Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Implantdirect.com
IMPLANT DENTISTRY / VOLUME 20, NUMBER 1 2011
Effect of Sinus Membrane Perforation on Dental Implant Integration: A Retrospective Study on 128 Patients
Eric Oh, DDS,* and Richard A. Kraut, DDS†
Sinusaugmentationasreportedby Acommoncomplicationofsinus patient who had an intact sinus. Allaugmentation is perforation of thefour infections resolved after culturesensitivity and placement of the pa-tion and/or implant placement. Thistient on an appropriate antibiotic forretrospective study examines the ef-fect of sinus membrane perforationwith regard to graft survival and im-the augmented sinuses, five implants
with periosteum and Schneiderian mem-brane, which is a pseudostratified
plant integration. A total of 175 si-failed, four of which were associated
ciliated epithelium that functions by re-
with perforated sinuses and and whichthe membranes being reported intactwas not associated with a perforatedat the time of surgery. A total ofgrafted sinus. (Implant Dent 2011;20:three infections occurred in patientsKey Words: sinus membrane, perfo- ration, osseointegration
membrane has been reported as a com-plication occurring 10% to 60% of the
patients were completely edentulous.
allergic patients). A full thickness buc-
PATIENTS AND METHODS Patients
*Chief Resident, Division of Oral and Maxillofacial Surgery,Montefiore Medical Center, Bronx, NY.
†Chairman, Department of Dentistry, Director of Oral andMaxillofacial Surgery Residency Program, Montefiore Medical
Reprint requests and correspondence to: Richard A. Kraut, DDS, Montefiore Medical Center, 111 East 210th Street, Bronx, NY 10467, Phone: (718) 920-5993, Fax: (718) 515-5419, E-mail: [email protected]
MA) was used to repair large perfora-tions. Implant Direct or Nobel BioCare
Copyright 2011 by Lippincott Williams & Wilkins
SINUS MEMBRANE PERFORATION EFFECT ON DENTAL IMPLANT INTEGRATION • OH AND KRAUT
the flap closed primarily with 3-OChromic gut and 3-O Vicryl sutures.
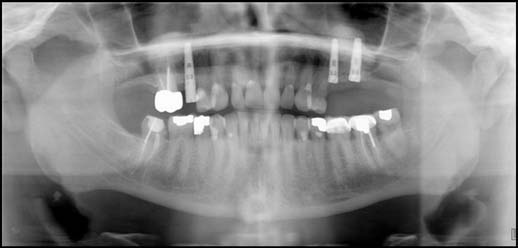
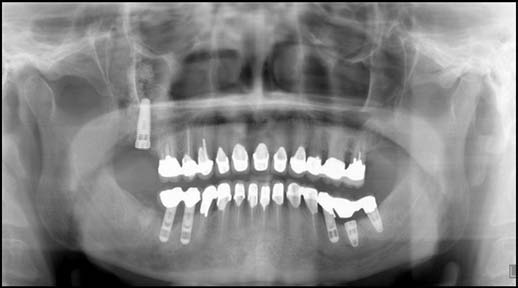
tients received sinus augmentation anddental implants in 2007. There was atotal of 175 sinus augmentations: 47were bilateral (Figs. 1 and 2) and 81were unilateral (Figs. 3 and 4). Thesurgeon noted 115 intact sinuses and
Fig. 1. Panoramic of intact bilateral sinus membrane.
60 (34%) perforated sinuses (Figs. 5– 8) during the surgeries. There werefour (2.2%) sinus infections (Table 1). Three infections occurred in patientswho had sustained a perforated sinusand one in a patient who had an intactsinus. All four infections resolvedafter culture and sensitivity and place-ment of the patient on Avelox (moxi-floxacin
Wayne, NJ), 400 mg daily for 10 daysplus Flonase (fluticasone propionate)(Glaxo Smith Kline, Triangle Park,NC), two sprays in each nostril daily
Fig. 2. Panoramic of intact bilateral sinus membrane.
plants placed in the bone-augmented si-nus. Three hundred four implants wereplaced in intact sinuses, and 134 im-plants were placed in perforated sinuses. A total of five implants failed: four im-plants from perforated sinus and oneimplant from an intact sinus. These dataresult in a 99% success rate of implantintegration in intact sinuses comparedwith 97% success rate in perforated si-nuses (Table 2).
were Noble Biocare Replace Selectand 190 were Implant Direct. Noble
Fig. 3. Panoramic of intact left sinus membrane.
Biocare had two (1%) failures com-pared with three (2%) failures for Im-plant Direct (Table 3).
were compared. There were 47 im-plants placed in augmented sinuses, 36implants placed in intact sinuses, and11 implants placed in perforated si-nuses. Nineteen implants were Im-plant Direct and 28 implants wereNobel Biocare. One implant (NobelBiocare) failed from an intact sinus(Table 4). DISCUSSION Fig. 4. Panoramic of intact right sinus membrane.
IMPLANT DENTISTRY / VOLUME 20, NUMBER 1 2011
mentation, including perforation ofsinus membrane, acute or chronic si-nusitis, cyst, mucocele, delayedwound healing, hematoma, and loss/sequestrum of bone. The most fre-quently occurring complication is per-foration of the sinus membrane, whichis reported in from 10% to 60% ofcases.4–7 Perforation of the sinus mem-brane by itself may cause further com-plications such as increased risk ofinfection due to communication withother sinuses or risk of migration of
Fig. 5. Panoramic of right perforated sinus membrane.
graft particles into the sinus wherethey induce polyps or other sinus dis-eases.12,13 Some studies report aban-doning sinus lifting procedure becauseof the wide perforation8,14–18 However,Schneiderian membrane perforation isnot an absolute indication for aban-doning the procedure unless the mem-brane is largely destroyed.12,19
ing perforation of the Schneiderianmembrane. The most common methodis the placement of resorbable mem-brane under the perforated Schneide-
Fig. 6. Panoramic of left perforated sinus membrane.
rian membrane.13,19,20,21 Other methodsfor treating perforation include foldingthe membrane up against itself,22 usingsutures,12 or using fibrin glue10,23 toclose the perforation. At our institu-tion, we routinely use Surgicel tocover small to moderate size perfora-tions. Surgicel is an absorbable hemo-static agent made of an oxidizedcellulose polymer, and it is usuallyused to control bleeding. Previous re-ports indicate that using Surgicel istechnically simple, fast, reliable, andeconomical. It shows limited bacteri-cidal qualities, and has no contraindi-
Fig. 7. Panoramic of right perforated and left intact sinus membrane.
chance of Schneiderian membraneperforation include anatomical varia-tions, surgeon’s experience, and pre-vious sinus infection or surgery. Anatomical factors consist of thick-ness of the lateral maxillary sinuswall, convex lateral sinus wall, con-nection between Schneiderian mem-brane and oral mucosa, narrow andwide sinus, maxillary sinus septa, lon-gitudinal septum, and root-shape con-figuration.3,9–11 It is also suggested that
Fig. 8. Panoramic of right perforated sinus membrane.
previous sinus surgery and absence ofalveolar bone are risk factors for a
SINUS MEMBRANE PERFORATION EFFECT ON DENTAL IMPLANT INTEGRATION • OH AND KRAUT
materials. Int J Oral Maxillofac Implants. Table 1. Infection Rate on Condition of Sinus Membrane
simultaneous implantation: A 6-year clini-cal investigation. Int J Oral Maxillofac Im-plants. 1999;14:557-564. Table 2. Implant Success Rate on Condition of Sinus Membrane
conference of 1996. Int J Oral MaxillofacTable 3. Implant Success Rate on Implant Brand
placement of hydroxylapatite-coated im-plants. J Oral Maxillofac Surg. 1989;47:
the maxillary sinus with intraorally har-vested autogenous bone prior to implant
Table 4. Immediate Loaded Implant Success Rate on Condition of
placement. Int J Oral Maxillofac Implants.
al. Augmentation of the maxillary sinus floor
with particulated mandible: A histologic andhistomorphometric study. Int J Oral Maxillo-fac Implants. 1996;11:760-766.
of maxillary sinus floor augmentation: A ra-
diographic assessment. Int J Oral Maxillo-
floor augmentation at the time of maxillary
fac Implants. 2004;19:559-562.
molar extraction: Success and failure rates
repair: Report of a technique for large per-
years. J Periodontol. 2002;73:39-44.
forations. Implant Dent. 1999;8:29-34.
6. Proussaefs P, Lozada J, Kim J, et al.
BS. Histologic and clinical observations of
CONCLUSION
human study. Int J Oral Maxillofac Im-
containment. Int J Oral Maxillofac Im-
et al. The clinical significance of sinus
fects of sealing the perforated sinus mem-
tion of the maxillary sinus. J Oral Maxillofac
membrane: A pilot study in humans. J Oral
Effects of sinus membrane perforations on
omy, physiology, surgery, and bone graft-
ing related to implantology—Eleven years
Disclosure
the augmented sinus. J Periodontol. 2006;
of surgical experience (1979–1990). J Oral
23. Choi BH, Zhu SJ, Jung JH, et al.
the products mentioned in this article.
et al. Chronic sinusitis complicating sinus
The use of autologous fibrin glue for clos-
lift surgery. Am J Rhinol. 2001;15:181-
ing sinus membrane perforations during si-
nus lifts. Oral Surg Oral Med Oral PatholEFERENCES Oral Radiol Endod. 2006;101:150-154.
maxillary sinus floor with autogenous mar-
pects of sinus floor elevation. Clin Oral Impl
JL, et al. Sinus lift grafts and endosseous
row and bone. J Oral Surg. 1980;38:613-
implants. Dent Clin North Am. 1992;36:
sification system for sinus membrane per-
reconstructions. Dent Clin North Am.
with options for repair. J Periodontol.
assessment of a sinus lift operation using
reoxidised cellulose (Surgicel) as graft ma-
Schulten E, et al. Anatomical and surgical
terial. Clin Oral Implants Res. 2001;12:
findings and complications in 100 consec-
utive maxillary sinus floor elevation proce-
large sinus membrane tears. J Oral Maxil-
dures. J Oral Maxillofac Surg. 2008;66:
lofac Surg. 2009;67:1937-1940.
The use of oxidized regenerated cellulose
4. Shlomi B, Horowitz I, Kahn A, et al.
brane tears during the sinus lift procedure. West Indian Med J. 2005;54:398-399.
Hildegard Teuschl Intensivseminaren, sowie die Arbeit in anwendungsorientierten Kontexten , d.h. über (fächerübergreifende) Probleme mit starkem Realitätsbezug. Als ich sie vor Weihnachten zuletzt besuchte, Studierenden bei der Abfassung ihrer Di-war sie müde, aber nicht mutlos. Seit über plomarbeiten und Dissertationen ein. Als einem Jahr hatte sie unheilbaren Krebs. Die Kriterium
Help for your patients who suffer from specific Unlike other anxiety disorders, specific phobias Specific phobias are the most prevalent and primordial of anx- iety disorders. Long lists of phobias with myriad Greek rootsare often cited in consumer press articles on anxiety, but generally do not respond these terms are of little use to clinicians. The research and clinical literat

 IMPLANT DENTISTRY / VOLUME 20, NUMBER 1 2011
Effect of Sinus Membrane Perforation on
IMPLANT DENTISTRY / VOLUME 20, NUMBER 1 2011
Effect of Sinus Membrane Perforation on


 SINUS MEMBRANE PERFORATION EFFECT ON DENTAL IMPLANT INTEGRATION • OH AND KRAUT
the flap closed primarily with 3-OChromic gut and 3-O Vicryl sutures.
SINUS MEMBRANE PERFORATION EFFECT ON DENTAL IMPLANT INTEGRATION • OH AND KRAUT
the flap closed primarily with 3-OChromic gut and 3-O Vicryl sutures.


 IMPLANT DENTISTRY / VOLUME 20, NUMBER 1 2011
mentation, including perforation ofsinus membrane, acute or chronic si-nusitis, cyst, mucocele, delayedwound healing, hematoma, and loss/sequestrum of bone. The most fre-quently occurring complication is per-foration of the sinus membrane, whichis reported in from 10% to 60% ofcases.4–7 Perforation of the sinus mem-brane by itself may cause further com-plications such as increased risk ofinfection due to communication withother sinuses or risk of migration of
Fig. 5. Panoramic of right perforated sinus membrane.
IMPLANT DENTISTRY / VOLUME 20, NUMBER 1 2011
mentation, including perforation ofsinus membrane, acute or chronic si-nusitis, cyst, mucocele, delayedwound healing, hematoma, and loss/sequestrum of bone. The most fre-quently occurring complication is per-foration of the sinus membrane, whichis reported in from 10% to 60% ofcases.4–7 Perforation of the sinus mem-brane by itself may cause further com-plications such as increased risk ofinfection due to communication withother sinuses or risk of migration of
Fig. 5. Panoramic of right perforated sinus membrane. SINUS MEMBRANE PERFORATION EFFECT ON DENTAL IMPLANT INTEGRATION • OH AND KRAUT
materials. Int J Oral Maxillofac Implants.
SINUS MEMBRANE PERFORATION EFFECT ON DENTAL IMPLANT INTEGRATION • OH AND KRAUT
materials. Int J Oral Maxillofac Implants.