Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Srs - forms console_apm.xls
New Patient Information Sheet Visit Date: Date of Birth:
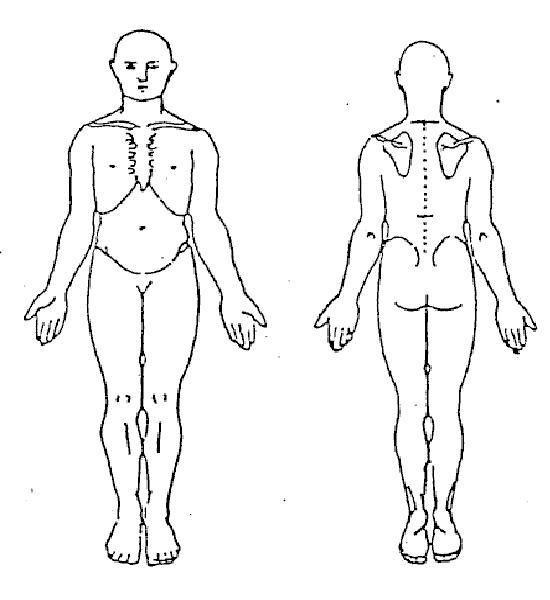
Please fill in the questions below as concisely and accurately as possible. The form may seem lengthy but it is very important to help us understand your paincomplaints. This wil help us provide you with the highest level of care.Primary Care Doctor: Doctor's Name Doctor's Address/Phone Referring Doctor: Doctor's Name Doctor's Address/Phone Pain Medicine Doctor you have seen before: Are there any claims pending or is this Workers Compensation related? List areas of pain: When did your pain begin: How did your pain start: Describe where your pain is: Does your pain radiate anywhere? (Examples: into your arm, leg, chest, abdomen) Circle the words which best describe your pain: Is the pain intermittent? or constant? Date of Birth: Circle the number between 0 - 10 that represents the intensity of your pain: 0 = No Pain 5 = Interferes with activities 10 = Worst pain imaginable Average Pain = Worst Pain = What makes pain worse? What makes pain better? Pain Diagram: Stabbing: / / / / / Burning: XXXXX Pins and Needles: 0 0 0 0 Aching/Throbbing: ^ ^ ^ ^ ^ Numbness: = = = = = Other: …… . Date of Birth: What pain medications have you tried: Medication Still Using Stopped Because Date of Birth: Please list other pain medications tried: Medication Still Using Stopped Because What treatments have you tried Procedure How Long Ago Effective? (Y/N) List ALL Surgeries: Hospital List ALL Medical Problems: (Include any diagnosis of anxiety or depression) Medical Problem Treating Doctor Telephone Number Date of Birth: List ALL Medications you're taking: Frequency List ALL Medication Allergies Reaction Are you allergic to iodine or x-ray contrast? Is your mother List major illnesses Age and cause of death Is your father List major illnesses Age and cause of death Divorced Do you have any children? Please list. Son/Daughter Medical Problems Are you employed? Yes If Yes: What is your job? Date of Birth: Are you: Disability How long ? List your hobbies and interests: Does your pain stop you from the things you enjoy? Do you smoke? If yes, how much? Do you use any illegal drugs? If yes, what? Do you drink alcohol? If yes, how much? Have you ever felt you should cut down drinking alcohol? Have people annoyed you by criticizing your drinking? Have you ever felt bad or guilty about your drinking? Have you ever had a drink first thing in the morning to steady your nerves or get rid of your hangover? Do you have any of the following symptoms: General/Constitutional: If yes, explain. If yes, explain. If yes, explain. Skin/Allergy: If yes, explain. If yes, explain. Sweating If yes, explain. Musculoskeletal: Joint stiffness If yes, explain. Joint/bone pain If yes, explain. Joint swelling If yes, explain. Muscle cramps If yes, explain. Headaches If yes, explain. Dizziness If yes, explain. Fainting If yes, explain. Date of Birth: Sensitivity to light If yes, explain. Sinus congestion If yes, explain. Nose bleeds If yes, explain. Bleeding gums If yes, explain. Mouth ulcers If yes, explain. Endocrine: Neck swelling If yes, explain. Heat/Cold intolerance If yes, explain. Weight loss/gain If yes, explain. Appetite change If yes, explain. Male erectile problem If yes, explain. Abnormal Bleeding / Discharge Pain If yes, explain. Respiratory: Wheezing If yes, explain. If yes, explain. Short of breath If yes, explain. Cardiovascular: Chest Pain If yes, explain. Palpitations If yes, explain. Lew Swelling If yes, explain. Hematological: Easy bruising If yes, explain. Easy bleeding If yes, explain. Abnormal clotting If yes, explain. Lymph Nodes: Enlargement If yes, explain. Tenderness If yes, explain. Gastrointestinal: Difficult swallowing If yes, explain. Heartburn If yes, explain. Constipation If yes, explain. Diarrhea If yes, explain. Change in stool If yes, explain. Date of Birth: Genitourinary: Painful urination If yes, explain. Difficult urination If yes, explain. Urgency/frequency If yes, explain. Incontinence If yes, explain. Blood in urine If yes, explain. Neurological: Fainting If yes, explain. Weakness/paralysis If yes, explain. If yes, explain. Headaches If yes, explain. Migrains If yes, explain. Psychiatric: Depression If yes, explain. Suicidal thoughts If yes, explain. If yes, explain. Sleep disturbance If yes, explain. Patient Signature Person filling in form if different from patient Relationship Continuation Information (if required) Provider Signature:
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:656 – 664Effectiveness of Proton Pump Inhibitors in Nonerosive RefluxBONNIE B. DEAN,* ANACLETO D. GANO, JR.,* KEVIN KNIGHT,* JOSHUA J. OFMAN,*,‡ andRONNIE FASS§*Cerner Health Insights, Beverly Hills, California; ‡Cedars-Sinai Medical Center, Department of Medicine, Los Angeles, California;and §Southern Arizona VA Health Care System, Tucson
Although none of the original manuscripts writ-Lord’s supper) as practiced by the early church ten by Moses or Paul or the other biblical writers prior to the circulation and collection of the New have been preserved (no doubt providentially; oth-Testament books, with their initiation as described erwise they might have become objects of worship), therein, can only be explained if the doc
 Date of Birth:
Date of Birth: