.This is useful here (e.g. Hunsicker), as an
predicted to act axially onto the distal humerus.
input to the moment equilibrium equations.
When triceps tension resists the £exing moment
The force on the distal humerus, during elbow £ex-
from an external load, tensile stresses are caused in the olecra-
ion, is greatest near extension, because the forearm and elbow
non, causing it to be vulnerable to fracture.
£exor muscles act in nearly the same directions. As £exion pro-gresses, the elbow joint force reduces and swings onto the ante-
tends to sublux the radial head anteriorly during elbow
rior aspect of the humeral joint surfaces. It acts onto the base ofthe coronoid and the posterior lip of the radial head at all angles
£exion the joint is stabilized by the axial forces in the
forearm muscles that keep the capitellum engaged inthe concave endface of the radial head.
Elbow extension results primarily from triceps ten-
The variation of forces acting onto the distal humerus
sion; the triceps is by far the strongest muscle in the
during elbow £exion is shown in When the elbow is
upper limb. It follows that elbow extension causes large
near full extension both the forearm muscles and the el-
humero-ulnar joint forces and that the triceps tension
bow £exors (principally biceps, brachialis, brachioradialis
causes large tensile stresses in the olecranon
and pronator teres) are pulling in similar directions.Their
The joint force varies from 1.5 kN acting onto the distal
tensile forces are then additive, resulting in very large
aspect of the humerus at full extension, to 3.5 kN acting
forces acting onto the end of the humerus. This reaches
onto the antero-distal aspect at 1201 £exion. This is im-
a maximum of 5 kN at 301 £exion, for maximal isometric
portant when placing an elbow prosthesis, since the ole-
strength of a normal young male adultIn the middle of
cranon may be eroded by rheumatoid disease, and
the arc of £exion the force vectors are AP for the fore-
further excavation for the ¢xation stem or keel of an im-
arm muscles and proximal for the elbow £exors, giving
plant should be minimized.There is also some force on
intermediate force values (2.5 kN) acting posteriorly
the humero-radial joint as the elbow extends, partly due
and proximally onto the distal humerus In the
to the wrist stabilizing muscles and partly from the lat-
£exed elbow the elbow £exors tend to distract the joint,
eral head of the triceps, which does not insert into the
in opposition to the forearm muscles that are always act-
tip of the olecranon but passes alongside it laterally and
ing along the forearm.Thus, the elbow forces fall to their
dissipates into the fascia over the anconeus.
lowest values,1kN maximum. In addition to the e¡ect of
Forearm pronation is driven primarily by the pronator
the directions of the force vectors the joint forces fall as
teres and pronator quadratus, while supination results
the elbow £exes because of the increasing muscle mo-
primarily from actions in biceps and supinator.Although
ment arms and falling muscle tensions. In extension the
these muscles tend to cause forces acting transversely to
elbow £exors rest against the anterior aspect of the
the axis of the forearm, they normally act in concert
joint so they have small moment arms about the axis.
with hand gripping and wrist stabilising actions that pull
This entails large tensions in order to produce a given
the bones axially.The result is that the humero-radial and
£exion e¡ect. As £exion proceeds, so the moment arms
humero-ulnar joints are loaded, while the proximal
of the muscles increase and the joint force can decrease.
radio-ulnar joint is subjected to only small forces.
At the same time, the muscle length-tension e¡ect
Actions in which the hand is pushing towards the cen-
comes into play: as the muscle shorten, so their maxi-
treline of the body with the elbow £exed, such as when
mum active tension producing capability decreases,
pulling a door open or holding a large box, tend to cause
also causing the joint force to decrease.
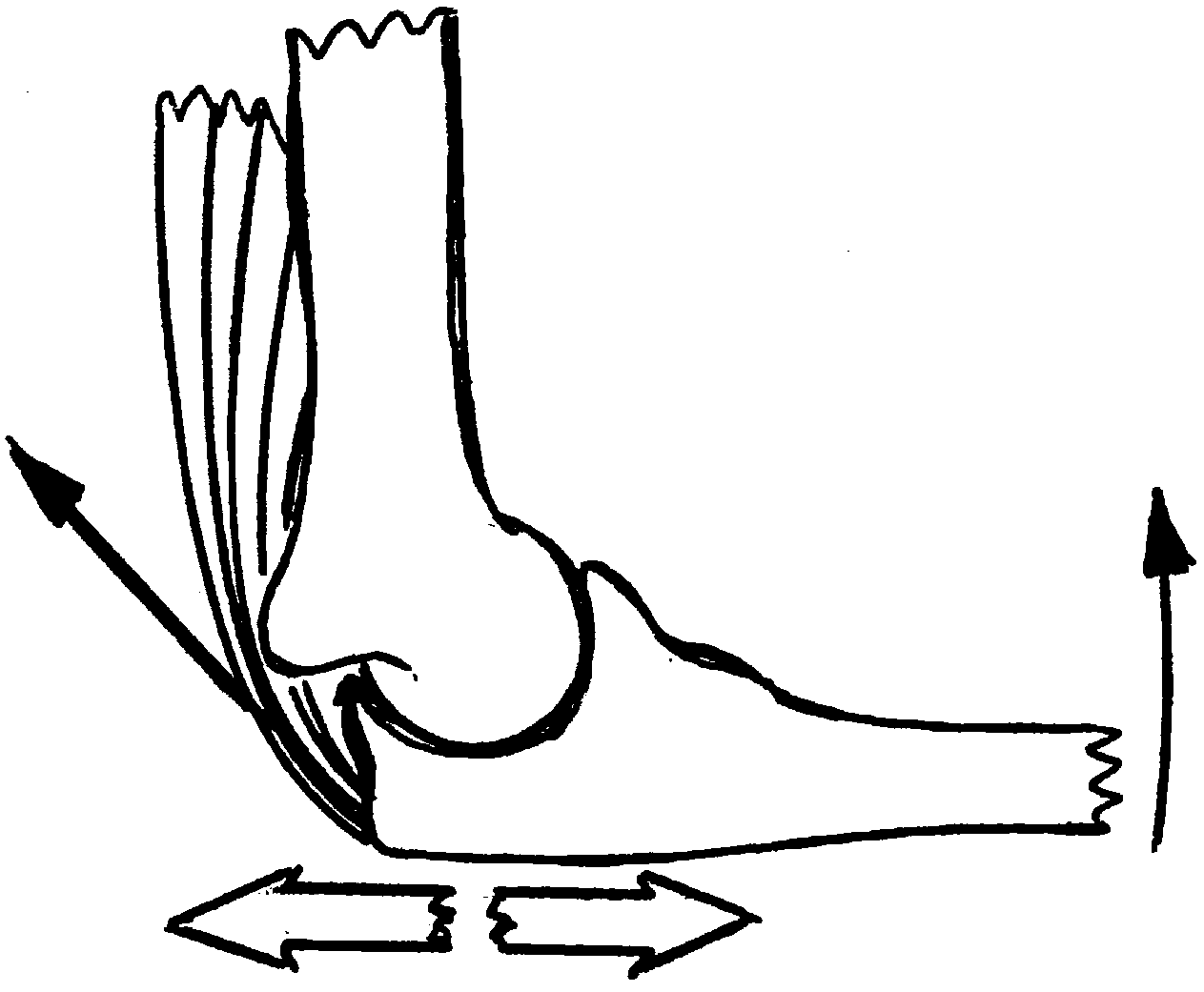
torsion load on the humerus. This is in response to ten-
Because of the combination of forearm muscles and
sions in the anterior pectoral muscles causing internal
elbow £exors acting, the forces acting on the distal hu-
rotation at the shoulder. This situation shows why the
merus correspond to equal and opposite reactive forces
distal humerus is so wide: this gives a base to resist the
onto the radius and ulna, and these are mostly acting dis-
abduction action of the forearm. The load is resisted by
tally and slightly posteriorly, that is towards the base of
a force couple: tension in the medial collateral ligament,
the coronoid process and towards the posterior rim of
and compression in the humero-radial joint If
the radial head Although the biceps tension
the radial head is missing, it is clear that the forces will
tions have shown that, if the force is directed along thecentreline of the forearm, then approximately 70% of theload is transmitted by the radius directly to the capitel-lum.If the force vector passes towards the lateral sideof the elbow, then all of the load passes directly to theradius and this is a stable situation. If the force passesmedially, the tenuous lateral collateral ligament struc-tures do not maintain stability, but this situation is notnormally encountered due to the carrying angle biasingthe loads to the radial side of the elbow.
In the past, anatomical texts noted how the shaft of
the ulna increases in cross-section proximally, which isthe opposite of the tendency of the radius. It seemed lo-gical to suggest that this re£ected load transfer from ra-dius to ulna via the ¢bres of the interosseous membrane,since the main ¢bres are oriented from proximal on theradius to distal on the ulna. Although an attractive con-cept, this mechanism does not hold up to an engineeringstress analysis. This is because the membrane has muchlower sti¡ness than the radius, so it cannot transmit asigni¢cant load until it is stretched by a proximal migra-tion of its radial attachment; this can only occur after ra-dial head fracture. The intact radius does not deformsu⁄ciently for a signi¢cant tension to build up in the in-terosseous membrane.
A further factor that limits the ability of the inteross-
eous membrane to transmit force is that it is slack whenthe forearm is pronated, the functional position whenpushing or falling onto the outstretched hand.This is be-cause the anatomical axis of forearm rotation passesanterior to the crest of the ulnar diaphysis to which themembrane is attached. The result is that the membraneis tightest with the forearm in mid rotation, when the
During an adduction action, the external load
radius is beyond the axis from the ulna, and slackens in
pressinginto the palm causes an abduction moment atthe elbow.
pronation, when the radius is alongside the axis. An al-
This is resisted by coupled actions of tension in the medial collat-
ternative hypothesis for the function of the interosseous
eral ligament and compression in the humeroradial joint. Similar
membrane is that it is an extensive area for muscle at-
forces apply during a fall onto the outstretched hand.
tachment, and so it acts to transmit tensile force fromthe deep muscles to the radius, in equilibrium with thecompressive force of the carpus loading the end of the
be concentrated onto the lateral edge of the coronoid
radius. A side-e¡ect of the muscle attachments is that
process. Since the base is narrower, this load will be
the muscles will tend to pull the ¢bres distally, away from
greater than that which had acted on the radial head,
the radius after an injury that has ruptured the mem-
and so too will be the tension in the ligament. It is these
brane, and so it often will not heal.
forces that cause torsional ¢xation failure of prostheses
In a fall forwards onto the outstretched hand, the
and which require the ¢xation to spread widely into or
posture taken up automatically has the shoulder partly
internally rotated, the elbow slightly £exed (approxi-mately 151), and the forearm semi-pronated, so that thepalm faces the £oor.The £exed posture is important
because this allows the elbow to £ex and the shoulder
to extend, after impact, thus absorbing energy bystretching their surrounding muscles rather than frac-
Pushing actions cause compressive forces to pass
turing a rigid column of bone.The landing posture places
through the hand and wrist, then along the forearm to
the lateral aspect of the elbow uppermost on impact.
the elbow. This situation is magni¢ed in a fall, when the
Consideration of the dorsi£exing tendency of the force
hand is extended to break the fall. A number of investiga-
from the £oor onto the hand reveals that the radius will
be compressed and the medial collateral ligament tensed
(similar to .Thus,100% of the impact force passes tothe radial head and so it is the most common site of bone
1. Amis A A, Miller J H. The elbow. In: Measurement of Joint
fracture at the elbowThe trabecular architecture of
Movement. Clin Rheum Dis 1982; 8: 571–593.
2. Amis A A, Dowson D, Unsworth A, Miller J H, Wright V. An
the radial head includes longitudinal columns of bone that
examination of the elbow articulation with particular reference to
transmit the joint force from the end face of the radius to
variation of the carrying angle. Eng Med 1977; 6: 76–80.
the cortex of the neck.This leads to axial splitting of the
3. Ray R D, Johnson R J, Jameson R M. Rotation of the forearm: an
bone. If the impact energy has still not been fully ab-
experimental study of pronation and supination. J Bone Joint Surg
sorbed, the radius continues to displace proximally, pas-
4. Nordin M, Frankel V H. Basic Biomechanics of the Musculoskeletal
sing posterior to the distal humerus and stripping o¡ soft
System, 2nd edn. PA, London: Lea and Febiger, 1989.
tissues. As this occurs, the axial force falls onto the
5. Basmajian J V, DeLuca C. Muscles alive: their functions revealed by
coronoid process, which may then also fracture. The
electromyography, 5th edn. Baltimore: Lippincott, Williams and
pocket of loose tissue created behind the capitellum al-
lows the radius to escape postero-laterally, with a rota-
6. Long C, Conrad P W, Hall E A, Furler S L. Intrinsic–extrinsic
muscle control of the hand in power group and precision handling.
tional movement into supination and then proximal
An electromyographic study. J Bone Joint Surg 1970; 53A: 853–
translation. Consideration of load transmission along the
forearm, in addition to the joint forces caused by the
7. Amis A A, Dowson D, Wright V. Muscle strengths and
muscles, shows why there is an increasing use of radial
musculoskeletal geometry of the upper limb. Eng Med 1979; 8:
8. Hunsicker P. Arm strength at selected degrees of elbow flexion.
joint against disruption caused by proximal migration of
Wright Air Development Centre, Wright-Patterson Air Force
Base 1955. Technical Report 54–548, Ohio.
9. Amis A A, Dowson D, Wright V. Elbow joint force predictions for
some strenuous isometric actions. J Biomech 1979; 13: 765–775.
10. Elftman H. Biomechanics of muscles. J Bone Joint Surg 1966; 48A:
11. Amis A A, Miller J H, Dowson D, Wright V. Biomechanical aspects
of the elbow: joint forces related to prosthesis design. J Med EngTechnol 1979; 3: 229–234.
The elbow is a complex mechanism and the articular
12. Amis A A, Miller J H, Dowson D, Wright V. Axial forces in the
geometry, kinematics, muscle actions and joint forces
forearm. Their relationship to excision of the head of the radius.
are described in greater detail elsewhere.The forces
In: Stokes IAF (ed.). Mechanical Factors and the Skeleton. London:
on the elbow are much greater than the external forces
exerted by the hand, because of the great mechanical
13. Carlsoo S, Johansson O. Stabilisation of and load on the elbow
joint in some protective movements. Acta Anatom Scand 1962;
disadvantage at which the muscles must act. Forceful ac-
tivities cause co-contraction of all the relevant muscles,
14. Amis A A, Miller J H. The mechanisms of elbow fractures: an
plus further actions to stabilize the wrist and elbow.The
investigation using impact tests in vitro. Injury 1995; 26: 163–168.
muscles all pass approximately along the arm, apart from
15. Knight D J, Rymaszewski L A, Miller J H, Amis A A. Primary
some smaller ones, and so the forces at the elbow are
replacement of the fractured radial head with a metal prosthesis. JBone Joint Surg 1993; 75B: 572–576.
very close to the sagittal plane. The force resultant acts
16. McDougall A, White J. Subluxation of inferior radio-ulnar joint
onto the distal aspect of the humerus when the elbow is
complicating fracture of radial head. J Bone Joint Surg 1957; 39B:
in extension, and moves progressively onto the anterior
aspect as the elbow £exes. This force is shared between
17. Amis A A. Biomechanics of the elbow. In: Wallace WA (ed.). Joint
the radial head and the ulnar coronoid in £exion,
Replacement in the Shoulder and Elbow. London: Butterworths,1998; 103–125.
falls mostly onto the olecranon in extension, and onto
18. Amis A A. Biomechanics of the elbow. In: Stanley D, Kay N R M
the radial head when falling onto the outstretched
(eds). Surgery of the Elbow: Practical and Scientific Aspects.
CELEBRAMOS EL DÍA DE LA ARMADA – 17/05/1814 1. A manera de prólogo 2. Efemérides 3. Noticias del Liceo 4. Noticias del Centro 5. Actualidad 6. Variedades 7. Consejos Útiles 8. Colaboraciones 9. Anécdotas Liceanas 10. Perfilex 11. Proa al Centro en el Recuerdo 12. Galería de Imágenes 13. Calendario de Actividades 14. Contactos Liceanos 15. Bolsa de Trabajo y de Servicios 16. Nuestra base
W hen we think ofglobalisation and its impact,the practices.Pierre Casse,in his book Training for the Cross- images that spring to mind involve American Cultural Mind , develops this idea, describing training infast-food outlets and European bottled water inanother culture as a creative act. Casse presents a triumvi-Third World countries, placard-waving demonstratorsrate model for manag

 c 2003 Elsevier Science Ltd. All rights reserved.
c 2003 Elsevier Science Ltd. All rights reserved.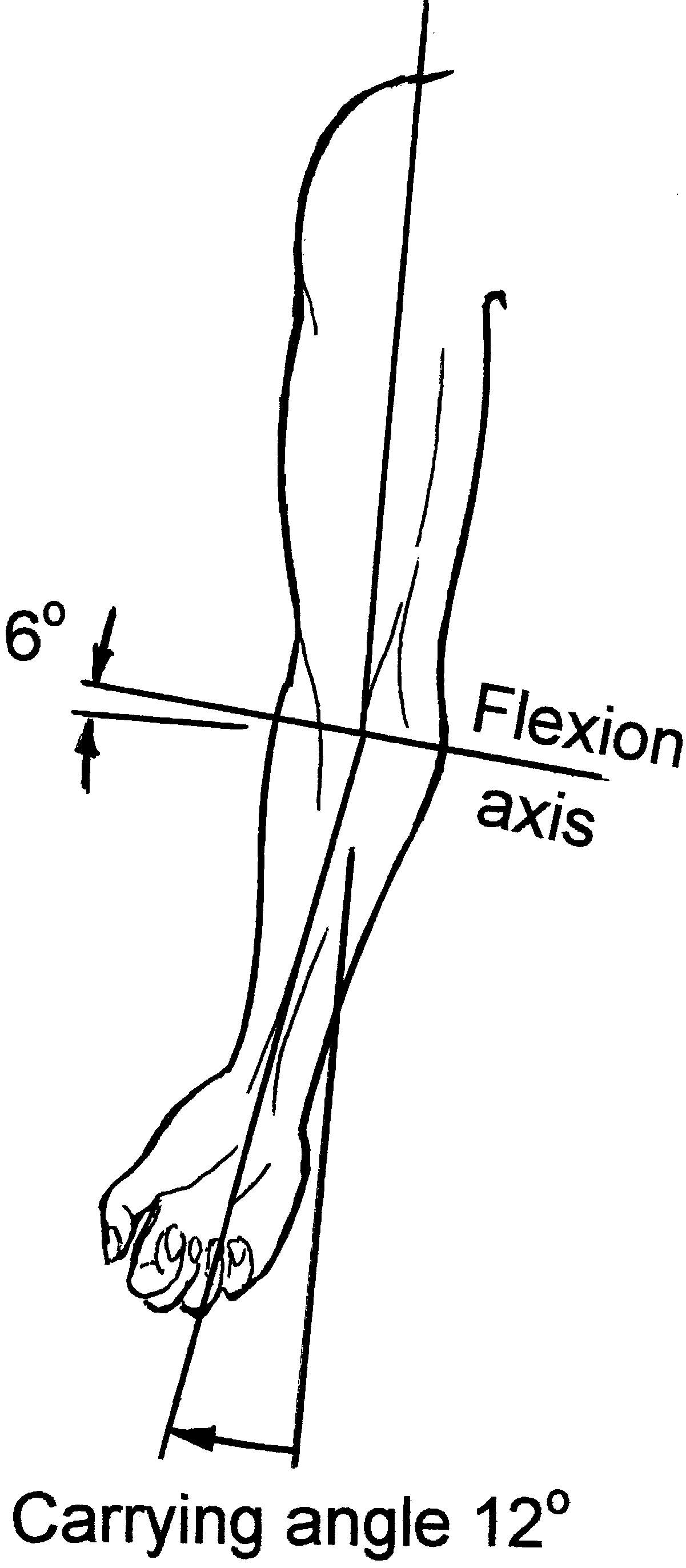 the coronoid process and of the rim of the radial headagainst the £oors of the anterior humeral fossae.
the coronoid process and of the rim of the radial headagainst the £oors of the anterior humeral fossae.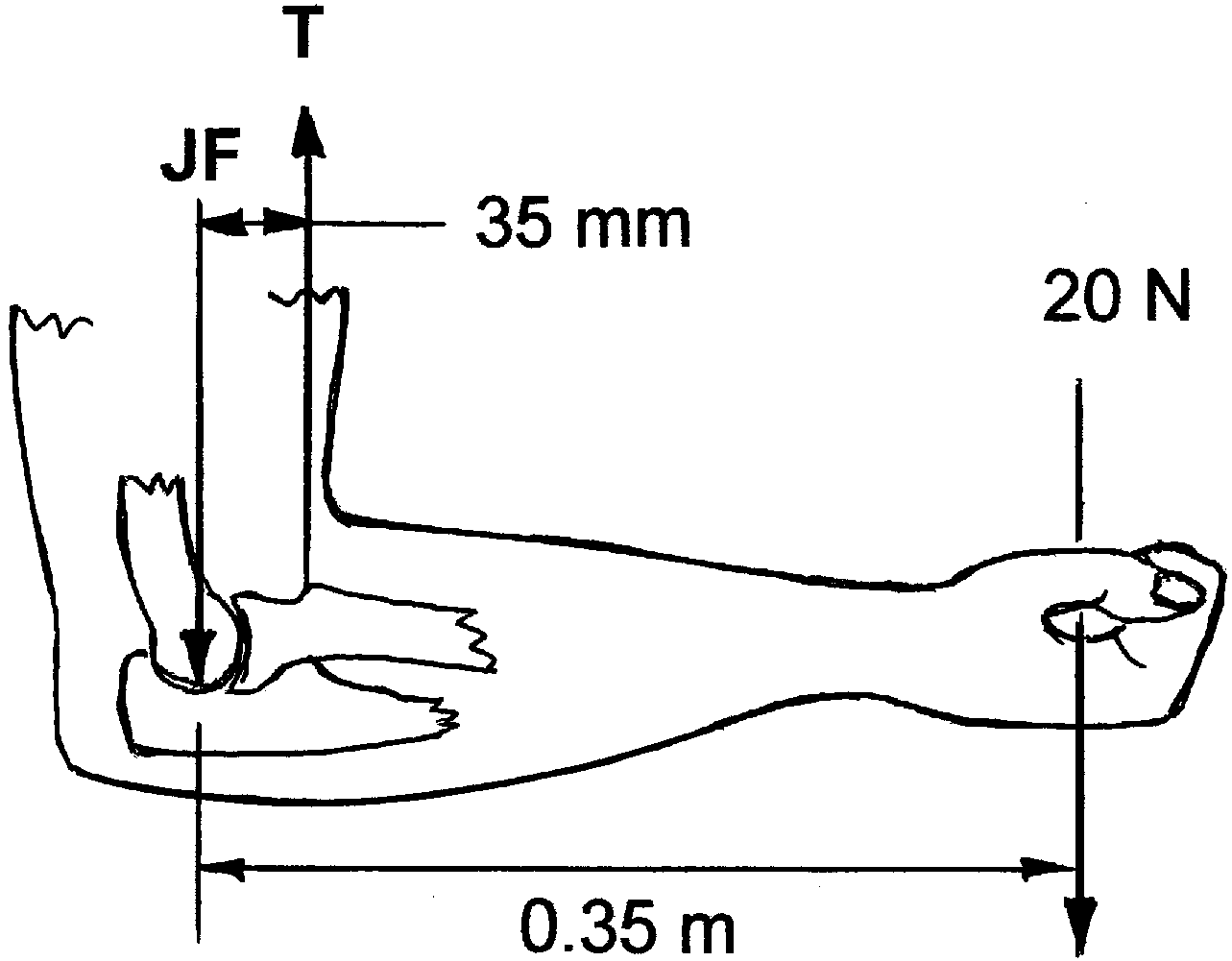 The simpli¢ed example was misleading because it con-
centrated solely on a ‘muscle’ that was parallel to the hu-merus, and this is a natural way to think of the situation,
It was noted in the introduction that the elbow muscles
given that the elbow is £exed by muscles such as biceps
work at a large mechanical disadvantage when compar-
and brachialis. It suggests that the joint forces act onto
ing their small moment arms about the joint axis to the
the end of the humerus. However, considering the hand,
large moment arms of loads exerted on the hand. It fol-
it is clear that there are other muscle actions inherent in
lows that the joint forces will be much greater than the
elbow £exion, to grasp the object being lifted, and to sta-
external forces, and also that they will depend almost en-
bilize the wrist. If the ¢st is clenched, even without the
tirely on the muscle tensions. Therefore, a good under-
hand supporting a load, then the tensions in the ¢nger
standing of which muscles act, and of their paths and
£exor muscles compress the humero-ulnar joint, due to
points of attachment, is central to appreciation of the
£exor digitorum super¢cialis originating from the medial
forces on the elbow. The joint forces in£uence many as-
epicondyle. At the same time, the wrist must be held
pects of clinical treatment, providing insight into why
against the £exion moments exerted by the ¢nger £exor
prostheses loosen or why bone fragments may tend not
tensions, and so there is co-contraction of the extensor
to remain in a reduced con¢guration, for example.
The simpli¢ed example was misleading because it con-
centrated solely on a ‘muscle’ that was parallel to the hu-merus, and this is a natural way to think of the situation,
It was noted in the introduction that the elbow muscles
given that the elbow is £exed by muscles such as biceps
work at a large mechanical disadvantage when compar-
and brachialis. It suggests that the joint forces act onto
ing their small moment arms about the joint axis to the
the end of the humerus. However, considering the hand,
large moment arms of loads exerted on the hand. It fol-
it is clear that there are other muscle actions inherent in
lows that the joint forces will be much greater than the
elbow £exion, to grasp the object being lifted, and to sta-
external forces, and also that they will depend almost en-
bilize the wrist. If the ¢st is clenched, even without the
tirely on the muscle tensions. Therefore, a good under-
hand supporting a load, then the tensions in the ¢nger
standing of which muscles act, and of their paths and
£exor muscles compress the humero-ulnar joint, due to
points of attachment, is central to appreciation of the
£exor digitorum super¢cialis originating from the medial
forces on the elbow. The joint forces in£uence many as-
epicondyle. At the same time, the wrist must be held
pects of clinical treatment, providing insight into why
against the £exion moments exerted by the ¢nger £exor
prostheses loosen or why bone fragments may tend not
tensions, and so there is co-contraction of the extensor
to remain in a reduced con¢guration, for example.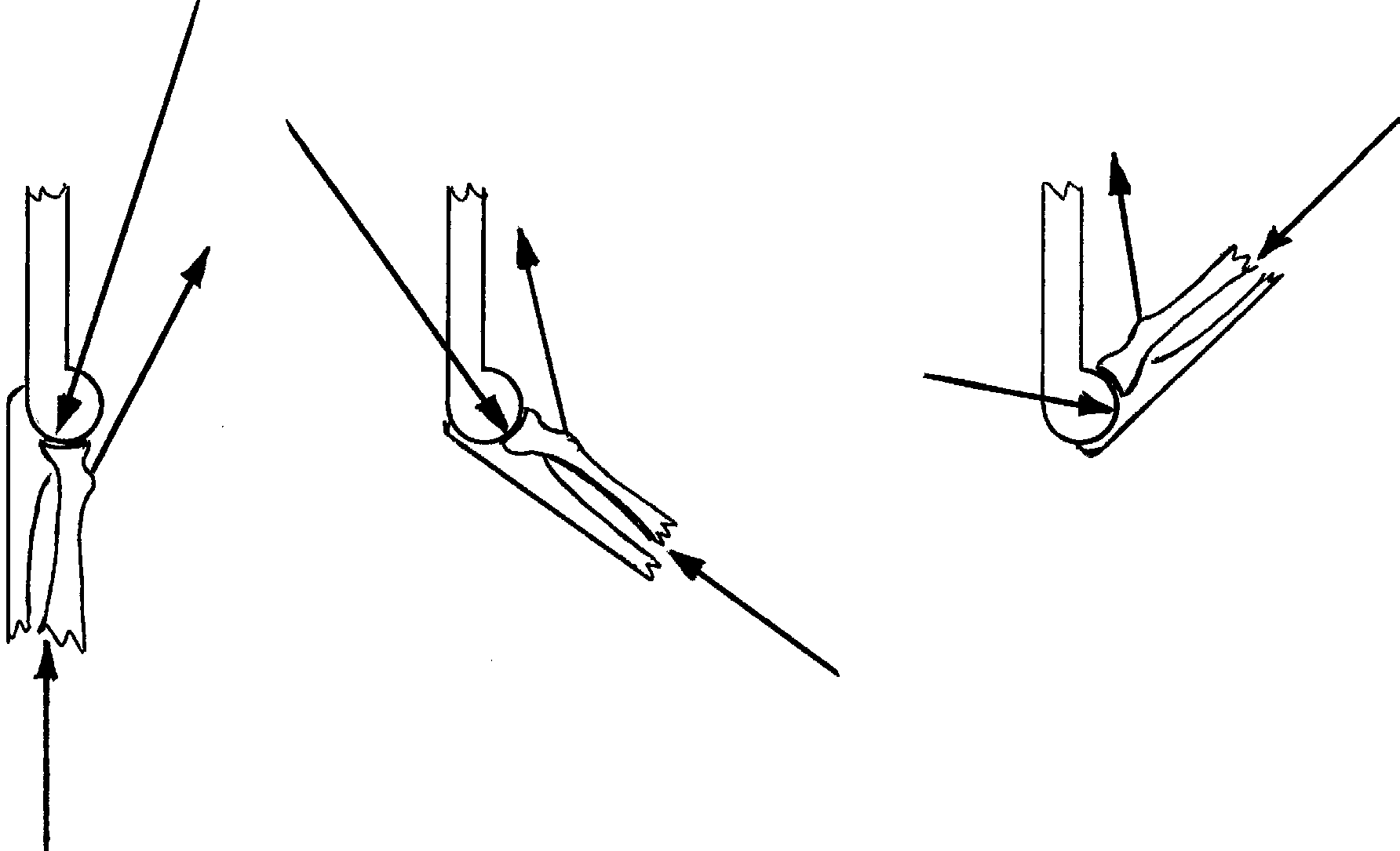
 When triceps tension resists the £exing moment
The force on the distal humerus, during elbow £ex-
from an external load, tensile stresses are caused in the olecra-
ion, is greatest near extension, because the forearm and elbow
non, causing it to be vulnerable to fracture.
When triceps tension resists the £exing moment
The force on the distal humerus, during elbow £ex-
from an external load, tensile stresses are caused in the olecra-
ion, is greatest near extension, because the forearm and elbow
non, causing it to be vulnerable to fracture.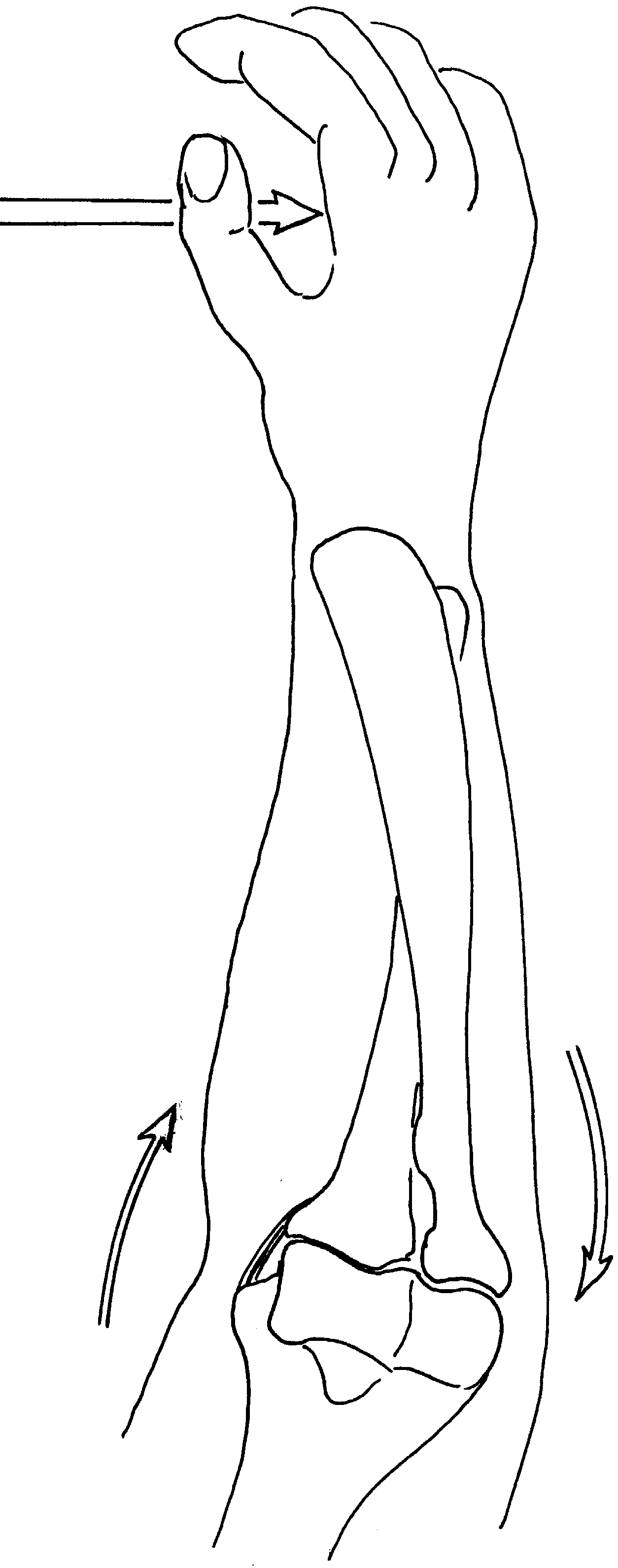 tions have shown that, if the force is directed along thecentreline of the forearm, then approximately 70% of theload is transmitted by the radius directly to the capitel-lum.If the force vector passes towards the lateral sideof the elbow, then all of the load passes directly to theradius and this is a stable situation. If the force passesmedially, the tenuous lateral collateral ligament struc-tures do not maintain stability, but this situation is notnormally encountered due to the carrying angle biasingthe loads to the radial side of the elbow.
tions have shown that, if the force is directed along thecentreline of the forearm, then approximately 70% of theload is transmitted by the radius directly to the capitel-lum.If the force vector passes towards the lateral sideof the elbow, then all of the load passes directly to theradius and this is a stable situation. If the force passesmedially, the tenuous lateral collateral ligament struc-tures do not maintain stability, but this situation is notnormally encountered due to the carrying angle biasingthe loads to the radial side of the elbow.