Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
C:\osman sankoh\health intervention trials\detailed site profiles\african sites\farafenni profile.pdf
Farafenni Demographic Surveillance System (Member of the INDEPTH Network) Profile of the FARAFENNI DSS, THE GAMBIA March, 2004 1. Physical geography and Population Characteristics of the Farafenni DSA
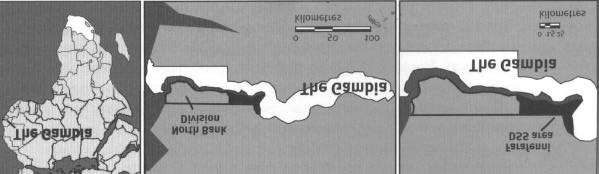
The Gambia is the smallest continental country in Africa, with a land area of just 10 360 km2 (480 km from east to west and on average 48 km from north to south) and a total population of 1.4 million in July 2000 (Figure 1). It is surrounded by Senegal, with which it once shared a short-lived federation (‘Senegambia”), from 1982 to 1989. The town of Farafenni is on the north bank of the Gambia River, about 170 km inland from the capital, Banjul. The main road between Dakar and the Casamance crosses the Gambia River at Farafenni, which has a ferry suitable for heavy vehicles. The average annual rainfall, measured at the Farafenni field station in 1989-99, was 683 mm, but the relative variability is large (22.6%), with amounts in the 11-year period ranging from 515 mm in 1991 to 1000 mm in 1999. The Gambia has a single rainy season, extending from June to October, with peak rains in August. The vegetation is dry savannah, with scattered trees, but in the rainy season, grasses and bushes grow strongly. Rice is cultivated in the river bottoms and in the upland areas where millet, sorghum, and other cereals are the staple food crops. Figure 1: Location of the Farafenni DSS site, The Gambia.
2. Population characteristics of the Farafenni DSA
The surveillance site is located in a rural area between latitudes 130 and 140N and longitudes 150 and 160W and comprises 40 small villages, extending 32 km to the east and 22 km to the west of the town of Farafenni (1993 population, 21,000). The UK Medical Research Council (MRC) has studied the population of the 40 villages since October 1981. The villages were originally selected for the study of malaria interventions requiring little previous use of antimalarials, which meant that larger villages and those within about 10km of the town of Farafenni were initially not under surveillance until July 2002 when Farafenni and its satellite Gambian villages within a 5-km radius became part of the DSS. This new segment of the demographic surveillance area (DSA) is designated the “urban” area so as to distinguish it from the initial 40 rural villages. The total population under surveillance as at 31 December 2002 was 16,883 in the rural part of the DSA comprising of 8,965 females and 7,918 males; and 26,008 in the urban part made up of 13,503 females and 12,505 males. These represent 39% and 61% respectively of the total surveillance population of 42,891. Both areas manifest an age structure characterised by youthfulness and fairly rapid growth rate (Figure 2), thus indicating a relatively constant but high level of fertility. At least 15% of the residents of each part of the DSA are under 5 years of age; and 45% and 43.4% are below the age of 15 in the rural and urban areas respectively. Half the women Farafenni DSS - Rural Farafenni DSS - Urban Age Group 35-39 Age Group 35-39 Population Population Figure 2: Age structure of the Farafenni surveillance population by area.
in the urban area (50.3%) fall within the reproductive age bracket of 15-49, compared with 44.8% in the rural area. The only structural difference between the two populations is in the sex ratio between the ages of 35 and 64 years (Figure 3). Whilst there were fewer males than females between the ages of 15 and 35 years in both populations, the rural population manifested a consistent sex ratio of about 80 males or less per 100 females for all ages over 35. The urban population, on the other hand, displayed a higher proportion of males than females among residents aged 45 and 69 years. The sex
Sex Ratio by Age Sex Ratio Figure 3: Sex ratio of the Farafenni surveillance population by age-group and area.
ratios in this age bracket ranged from 119 among those aged 45-49 to 160 among urban residents aged 55-59. The most probable explanation of the disparities in sex ratios between the two populations is the difference in their respective levels of net migration. The town of Farafenni serves as a destination point for migrants from the rural part of the DSA as well as other villages outside the DSA; whereas the rural area of the DSA is a migration source for the town of Farafenni, other growth centres such as Kerewan and Kaur, and the Greater Banjul Area. As a result, the urban part of the DSA will be expected to have more immigrants than outmigrants, whereas the reverse will be the case in the rural area. What remains to be established is whether the high proportion of males relative to females aged 45-49 in the urban area is due mainly to the influx of males into Farafenni town, or whether it is accompanied by a significant exodus of females within that age bracket outside of Farafenni town. The surveillance population comprises mainly of three ethnic and linguistic groups, viz.: Mandinka (about 43%), Wollof (36%), and Fula (20%). Nearly all of the residents are Muslim. Farming is the primary occupation of most residents, both male and female. In a 1998 survey, men were asked about their main occupations: 92% said farming, 12% said a trade or craft, and 9% said some form of trading, or commerce. The population is poor. In June-July 1996, a survey of household heads revealed that only 61% had radios, 44% slept on iron or wooden beds, 35% had carts, and 40% still had homes with thatched roofs (Hill et al. 1996). Nine primary schools serve the rural part of the DSA. Many children have to walk up to 5 km to school, which restricts school attendance. In a 1998 survey, just 10% of the men =18 years old and 3% of the women 15-54 years old had ever attended school. In a 2000 survey of household heads, only 54% of households with school-age children reported any children attending school. Villages are organized into compounds containing up to 149 people, with an average of 18 persons overall. A compound is based on an extended family unit, headed by a senior man. Residents might include the head’s brothers or sons and their and his own wives and children. Polygyny is widespread: 40% of married men were polygynous in 1998, with an average 2.6 wives each. Co-wives very often reside in the same compound, together with their children. Additional compound residents include distant relatives or non-family members, such as foster children or Quranic scholars. Compounds consist of a group of buildings bordered by some kind of fence. Most houses are constructed of mud-brick walls, with either thatched or corrugated-metal roofs; cement buildings are rare. Kitchens and other buildings are more commonly made from Krinting (woven lattice work) and thatch. Water is usually gathered from a common pump well (82% of compounds), but 12% of compounds still rely on traditional wells, with buckets and ropes. The pump wells became a common feature of most villages after the late 1980s. Most compounds do not have standard latrines, but sonic have a simple hole in the ground that is used by adults more often than children. None of the villages has electricity. A single graded road runs east-west on the North Bank of the river from the eastern part of the country, through Farafenni to Barra on the coast, the crossing point for Banjul on the opposite shore. Unimproved tracks link this road to the villages. An intermittent public bus service began in 1986, along the main north-bank road. Most villagers walk to Farafenni, but horse and donkey carts and a few privately owned bush taxis provide transport to the town, especially on market day (Sunday in Farafenni). The study villages have no telephones, but three of the nearby larger villages not in the surveillance system have public payphones. Village-based primary health care was begun in The Gambia in 1981. A health centre was established in the town of Farafenni in 1983, and in 1998 it was upgraded to become the third hospital in the country. The hospital has 155 beds and provides essential medical, paediatric,
obstetric, gynaecological, surgical, and ophthalmic services. Before these services were available in Farafenni, patients had to be transported to the Royal Victoria Hospital in Banjul, using the ferry and an ambulance or bus service. In the early 1980s, the health centre was staffed by a team of two to four physicians from China, but at present, MRC physicians and Cuban doctors support the hospital’s clinical services. At two dispensaries closer to the study villages, patients can be seen and referred to Farafenni. The town has a few private dispensaries and pharmacies. Eight paid community-health nurses (CHNs) serve the area and supervise the volunteer traditional birth attendants (TBAs) and village health workers (VHWs), who form the base of the primary health care (PHC) program. CHNs manage maternal and child health (MCH) clinics, including five monthly mobile clinics in study villages and two static weekly clinics accessible to residents of the study area. All villages with a population of more than 400 persons are eligible to become PHC villages, with a resident TBA and a VHW, but this depends on the level of commitment and organization of each village. Fifteen of the 40 villages within the Farafenni DSS have been designated PHC villages. The district health-management team, with support from MRC physicians, maintains weekly clinics in two larger villages, one to the east and the other to the west of Farafenni. The MRC fieldworkers use referral forms to encourage needy residents of the study area to attend these clinics. User fees are charged for all these public health services. Maternal- and child (under-five)-health services are available after buying a child-health or antenatal card for 5 dalasi (in January 2004, 32.00 Gambian dalasi [GMD] = 1 United States dollar [USD]). The clinic fee for children 5-14 years old is 1 dalasi; and for adults, 5 dalasi. Admission fees at the hospital for adults (free for children <5 years old and pregnant women) are 25 dalasi a week, and for major operations, the fee is 50 dalasi. Immunization levels in the study area are fairly high: 88% of children had been vaccinated against tuberculosis by 1 year old; 75%, against DPT3 by 2 years old; and 64%, against measles by 2 years old (unpublished data). Virtually all women in the study area who delivered babies in 1998 had received some antenatal care, with the mean number of visits at 3.5 for each woman. The first visit occurred fairly late in the pregnancy, on average at 5.7 months. Twenty percent of all deliveries in 1998 were attended by a health professional, 51% by a TBA, and 25% by a relative, but 4% of the women delivered “on their own.” Based on preliminary reviews of verbal autopsies (VAs) for 1998 and 1999, the most frequent cause of death in infants was acute respiratory infection (ARI), whereas in children 1-4 years old it was malaria. These two conditions accounted for about half of the deaths in children <12 years old. Other leading causes of death were acute gastroenteritis, malnutrition, anaemia, and septicaemia. For adults, major causes of death during 1999 were ARI, gastroenteritis, tuberculosis, cardiovascular disease, and malignancies. Maternal mortality is still an important cause of death in women of reproductive age. Very few AIDS deaths have been reported. The MRC Farafenni field station is currently a base mainly for work on malaria, trachoma and reproductive health. Although not all of the work conducted at the station involves the surveillance villages, very often research projects include at least one of the study villages. Additional data can be readily added to the surveillance data, as all studies use the permanent ID number for individuals.
3. Farafenni DSS procedures
3.1. Introduction to the Farafenni DSS site
Since October 1981 MRC has maintained the Farafenni DSS as a surveillance site for both demographic and health data. At its inception, the primary objective of the project was to monitor the impact of the Gambian PHC program on outcomes of pregnancy and child survival. Surveillance of births and deaths began in April 1982, after the completion of the original census. The 16 larger villages of the area joined the PHC program in early 1983. Another MRC objective was to monitor malaria morbidity and mortality within the area and consider ways to link malaria interventions with the PHC program. Large villages and towns with drug sellers and access to drugs in 1981 were thus excluded from the study area, as antimalarial drugs were available outside the government system. The site has been used to answer a range of scientific questions and a search of the literature using the names of the main investigators quickly reveals more than 100 published papers and reports. Here, we refer to just a few key publications to provide an introduction to some of the research output from the site. The initial work on malaria prophylaxis is summarized by Greenwood et al. (1989). The ability of village health workers to provide this prophylaxis was examined by Menon, Snow et al. (1990). Later work included studies of chloroquine resistance (Allen et al. 1990; Menon, Otoo, et al. 1990). Work in the early 1990s was mainly on issues such as malaria prophylaxis and iron supplementation in pregnancy (Greenwood et al. 1994; Menendez, Todd, Alonso, et al. 1994; Menendez, Todd, Alonso, Francis, et al. 1994; Greenwood et al. 1997). More work on the effectiveness of impregnated bednets and treatment of malaria was conducted in the Farafenni villages (Müller et al. 1996). Over the last few years, much of the malaria work has focused on reduction of Plasmodium falciparum malaria transmission (Targett et al. 2001; von Seidlein et al. 2001). The progress of the PHC program was evaluated using the study villages (Greenwood et al. l990a, b) and was looked at in greater detail by Hill et al. (1998) and Hill et al. (2000). In 1992 and 1994 studies were conducted on fertility and its proximate, as well as its cultural, determinants (Bledsoe et al. 1994; Bledsoe et al. 1998). In the mid- and late 1990s, a new focus for work in the study villages was adult health. A comparative study of non-communicable disease among adults in Banjul and the study villages was completed in 1997 (van der Sande et al. 2000; Nyan et al. 2001a, b; van der Sande et al. 2001; Walraven, Nyan et al. 2001). The MRC reproductive health program included a major field study using interview, clinical, and laboratory methods, covering about half of the resident female population of reproductive age (Walraven, Scherf et al. 2001). Maternal mortality was examined by Greenwood et al. (1987), Graham et al. (1989), Greenwood et al. (1990a), and more recently by Walraven et al. (2000). The program included a demographic study of the fertility and reproduction of men in 1998-99 (Ratcliffe et al. 2000). 2.2. Farafenni DSS data collection and processing
The surveillance system was originally set up to follow the population of young children, rather than monitoring the demography of the general population. Since then the surveillance has expanded to include information on all residents of the study area, adults and children. In 1986, one village withdrew, after a misunderstanding about the collection of blood samples for a cross- sectional survey.
In 1998, the surveillance system was converted to the household-registration system (HRS), originally developed for use in Navrongo, Ghana. New field- and data-management procedures were implemented at conversion, as described below. Before the HRS, censuses were conducted biennially, and data were collected on an ongoing basis through village recorders (citizens of the villages), with regular visits from fieldworkers. Since 1998 fieldworkers have visited each compound to collect data on vital events, at least once every 3 months. The most recent census was conducted in 2000. Field procedures MAPPING — Maps of the villages were last revised in 1998. New compounds are added to the maps as changes are observed during the census rounds every 3 months. The latitude and longitude of all villages and compounds have been established using hand-held GPS devices. Work is under way to link these coordinates with other maps, including those available from satellite photography. INITIAL CENSUS — The initial census was begun in October 1981, but it is impossible to identify the population originally enumerated, because until April 1989 the census was updated without archiving. Censuses are conducted in the study area biennially. During these censuses, fieldworkers visit every compound to verify and update information on all residents. Fieldworkers use a roster of all current residents and previous residents who have migrated. New residents are added, after it has been established that they are not temporary visitors. Since the inception of HRS one census has been conducted, in 2000. This census was different from the normal HRS rounds every 3 months, in that the HRS team of fieldworkers was expanded, and this enlarged team worked together with the field supervisor in each village. REGULAR UPDATE ROUNDS — Since the conversion to the HRS three fieldworkers are responsible for the surveillance, under the direction of a field supervisor. Each fieldworker is responsible for updating a specific set of villages in which they are resident. Fieldwork is organized into a series of 3-month periods, called rounds. Fieldworkers visit each compound at least once in every round. Working from a list of all residents for each compound, the fieldworkers verify and update the recorded information with the compound head or another senior adult. These printed lists are organized by village and are filed in binders that the fieldworkers take with them to the field. These lists are updated and reprinted each year. Village recorders who were originally responsible for reporting vital events for their villages are still involved in the fieldwork. They continue to provide a useful point of contact for the fieldworkers and help with outreach and sensitization, explaining new studies and passing on research findings to the villagers. CONTINUOUS SURVEILLANCE — All deaths, births, migration within or beyond the study area, pregnancies, and marriages are recorded during the rounds that are made every 3 months. The files on individuals also include information on their enumerated parents and husband (if married). Pregnancies are followed for outcomes of miscarriage, still or live birth, and more complete
coverage of neonatal deaths. Information on pregnancies is collected from TBAs, MCH clinics, and regular updating rounds. Marriages are recorded for women because of the complexity of recording data on several wives for polygynous men. Men can be linked to their wives easily within the HRS system. VAs are conducted for all deaths. Children’s deaths have been followed with VAs since 1998. Deaths of women of reproductive age as far back as 1993 were studied in 1998. All deaths of adults are also followed with a VA. Socioeconomic surveys were conducted in 1996 and 2000. Often a round will include some additional questions to complement the basic surveillance. Recently, this included a set of questions on perceptions of mortality change since the early 1980s. FIELD SUPERVISION AND QUALITY CONTROL — Weekly meetings are held with the senior staff responsible for the HRS and the field- and data-management team to sort out queries and procedural issues. Errors identified during data entry and checking using the HRS are referred to the fieldworkers for resolution during the succeeding week. Data management and analysis At the outset, the data were recorded in paper ledgers organized by compound. Snow and Rowan converted the older ledgers to dBase II computer files, readable on BBC Torch, and then on IBM personal computers running dBase III. The initial numbering system was based on the Matlab system (Bangladesh), with all compounds numbered sequentially from 1 to more than 900. In 1992, the compounds were remapped and renumbered, replacing the old survey number with a new survey number that included village, compound, and personal identifiers arranged in a hierarchical sequence. Starting in 1989, the data were saved in a “frozen” census every March 31. For the period before tire frozen-census files were archived, it is impossible to calculate the person-years accurately, although data on birth and death events are available from April 1982 onwards. Vital rates for this earlier period have to be taken from published reports. As the census years begin on 1 April each year, nine frozen-census rounds occurred from 1989 to 1997, and these provide the raw data for estimating birth and death rates for this period. These flat files can be linked, but before conversion to HRS, this was cumbersome and time-consuming, and the calculation of person-years of exposure remained problematic because of the lack of detail on the dates of migration. The routine surveillance was checked every 2 years by conducting a full re-enumeration of the entire study site, and this enumeration often led to corrections in the older data and thus to some minor changes in the resulting annual rates. In 1998, full conversion to HRS was completed. The detailed conversion tasks required close examination of the quality and the consistency of the archived data. Dates of death, for example, were compared with the status variable “dead” to reveal inconsistencies. The discrete census files in dBase were cleaned and linked chronologically before the conversion to HRS. The decision was made to merge the frozen-census fields backwards from the 1997 frozen census, on the assumption that the most recent data were the most accurate (MacLeod 1998). After being merged, the data were rechecked for missing or impossible codes, and corrections were made, as necessary. The number of changes was not large, but they took many hours to check, both in the office and in the field. The final merged files contained information on 30,460 individuals, recorded since 1981. Some complex checks were applied using SAS software to deal with residents missing in one census and recorded in a subsequent enumeration or vice versa. The late recording of some vital
events, missed by fieldworkers but picked up during a re-enumeration, still poses a challenge for analysts eager to calculate rates based on true person-years of exposure. After careful merging and checking of the archived data — the “legacy” data in HRS parlance — the original dBase fields were converted to the data sets used in HRS. The HRS version in use in Farafenni was modified, and this included the conversion of the older variable names to new names used in HRS. Several new variables were not on the original dBase fields and had to be collected from the field (husband’s ID, pregnancy outcome) or inferred from other variables (household status, migration types). All these tasks were accomplished in 1998 and since then, both the office and field procedures are driven by the demands of HRS. Within FoxPro, files can be easily constructed to link individuals to their relatives or other members of social groups, such as a compound. The moves of individuals in and out of the study area several times in a single year can now be properly recorded, whereas the previous system was only able to record one migration event in a census year. The HRS includes extensive data validation and consistency checks even at the data-entry stage. Individuals are considered eligible for enumeration if they expect to he resident in the study area for at least 6 months and are present during the rainy season. A seven-digit permanent ID number uniquely identifies all individuals, including information on their village and compound of enumeration, as well as a unique personal identifier. Information on individuals includes name, sex, ethnicity, date of birth, parents’ ID (if parents were enumerated), village, compound, and household of residence, residency status, and date of status change. The IDs of husbands are linked to those of their wives. Individual village (alkalo), compound, and household heads are also designated. Pregnancies and pregnancy outcomes are recorded. All updates are recorded directly on the lists of individuals that the fieldworkers take to the field. The field supervisor checks these lists. The data-entry clerk responsible for the HRS checks every entry and is responsible for all queries. All data are now entered directly into the HRS. Internal validity checks are performed at the data-entry stage. Back-up copies are made frequently. Queries are sent back weekly to the field through the field supervisor. During re-enumeration, major discrepancies are reviewed, and changes are made if appropriate. Any proposed changes to individual records not associated with a demographic event (such as name or birth-date changes or deletion of suspected duplication of individual records) are submitted by fieldworkers as a “petition for change,” and these are considered using information from the field and the history recorded in the HRS. Senior scientists attached to the relevant unit perform data analysis. The programs in the HRS are useful for basic rates and ratios, but additional analysis with SAS, STATA or SPSS software is needed for more detailed work. The FoxPro system greatly facilitates the construction of flat files for these analyses. Results are shared at village meetings, meetings with local health workers, and seminars with policymakers. Analyses are submitted for publication in peer-reviewed journals, and findings are presented at international conferences and meetings.
4. Farafenni DSS basic outputs
4.1. Demographic indicators
Fertility
Earlier fertility studies conducted in the rural communities of the Farafenni DSA indicate a total fertility rate of 7.5 births for women aged 15-54 for the period 1987-1992. However, the DSS database reveals a total fertility rate of 5.37 births for the entire rural DSA for the period 1993- 1997; and 6.15 births for 1998-2002. Comparing these levels of fertility with estimates of 6.8 and 6.0 births for the Local Government Area of Kerewan (where the DSA is situated) and The Gambia respectively based on the 1993 Population and Housing Census, it can be argued that the total fertility rate in the rural part of the DSA may have never been below 6 births per woman. Age-Specific Fertility Rates FDSS, Rural ASFR 0.15 1993-1997 1998-2002 Figure 4: Age-specific fertility rates by period for the rural DSA.
The relatively lower estimates obtained, especially for the period 1993-1997, may be due to under-registration of births by the surveillance system. The increase in fertility observed between the two quinquennia should cautiously be interpreted as an improvement in the registration of births in the later period, which is clear from the comparison of age-specific fertility schedules for the two periods shown in Figure 4. Far fewer births were recorded in the period 1993-1997 for women aged 25-29, the age-group in which both the mean and median ages of childbearing are expected to fall for high fertility populations like that of the rural part of the DSA. The schedule for 1998-2002 is
plausible but does not provide much information as to the degree of under-registration of births during the period. Mortality Previous analyses of the DSS data relating to earlier periods of the system have shown evidence of marked improvements in childhood mortality, especially in Primary Health Care villages (Hill et al., 2000). A life table analysis of the deaths documented by the system in the period 1993-2002 yields childhood mortality and life expectancy indicators shown in Table 1.
Table 1: Childhood mortality indicators and life expectancy at birth in the rural DSA.
∗ per 1,000 live births; † per 1,000 population. Infant mortality rate, 1q0, was estimated at 76 per 1,000 live births in the rural part of the DSA between 1993 and 1997. Overall under-5 mortality rate, 5q0, for the same period was 190 per 1,000 live births. This implied a child mortality rate (4q1) of 124 per 1,000 population, thus indicating that children in this part of the DSA had a higher probability of dying between exact ages 1 and 5 than in infancy. This rather unusual pattern of childhood mortality, whose cause-of-death structure is yet to be established, has been shown to be unique to the Sahel West African region (Ahmad et al., 2000; Bicego and Ahmad, 1996; Blacker et al., 1985). This implies that the FDSS, which is geographically located in this region and depicts such a characteristic, has documented reliable records relating to deaths under the age of 5 years. The extent to which the estimated levels are affected by the under-registration of births mentioned in the previous section will have to be investigated in due course. Similar estimates for the period 1998-2002 show the same pattern of childhood mortality with significant improvements in terms of levels, especially between exact ages 1 and 5. Overall under-5 mortality rate for this period was 168 per 1,000 live births, representing a decline of about 12% over the previous quinquennium. For comparison purposes, a sample survey conducted in 1990 estimated under-5 mortality levels in the Kerewan Local Government Area and The Gambia as a whole at 129 per 1,000 (Republic of The Gambia, 1993). The mortality experience at all ages yielded a life expectancy at birth of 49 years or males and 51.7 years for females for the period 1993-1997. These estimates compare reasonably well with those obtained for The Gambia from the 1993 Population and Housing Census (Central Statistics Department, 1998). Both sexes recorded gains in expectation of life in the subsequent five-year period 2.4% for males and 5.2% for females reflecting the improvements in mortality, especially among children under 5 years of age.
The age-specific mortality schedules for the rural residents of the DSA are presented in Figure 5 by sex for the two quinquennia. They manifest the usual “J”-shaped mortality curve characteristic of human populations. Female mortality is generally lighter save for the early childbearing ages where, for developing rural societies such as the one being discussed here, a
Age Pattern of Mortality Age Pattern of Mortality FDSS, Rural: 1993-1997 FDSS, Rural: 1998-2002 q q Both Sexes Both Sexes Figure 5: Age pattern of mortality in the rural part of the DSA by sex and period.
significant number of maternal deaths can occur. The exceptionally low mortality level for males aged 25-29 in 1998-2003 is implausible, thus raising questions on the quality of mortality information relating to adults collected by the system during that period. Trends in maternal mortality In the 1980s, three studies used the surveillance system to estimate the level of maternal mortality in the region. In the first study, between April 1982 and March 1983, all pregnancies in the area were followed prospectively, and the maternal mortality ratio was estimated at 2,362 per 100,000 live births (with wide confidence intervals, as a result of small sample size) (Greenwood et al. 1987). In the second study, a reproductive-age mortality survey of all deaths in women between April 1984 and March 1987 estimated a maternal mortality ratio of 1,091 per 100,000 live births (Greenwood et al. 1990a). The third study, conducted in the fall of 1987, was a field trial of the sisterhood method in six of the villages in the Farafenni surveillance area, and it documented a maternal mortality ratio of 1,005 per 100,000 live births for the mid-1970s (Graham et al. 1989). During the 1993-98 period, 74 female deaths were recorded among women 15-49 years old, and 18 were classified as maternal deaths (25.7%). In the same period, 4,245 live births occurred, corresponding to a maternal mortality ratio of 424 per 100,000 live births, less than half the levels reported from studies in the 1980s. The level of maternal mortality has decreased in both PHC villages (with trained TBAs) and non-PHC villages (with no trained TBAs), with the two sets of villages showing no significant difference. Although impossible to ascertain with certainty, the decrease is probably related to a combination of increased availability of essential obstetric care, improved transport, and increased communication (Walraven et al. 2000).
5. Capacity for Conducting Clinical Trials 5.1. MRC Scientific Co-ordinating Committee
All research projects undertaken at the MRC Laboratories are assessed for their scientific merit by the Scientific Co-ordinating Committee (SCC) and for their compliance with the ethical standards by the Gambia Government/MRC Joint Ethics Committee (see section 5.2 below). Researchers present their project proposals in a standard format at the monthly SCC meeting, where they are discussed and reviewed. Approval by the Committee is required before any research activity is undertaken. Additionally, letters amending or updating existing projects are reviewed to ensure that the SCC is fully aware of every development in the research of the MRC Laboratories. Once approval has been given, every proposal is forwarded to the Ethics Committee for their views. The members of the Scientific Co-ordinating Committee are drawn from the staff of the MRC Laboratories, including those at the Field Stations, reflecting expertise not only in scientific research but also in a range of areas such as technical services and resource management. Discussions are frank and lively, with contributions from all areas of expertise, and this challenging form of peer review ensures that the high standard of the research of MRC Laboratories is maintained. 5.2. The Gambia Government/MRC Joint Ethics Committee
The Gambia Government/MRC Joint Ethics Committee is accountable to the Director of the Department of State for Health (DoSH) and to the Director of the MRC Laboratories, The Gambia. The Committee consists of 11 members: a Chairman, 4 members nominated by each Director (one of each four is a lay member who is not an employee of the respective institution) and the two Directors. The Directors, with the Chairman, nominate from the members one who acts as Scientific Advisor to the Chairman who acts as his/her deputy. The Chairman and members are appointed following consultation between the Directors. The Chairman is independent of both institutions. Members serve for an initial period of 2 years, which may be renewed for a further 2-year period and exceptionally for longer.
The Committee reviews research projects to be undertaken under the auspices of the MRC Laboratories, The Gambia by either members of the unit or attached workers. The Committee also reviews ethical aspects of other research work to be carried out in The Gambia if requested to do so by the Director of Medical Services, Department of State for Health, or his deputy. The quorum for a meeting is the Chairman, or his deputy, and three members, one of whom must be a lay member, and one a nominee of the Director of the Department of State for Health. A project is deemed approved when it receives the support of at least 4 members of which one is not an employee of MRC. In the event of more than one member having strong objections or reservations the submission may be resubmitted or rejected. Applicants whose project has been rejected have the right to appear before the Committee in person to appeal against this decision. Meetings are held at monthly intervals after a meeting of the MRC Laboratories’ Scientific Co-ordinating Committee. The Director of the MRC Laboratories and the Director of Medical Services
are members of the Committee ex-officio, but have no voting rights on any project considered by the Committee. The Secretariat is provided by MRC Laboratories. 5.2. Description of Laboratory Facilities
The Farafenni Field Station has a laboratory with state-of-the-art equipment for cutting-edge research. The laboratory has rooms, facilities and personnel that are dedicated to work relating to haematology, biochemistry, immunology/molecular biology, entomology and parasitology. Haematological analysis is done using a Medonic Cell Analyser CA530. This is an advanced microprocessor automatic cell counter that performs a complete automatic blood cell analysis designed to measure up to 20 parameters using whole blood or pre-diluted blood. Some of the basic parameters that can be obtained include red blood cell count (RBC), haemoglobin, white blood cell count (WBC) and differential count, platelet count, mean red cell volume (MCV), mean cell haemoglobin concentration (MCHC). ABO blood grouping and cross matching and HIV testing can be done in the haematology area of the laboratory. Clinical Biochemistry analysis is carried out with the use of a Visual (Biomerieux) Analyser that is attached to a results printer. This polychrome analyser is used for all our biochemical and immunochemical analysis. There is a reflotron machine as a backup. The parasitology area is well stocked with compound microscopes for routine malaria microscopy and other parasitological examinations including urine and stool analysis. The station has well- trained microscopists for the diagnosis and speciation of malaria parasites. All the microscopists take part in a malaria slide quality control assessment bimonthly to ensure that our high standards in malaria microscopy are maintained. The pre- and post-PCR rooms are well equipped with PRC machine (Thermal cycler), centrifuge and microwave. The main function of this lab is genotyping of malaria parasites to detect resistant markers for commonly used antimalarial drugs (chloroquine, sulfadoxine/pyrimethamine) There is a culture room equipped with carbon dioxide incubator, a fridge and sterile cabinet. Other essential support equipment include an autoclave for the sterilization of materials used for elispot and other assays, a freezer room with adequate storage facilities including one -70°C freezer and 3 other -40°C freezers for the proper storage of laboratory samples. The freezers are regularly checked by a trained laboratory attendant to ensure that the desired temperatures are maintained. The entomology section of the laboratory is one of the biggest facilities in the station. It has two insectaries where a stable colony of Anopheles gambiae mosquitoes has been established to serve as the source of adult mosquitoes for insecticide resistance experiments and infectivity and transmission studies. A major component of the research portfolio in the Farafenni Field Station has been the search for effective antimalarial drugs and combinations that are able to impede post- treatment transmission and selection of resistant Plasmodium falciparum. This is carried out through membrane feeding experiments in the insectaries. Maintenance of all laboratory and storage equipment is carried out monthly by trained technicians from the MRC Headquarters in Fajara and also by experts from the UK. The field station has its own generators for a regular and consistent electricity supply.
5.3. Description of Clinical Facilities
The Field Station utilises clinical facilities available at the government Maternal and Child Health (MCH) Clinic and the AFPRC General Hospital in Farafenni for the conduct of all clinical studies. This arrangement has been made possible by courtesy of a strong collaboration with the Gambian State Department for Health (DOSH), The Divisional Health Team for North Bank East (DHT NBE) and the Management of the AFPRC General Hospital. The AFPRC General Hospital is a 250-bed hospital with Paediatric, medical, Surgical, Dental and Eye Care Units. It was commissioned in 1998 to provide health care services for the Farafenni township and 63 neighbouring communities. It also serves as the referral centre for the North Bank East Division and neighbouring communities from Central and Lower River Divisions of the Gambia. It has a laboratory with basic facilities for haematological, biochemical and parasitological investigations. There is a blood bank at the hospital laboratory and the field station assists with storage in times of power outages. The field station has been allocated a consulting room at the MCH clinic and the hospital for routine clinical services, screening, enrolment and follow-up of clinical trial and other study participants. MRC clinicians take part in clinical duties at the hospital and MCH clinic in addition to their research activities while the hospital staff participate in the field station’s research projects located at the hospital. There is unlimited access to the hospital’s laboratory and other diagnostic facilities such as X-Ray and ultrasound. The station has therefore made significant contribution to the equipment of the hospital laboratory and the training of staff in the laboratory. For example, staff of the hospital laboratory have received training in malaria microscopy and participate in continuous assessment and quality control checks. During the malaria season in September to December, a laboratory is set up at the MCH clinic for screening of malaria patients. The field station also has access to facilities at health centres in surrounding towns for research work and routine health care delivery to supplement the services of government. The field station is currently collaborating with health centres located in Njaba Kunda, Illiasa, Ngeyen Sanjal and Soma for screening, recruitment and follow-up of study subjects.
5.4. List of Scientists
STAFF NAME QUALIFICATION POSITION
Statistician & Head, MRC Malaria Programme
Clinical Epidemiologist & MRC Scientific Advisor
These core members of staff are complemented by a team of renowned international scientists based at the Headquarters of MRC Laboratories in Fajara. 6. Catalogue of Completed and Ongoing Projects
6.1. Completed Research Projects
Clinical Trials
1. A comparative trial of safety, tolerability and efficacy of sulfadoxine/pyrimethamine combined
with artesunate against acute uncomplicated malaria in Gambian children.
2. A phase I trial of a high dose regimen of malaria candidate vaccines DNA ME-TRAP, FP9 ME-
TRAP and MVA ME-TRAP in adult males in Farafenni.
3. The impact of antimalarial treatment upon the development and persistence of Plasmodium falciparum gametocytes in vivo and in vitro: a randomised trial of chloroquine, sulfadoxine plus pyrimethamine (SP) and CQ plus SP.
4. The impact of antimalarial treatment upon the development and persistence of Plasmodium falciparum gametocytes in vivo and in vitro: a randomised trial of sulfadoxine/pyrimethamine (SP) and artemether plus lumifantrine (CO-artemether).
5. Pharmacokinetic, safety and efficacy of chlorproguanil/dapsone (LAPDAP) in the treatment of
acute uncomplicated Plasmodium falciparum malaria in Gambian children
6. A randomised, controlled, double-blind efficacy trial of DNA/MVA ME-TRAP prime-boost
immunization against malaria infection in Gambian adults
Other Trials 1. Dynamics of gametocyte production of Plasmodium falciparum clones in nature 2. Procurement and use of bednets for malaria control in rural Gambia: A case for community
6.2. Ongoing Research Activities
Clinical Trials
Project 1: Intermittent sulfadoxine-pyrimethamine (SP) to prevent moderate/severe anaemia and low birthweight secondary to malaria in multigravidae: a randomised placebo-controlled trial in The Gambia
Objectives This trial has two components giving us further important information: A. A study to see whether giving SP at clinic visits to multigravidae (women who are pregnant and
have had a pregnancy at least once before of more than 16 weeks duration) reduces anaemia (‘low blood’) in the mothers and low birthweight in the babies
B. A study to see whether giving folate with SP at the first clinic visit to primigravidae (women
who are pregnant for the first time or with a past history of miscarriage and no pregnancy having gone beyond 16 weeks) has a negative effect on the working of SP, compared with starting with the folate 14 days later
Collaboration Collaborators on the trial are the Medical Research Council Laboratories, Divisional Health Team (DHT) North Bank East, AFPRC General Hospital and the Gates Malaria Partnership at the London School of Hygiene & Tropical Medicine.
Funding Malaria Gates Partnership
Population and Period In this randomised placebo-controlled trial the aim is to recruit 3000 multigravidae during the period July 2002 - June 2003 and follow these women through their pregnancy and post-partum period and estimate as the most important endpoints the birthweight and prevalence of post-partum anaemia. We will also determine the cost effectiveness, acceptability and convenience of intermittent SP. For Primigravidae, we intend to recruit 1,000 primigravidae who are all receiving PIT with SP during the period July 2002 until December 2003. The study will be conducted in 8 clinics/PHC circuits in the North Bank East Health Division and 6 in the Lower River Division (see Appendix 1). In each clinic a fieldworker will be posted to work together with the Maternal and Child Health (MCH) teams and gather data at the clinic and during home visits to study participants. Each multigravida participating in the trial who comes to the clinic from 1 July 2002 until 30 June 2003 will receive at each monthly clinic visit (with a maximum of 4) either 3 tablets of SP or 3 tablets of placebo (that look like SP tablets). Each primigravida will receive at the clinic visits SP (again with a maximum of 4 doses), but will be randomised to receive folate and iron with the SP for the first 14 days at the first visit, or only SP and iron. Recruitment of the study in the primigravidae is from 1 July 2002 until 31 December 2003. Significance The World Health Organization is considering recommending treatment at regular intervals (e.g. at each clinic visit with a maximum of 4 treatments) with sulfadoxine-pyrimethamine (SP) or Fansidar® to all pregnant women throughout the year in malarious areas in Africa. This is called ‘preventative intermittent treatment’ or PIT. There is good evidence that giving SP at clinic visits
is an effective strategy to decrease the risk of moderate/severe anaemia and low birth weight in primigravidae, but there are no estimates on the impact in multigravidae. There is also no information on whether intermittent SP should be given throughout the year to pregnant women in areas where there is seasonal malaria such as The Gambia. We are going to research this. It is not known whether folate supplementation will increase the incidence of treatment failure in women receiving SP. Iron and folate tablets are given routinely to pregnant women in The Gambia during clinic visits, to prevent nutritional anaemia. However, folate supplementation may reduce the activity of antifolate antimalarials such as SP. We are testing this hypothesis in a randomised controlled trial that measures the impact of starting folate at the same time as SP, or starting this two weeks later, on parasitaemia in women receiving PIT. Project 2: Randomised controlled trial of amodiaquine plus artesunate, amodiaquine plus sulfadoxine- pyrimethamine and chloroquine plus sulfadoxine-pyrimethamine in Gambian children Objectives 1. To measure P. falciparum transmission seven days after AQ-AS and AQ-SP combination
treatment compared to CQ-SP by comparing gametocyte carriage rates and infectiousness to mosquitoes.
2. Use a multi-site randomised control trial (RCT) to determine and compare the therapeutic
effectiveness of the treatment regimens against uncomplicated P. falciparum malaria in children in rural Gambia by comparing day 14 and 28 parasite clearance rates.
Collaboration The study is being conducted in collaboration with AFPRC General Hospital, Farafenni and the London School of Hygiene & Tropical Medicine. Funding This is an MRC core funded project Population and period The study was conducted during the 2003 malaria season in Farafenni, Brikama, Njaba Kunda and Ngeyen Sanjal. Children aged 0.5-10 years presenting with uncomplicated malaria were randomly allocated AQ-AS, AQ-SP or CQ-SP. In Farafenni, 500 children were enrolled and followed on days 1,2,3, 4, 7, 14 and 28. On day 7, those with gametocytaemia were requested to provide 2.0 ml venous blood for mosquito infectivity experiments. At the other sites, to estimate effectiveness, 1500 treated children were followed on days 14 and 28 only Significance Resistance of P falciparum to chloroquine (CQ) is approaching a critical level in West Africa. Affordable malaria treatment options in areas with CQ resistance include amodiaquine (AQ) and sulfadoxine-pyrimethamine (SP). Combination therapy may protect these drugs against the rapid
development of resistance. Our recent data indicates that drug combinations vary in their ability to impede transmission, a key factor in the spread of drug resistance. Trials have demonstrated the adequate safety and good efficacy of CQ-SP, AQ-SP and AQ-artesunate (AS) combinations in several settings in Africa. However, it is not known which combination will minimize the inevitable risk of selection and transmission of resistance parasites. Furthermore, the effectiveness of these regimens in African outpatient settings has been little studied. We thus propose to evaluate the transmission potential and effectiveness of AQ-AS and AQ-SP combinations compared to CQ- SP for uncomplicated P. falciparum malaria in Gambian children. Project 3: A Phase I trial of the malaria candidate vaccines FP9 CSO, and MVA CSO in adult males aged 18-45 yrs in Farafenni.
Objectives The primary aim is assessment of safety and reactogenicity of these vaccines in Gambian adults. The secondary aim is assessment of immunogenicity and comparison with UK adults. Collaboration University of Oxford, LSHTM Funding Gates Malaria Partnership/ Wellcome Trust Period Covered: Jan – July 2004 Study Population: 32
If safety is acceptable and immunogenicity is good or better than in the UK coupled with evidence of complete protection in the challenge studies in Oxford, then a field efficacy trial in adults could be proposed for Farafenni in the 2004 malaria season.
Other Trials
Project 1:
Community perceptions of a malaria vaccine trial in the North Bank Division of The Gambia.
Objectives To assess:
1. Ideas about vaccines and immunization 2. Understanding of research in general and vaccine trials in particular 3. Previous experiences with vaccination and medical research 4. The consent process and retention of consent information 5. Reasons for participation/refusal/dropout 6. Community understanding of the lack of efficacy of the vaccine
Collaboration: LSHTM Funding Gates Malaria Partnership Period Covered November 03 – April 04 Study Population: 180 Significance Vaccines can only be considered effective if they are culturally acceptable. It is therefore important that, parallel to efforts to develop and test new vaccines, studies are carried out to identify potential obstacles to acceptance and to understand determinants of both passive and active demand for vaccines. 6.3 Projects that have directly influenced National Health Policy
Impregnated bed net study.
7. List of Selected Publications
1. Jawara,M., McBeath,J., Lines,D., Pinder,M., Sanyang,F. & Greenwood,B.M. (1998)
Comparison of bednets treated with alphacypermethrin, permethrin or lambdacyhalothrin against Anopheles gambiae in the Gambia Medical and Veterinary Entomology12, 60-66.
2. Quinones,M.L., Lines,Jo., Thomson,M.C., Jawara,M. & Greenwood,B.M. (1998)
Permethrin-treated bed nets do not have a 'mass-killing effect' on village populations of Anopheles gambiae s.l. in The Gambia Transactions of the Royal Society of Tropical Medicine and Hygiene92, 373-378.
3. Gosling,R., Walraven,G., Manneh,F., Bailey,R. & Lewis,S.M. (2000) Training health
workers to assess anaemia with the WHO haemoglobin colour scale Tropical Medicine and International Health5, 214-221.
4. Ansell,J., Hu,J.-T., Gilbert,S.C., Hamilton,K.A., Hill,A.V.S. & Lindsay,S.W. (2000)
Improved method for distinguishing the human source of mosquito blood meals between close family members Transactions of the Royal Society of Tropical Medicine and Hygiene 94, 572-574.
5. Lindsay,S., Ansell,J., Selman,C., Cox,V., Hamilton,K. & Walraven,G. (2000) Effect of
pregnancy on exposure to malaria mosquitoes The Lancet355, 1972.
6. Quinones,M.L., Drakeley,C.J., Muller,O., Lines,J.D., Haywood,M. & Greenwood,B.M.
(2000) Diversion of Anopheles gambiae from children to other hosts following exposure to permethrin-treated bednets Medical and Veterinary Entomology14, 369-375.
7. De Martin,S., von Seidlein,L., Deen,J.L., Pinder,M. & Walraven,G. (2001) Community
perceptions of a mass administration of an antimalarial drug combination in The Gambia Tropical Medicine and International Health6, 442-448.
8. von Seidlein,L., Jawara,M., Coleman,R., Doherty,T., Walraven,G. & Targett,G. (2001)
gametocytaemia after treatment with chloroquine,
pyrimethamine/sulfadoxine, and pyrimethamine/sulfadoxine combined with artesunate in young Gambians with uncomplicated malaria Tropical Medicine and International Health 6, 92-98.
9. Deen,J.L., von Seidlein,L., Pinder,M., Walraven,G.E.L. & Greenwood,B.M. (2001) The
safety of the combination artensunate and pyrimethamine-sulfadoxine given during pregnancy Transactions of the Royal Society of Tropical Medicine and Hygiene95, 424- 428.
10. Clarke,S.E., Bogh,C., Brown,R.C., Pinder,M., Walraven,G.E.L. & Lindsay,S.W. (2001) Do
untreated bednets protect against malaria? Transactions of the Royal Society of Tropical Medicine and Hygiene95, 457-462.
11. Bogh,C., Clarke,S.E., Pinder,M., Sanyang,F. & Lindsay,S.W. (2001) Effect of passive
zooprophylaxis on malaria transmission in The Gambia Entomological Society of America 38, 822-828.
12. Ansell,J., Hamilton,K.A., Pinder,M., Walraven,G.E.L. & Lindsay,S.W. (2002) Short-range
attractiveness of pregnant women to Anopheles gambiae mosquitoes Transactions of the Royal Society of Tropical Medicine and Hygiene96, 113-116.
13. Deen,J.L., Walraven,G.E.L. & von Seidlein,L. (2002) Increased risk for malaria in
chronically malnourished children under 5 years of age in rural Gambia Journal of Tropical Pediatrics48, 78-83.
14. von Seidlein,L. et al. (2002) Treatment uptake by individuals infected with Plasmodium falciparum in rural Gambia, West Africa Bulletin of the World Health Organization80, 790-796.
15. Clarke,S.E., Bogh,C., Brown,R.C., Walraven,G.E.L., Thomas,C.J. & Lindsay,S.W. (2002)
Risk of malaria attacks in Gambian children is greater away from malaria vector breeding sites Transactions of the Royal Society of Tropical Medicine and Hygiene96, 499-506.
16. Bogh,C., Clarke,S.E., Walraven,G.E.L. & Lindsay,S.W. (2002) Zooprophylaxis, artefact or
reality? A paired-cohort study of the effect of passive zooprophylaxis on malaria in The Gambia Transactions of the Royal Society of Tropical Medicine and Hygiene96, 593-596.
17. Sutherland,C.J. et al. (2003) A transient reduction in treatment failures caused by the
addition of artesunate to chloroquine for treatment of plasmodium falciparum malaria in Gambian children American Journal of Tropical Medicine and Hygiene 1-7.
18. Emerson,P.M. et al. (1999) Effect of fly control on trachoma and diarrhoea The Lancet353,
19. Emerson,P.M., Bailey,R.L., Mahdi,O.S., Walraven,G.E.L. & Lindsay,S.W. (2000)
Transmission ecology of the fly Musca sorbens, a putative vector of trachoma Transactions of the Royal Society of Tropical Medicine and Hygiene94, 28-32.
20. Emerson,P.M., Bailey,R.L., Walraven,G.E.L. & Lindsay,S.W. (2001) Human and other
faeces as breeding media of the trachoma vector Musca sorbensMedical and Veterinary Entomology15, 314-320.
21. Walraven,G. & Weeks,A. (1999) Editorial: The role of (traditional) birth attendants with
midwifery skills in the reduction of maternal mortality Tropical Medicine and International Health4, 527-529.
22. Walraven,G., Telfer,M., Rowley,J. & Ronsmans,C. (2000) Maternal mortality in rural
Gambia: levels, causes and contributing factors Bulletin of the World Health Organization 78, 603-613.
23. Ratcliffe,A.A., Hill,A.G. & Walraven,G. (2000) Separate lives, different interests: male and
female reproduction in The Gambia Bulletin of the World Health Organization78, 570-579.
24. Walraven,G. et al. (2001) The burden of reproductive-organ disease in rural women in The
Gambia, West Africa The Lancet357, 1161-1167.
25. Ratcliffe,A.A., Hill,A.G., Dibba,M. & Walraven,G. (2001) Editorial: The ignored role of
men in fertility awareness and regulation in Africa African Journal of Reproductive Health 13-15.
26. Morison,L. et al. (2001) The long-term reproductive health consequences of female genital
cutting in rural Gambia: a community-based survey Tropical Medicine and International Health6, 643-653.
27. bij de Vaate,A., Coleman,R., Manneh,H. & Walraven,G. (2002) Knowledge, attitudes and
practices of trained traditional birth attendants in The Gambia in the prevention, recognition and management of postpartum haemorrhage Midwifery18, 3-11.
28. Scherf,C., Morison,L., Fiander,A., Ekpo,G. & Walraven,G. (2002) Epidemiology of pelvic
organ prolapse in rural Gambia, West Africa British Journal of Obstetrics and Gynaecology 109, 431-436.
29. Walraven,G., Ekpo,G., Coleman,R., Scherf,C., Morison,L. & Harlow,S.D. (2002)
Menstrual disorders in rural Gambia Studies in Family Planning33, 261-268.
30. West,B., Walraven,G., Morison,L., Brouwers,J. & Bailey,R. (2002) Perfomance of the rapid
plasma reagin and the rapid syphilis screening tests in the diagnosis of syphilis in field conditions in rural Africa Sexually Transmitted Infections78, 282-285.
31. Halton,K. et al. (2003) Herpes simplex 2 risk among women in a polygynous setting in rural
West Africa AIDS17, 1-7.
32. Hill,A.G., MacLeod,W.B., Joof,D., Gomez,P., Ratcliffe,A.A. & Walraven,G. (2000)
Decline of mortality in children in rural Gambia: the influence of village-level Primary Health Care Tropical Medicine and International Health5, 107-118.
33. Bates,C.J., Mathews,N., West,B., Morison,L. & Walraven,G. (2002) Plasma carotenoid and
vitamin E concentrations in women living in a rural West African (Gambian) community Int. J. Vitam. Nutr. Res.72, 133-141.
34. Coleman,R., Loppy,L. & Walraven,G. (2002) The treatment gap and primary health care for
people with epilepsy in rural Gambia Bulletin of the World Health Organization80, 378- 383.
35. Ratcliffe,A.A., Hill,A.G., Harrington,D.P. & Walraven,G. (2002) Reporting of fertility
events by men and women in rural Gambia Demography39, 573-586.
36. Bledsoe,C.H., Hill,A.G., Langerock,P. & D'Alessandro,M. (1994) Constructing natural
fertility: the use of Western contraceptive technologies in rural Gambia Population and Development Review20, 81-113.
37. Bledsoe,C.H., Banja,F. & Hill,A.G. (1998) Reproductive mishaps and Western
contraception: an African challenge to fertility theory Population and Development Review 24, 15-57. References
1. Ahmad,O., Lopez,A. & Inoue,M. (2000) The decline in child mortality: A reappraisal. Bulletin of the World Health Organization78, 1175-1191.
2. Allen,S.J., Otoo,L.N., Cooke,G.A., O'Donnell,A. & Greenwood,B.M. (1990) Sensitivity of Plasmodium falciparum to Chlorproguanil in Gambian children after 5 years of continuous prophylaxis. Transactions of the Royal Society of Tropical Medicine and Hygiene.143, 3043-3048.
3. Bicego,G. & Ahmad,O.B. (1996) Infant and child mortality. Macro International, Calverton, Maryland.
4. Blacker,J.G., Hill,A.G. & Timaeus,I.M. (1985) Age patterns of mortality in Africa: an examination of recent
evidence. In: International Population Conference, Florence International Union for the Scientific Study of Population, Liege, Belgium.
5. Bledsoe,C.H., Hill,A.G., Langerock,P. & D'Alessandro,M. (1994) Constructing natural fertility: the use of
Western contraceptive technologies in rural Gambia Population and Development Review20, 81-113.
6. Bledsoe,C.H., Banja,F. & Hill,A.G. (1998) Reproductive mishaps and Western contraception: an African
challenge to fertility theory Population and Development Review24, 15-57.
7. Central Statistics Department (1998) Population and Housing Census, 1993: Mortality Analysis and Evaluation. Ministry of Finance and Economic Affairs, Banjul, The Gambia.
8. Graham,W., Brass,W. & Snow,R.W. (1989) Estimating maternal mortality: "The sisterhood method". Studies in Family Planning20, 17-25.
9. Greenwood,A.M. et al. (1987) A prospective study of the outcome of pregnancy in a rural area of The
Gambia. Bulletin of the World Health Organization65, 635-643.
10. Greenwood,A.M. et al. (1990) Evaluation of a primary health care programme in The Gambia. I. The impact
of trained traditional birth attendants on the outcome of pregnancy. Journal of Tropical Medicine and Hygiene 93, 58-66.
11. Greenwood,A.M. et al. (1990) Evaluation of a primary health care programme in The Gambia. I. The impact
on mortality and morbidity in young children. Journal of Tropical Medicine and Hygiene93, 87-97.
12. Greenwood,A.M., Menendez,C., Todd,J. & Greenwood,B.M. (1994) The distribution of birth weights in
Gambian women who received malaria chemoprophylaxis during their first pregnancy and in control women. Transactions of the Royal Society of Tropical Medicine and Hygiene.88, 311-312.
13. Greenwood,B.M. et al. (1989) A comparative study of Lapudrine and Maloprim as chemprophylactics against
malaria in Gambian children. Transactions of the Royal Society of Tropical Medicine and Hygiene.83, 182- 188.
14. Hill, A. G, Hill, M. C., Gomez, P., and Walraven, G. Report on the living standards survey conducted in the
villages of the MRC main study areas, North Bank Division, Republic of The Gambia in June-July 1996. 1996. Farafenni, The Gambia, Medical Research Council.
15. Hill,A.G., MacLeod,W.B., Sonko,S.S.T. & Walraven,G. (1998) Improvements in childhood mortality in The
Gambia. The Lancet352, 1909.
16. Hill,A.G., MacLeod,W.B., Joof,D., Gomez,P., Ratcliffe,A.A. & Walraven,G. (2000) Decline of mortality in
children in rural Gambia: the influence of village-level Primary Health Care. Tropical Medicine and International Health5, 107-118.
17. MacLeod, W. B. Description of the Farafenni demographic surveillance system and operation of the
household registration system. 1998. Farafenni, The Gambia, Medical Research Council.
18. Menendez,C., Todd,J., Alonso,P.L., Francis,N. & Greenwood,B.M. (1994) Malaria prophylaxis, infection of
the placenta and birth weight in Gambian primigravidae. Journal of Tropical Medicine and Hygiene97, 244- 248.
19. Menendez,C., Todd,J., Alonso,P.L., Lulat,S., Francis,N. & Greenwood,B.M. (1994) The effects of iron
supplementation during pregnancy given by trtaditional birth attendants on the prevalence of anaemia and malaria. Transactions of the Royal Society of Tropical Medicine and Hygiene.88, 590-593.
20. Menon,A., Otoo,L.N., Herbage,E.A. & Greenwood,B.M. (1990) A national survey of the prevalence of
chloroquine resistant Plasmodium falciparum malaria in The Gambia. Transactions of the Royal Society of Tropical Medicine and Hygiene.84, 638-640.
21. Menon,A., Snow,R.W., Byass,P., Greenwood,B.M., Hayes,R.J. & N'jie,A.B.H. (1990) Sustained protection
against mortality and morbidity from malaria in rural Gambian children by chemoprophylaxis given by village health workers. Transactions of the Royal Society of Tropical Medicine and Hygiene.84, 768-772.
22. Muller,O. et al. (1996) A randomised trial of chloroquine, amadiaquine and pyrimethamine-sulphadoxine in
Gambian children with uncomplicated malaria. Tropical Medicine and International Health1, 124-132.
23. Nyan,O.A. et al. (2001) Atopy, intestinal helminth infection and total serum IgE in rural and urban adult
Gambian communities Clinical and Experimental Allergy31, 1672-1678.
24. Ratcliffe,A.A., Hill,A.G. & Walraven,G. (2000) Separate lives, different interests: male and female
reproduction in The Gambia. Bulletin of the World Health Organization78, 570-579.
25. Republic of The Gambia (1993) Gambian contraceptive prevalence and fertility determinants survey.
Bamako, Mali: CERPOD and The Population Council.
26. Targett,G.A.T. et al. (2001) Artesunate reduces, but does not prevent, post-treatment transmission of
Plasmodium falciparum to Anopheles gambiae. Journal of Infectious Diseases183, 1254-1259.
27. van der Sande,M.A.B. et al. (2000) Blood pressure patterns and cardiovascular risk factors in rural and urban
Gambian communities Journal of Human Hpertension14, 489-496.
28. von Seidlein,L., Jawara,M., Coleman,R., Doherty,T., Walraven,G. & Targett,G.A.T. (2001) Parasitaemia and
gametocytaemia after treatment with chloroquine, pyrimethamine/sulphadoxine, and pyrimethamine/sulphadoxine combined with artesunate in young Gambians with uncomplicated malaria. Tropical Medicine and International Health6, 92-98.
29. Walraven,G., Telfer,M., Rowley,J. & Ronsmans,C. (2000) Maternal mortality in rural Gambia: levels, causes
and contributing factors. Bulletin of the World Health Organization78, 603-613.
30. Walraven,G. et al. (2001) The burden of reproductive-organ disease in rural women in The Gambia, West
Africa The Lancet357, 1161-1167.
1. Statistics will become important StaGen Co. LTD is the company focused on both genetics and statistics. It was established for the purpose of contributing to personalized medicine and pharmacogenomics (or pharmacogenetics) from the aspect of statistical genetics. Pharmacogenomics and personalized medicine are the fields that will become very important in the near future. Since you may not under
Mucosalpreservationiscriticaltosuccessintreatmentofnasalobstructionsecondarytoturbinate hypertrophy. Since hypertrophy is most often secondary to submucosal and non-osseous factors including hypervascularity and submucosal soft tissue excess, BipolarRadiofrequency Turbinate Ablation (RFTA) represents a highly effective, rapid, and well-tolerated techniquethat can be done both i