Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Clinical scenario series on
Group on Immunization Education Society of Teachers of Family Medicine CLINICAL SCENARIO SERIES ON IMMUNIZATION Shingles and Post Herpetic Neuralgia Written by: Donald B. Middleton, MD Department of Family Medicine University of Pittsburgh Revision of this clinical scenario was funded from an unrestricted educational grant from the Pennsylvania Academy of Family Physicians. This scenario was initially funded by an unrestricted educational grant from Merck & Co., Inc. to the Society of Teachers of Family Medicine Foundation. Copyright 2010 Society of Teachers of Family Medicine Permission to use, copy and distribute this clinical scenario is hereby granted for private, non-commercial and educational purposes only, provided that the above copyright notice appears with the disclaimer and following notice: this document may be reprinted and distributed for non-commercial and educational purposes only, and not for resale. No resale use may be made of this material at any time. All other rights reserved. Disclaimer: Use at your own risk! Every effort has been made to ensure accuracy. However, no liability or warranty for error of omissions exists, expressed or implied. This information is provided by the Society of Teachers of Family Medicine (STFM) Group on Immunization Education only as assistance for physicians making clinical decisions regarding care of their patients. As such, this information cannot substitute for the individual judgment brought to each clinical situation by the patient’s physician. As with all clinical reference resources, they reflect the best understanding of the science of medicine at the time of publication, but they should be used with the clear understanding that continued research may result in new knowledge and recommendations.
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
Learning Objectives
1. Learn the natural history of herpes zoster virus. 2. Recite the clinical course of an attack of herpes zoster (shingles). 3. Recognize the severe consequences an attack of herpes zoster (shingles) for
4. Incorporate herpes zoster (shingles) vaccine into clinical practice as an
effective health preventive measurement for an older adult.
Scenario Visit 1 After shoveling snow 2 days ago, Ramon, a 66 year-old married financial consultant, presents with severe, right sided, burning pain (8 out of 10) radiating from his back around his chest to his upper abdomen. The pain is relentless, unresponsive to ibuprofen, 600 mg, TID, and local heat; is constantly distracting; and interferes with simple tasks like dressing or sleeping. He is unable to work. Past health issues include osteoarthritis involving the thoracic and lumbar disks responsive to physical therapy and ibuprofen, prn. He also has diet- and metformin (1000 mg, BID)-controlled diabetes mellitus (his last A1c = 6.8%); hypertension controlled with HCTZ, 25 mg, daily; and hypercholesterolemia (his last LDL = 98, HDL = 41) controlled with simvastatin, 40 mg, daily. He neither drinks to excess nor smokes, and he exercises twice a week. He gets annual influenza vaccination but has never pneumococcal polysaccharide vaccine (PPVS23). His last tetanus shot was at age 50 years. He has two children and three grandchildren. His father died at age 58 from a heart attack. His mother is 87 and has osteoarthritis but is still fit. His wife, Louisa, age 61 years, is concerned about whether his pain could be from his heart or his back arthritis. His physical examination is unremarkable except for severe pain of the right back at rest, intensified with movement, touch, and palpation of the right back at the level of T9. Cardiac and pulmonary evaluations are normal except for a BP of 144/88, but he seems to be in intense pain. The EKG is normal.
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
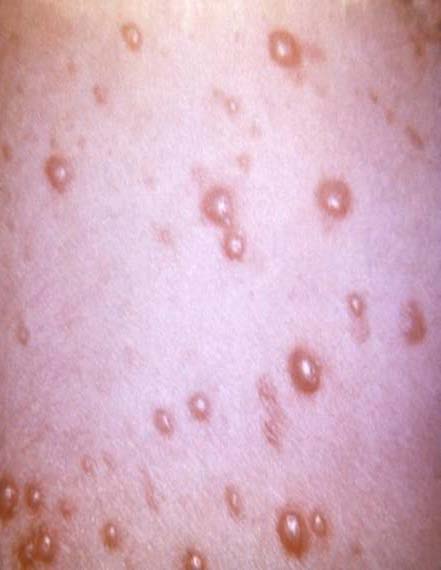
Treatment given is acetaminophen, 1000 mg, QID and oxycodone, 15 mg, QID, prn given especially for sleep. Ramon is instructed to return immediately if he develops worsening symptoms such as shortness of breath or a rash. Visit 2 The next day, Ramon returns with a rash around his right midback to his flank. The vesicular rash seemed to develop quickly over the past 24 hours. The pain persists (8 to 9 of 10) with only moderate relief from the oxycodone/acetaminophen. It interferes with almost all of his daily routine including work. Two weeks ago Ramon and Louisa had visited their 15 month-old granddaughter, Concha, in Mexico. Concha developed chickenpox while they were visiting. Ramon states that he never had chickenpox, but Louisa is concerned that Ramon has shingles. She wants to treat his severe discomfort as well as keep herself safe and shingles free. On examination he has over 200 two to four mm vesicles on red bases scattered from his back around to his upper abdomen. Any touch is intolerable.
Zoster in a Thoracic Dermatome Shingles vesicles
Source: Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
Questions 1. How is this illness linked to chickenpox?
2. What medication(s) is (are) indicated? How could this problem have
3. What can be done to help protect Louisa and other family members? Will she
4. What complications can occur following an attack of herpes zoster (shingles)? 5. What vaccines are indicated for Ramon, Louisa, and other family members? 6. Is the vaccine to prevent shingles safe?
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
Answers 1. Almost every adult world wide has had chickenpox even though the individual
is unable to recall the illness. After chickenpox clears, herpes zoster, the causative DNA virus, survives lifelong in a latent state in the dorsal root ganglia of the spinal cord. Each dorsal root ganglion innervates a particular dermatome on one side of the body. The dermatome with the most pox lesions during acute chickenpox is most likely to develop an outbreak of shingles in later life.
Disease Risk Years later with waning cellular immunity due to aging or immune system challenge like chemotherapy, herpes zoster resurfaces as shingles. Because most adults have had chickenpox, whether they remember it or not, more than 90% of the population is at risk for developing shingles, . Those over age 60 years are at particular risk. After age 85 years, the risk of developing shingles is over 50%. An estimated 1,000,000 cases occur annually in the United States. Only one (or rarely two adjacent) unilateral dermatome is effected during an episode of shingles. The pain from shingles is variable in onset and lasts usually 2 to 4 weeks, resolving as the vesicles scab over and clear. The rash develops 1 to 5 days after the onset of pain and does not cross the midline. Acute shingles pain, often described as lancinating or burning, can be debilitating. Older individuals generally have more severe pain indicative of a higher risk of chronic nerve damage. Those with intense prodromal pain or large numbers of vesicles are more likely to suffer complications, particularly post-herpetic neuralgia (PHN) (see below). Immunogenicity Cellular immunity provides the major protective response to herpes zoster. A marker of immune response, serum antibody levels reflect but do not exactly correlate with the ability to control zoster. Herpes zoster vaccine boosts both cellular immunity which serves to keep zoster in the latent state and antibody levels. Because individuals who recover from acute shingles must have activated their own immune systems in order to have recovered, they are unlikely to benefit from zoster vaccination at least in the immediate years following recovery from the acute infection. The virus is not cleared from the body but simply becomes latent again so some persons can develop shingles again in the future. In the 8 year period following a bout of zoster, the risk of
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
developing recurrent zoster is approximately 6%. Routine childhood immunization against herpes zoster has resulted in many fewer cases of natural chickenpox, and as a consequence most adults will no longer boost their own immune systems from recurrent exposure to ill children. Without this natural boosting, shingles outbreaks may shift to the younger adult population and/or the risk of recurrent disease may increase. The influence of reduced varicella prevalence on zoster epidemiology is uncertain. Whether exposure to chickenpox can trigger shingles is unclear but unlikely. Most cases of shingles occur sporadically. Exposure to shingles can certainly lead to chickenpox in a non-immune individual, particularly if that individual touches the shingles rash. Chickenpox can be severe in adults and is often complicated by pneumonia. Airborne transmission of herpes zoster from a shingles attack is extremely unlikely to occur despite evidence that scratching a zoster rash can aerosolize DNA from Herpes zoster virus.
Sidebar The diagnosis of shingles is sometimes difficult because pain can mimic many other conditions. Ramon’s initial differential diagnoses included radiculopathy, diabetic neuropathy, myalgia from shoveling, and myocardial pain.
2. Treatment includes antiviral therapy (acyclovir, famciclovir, valacyclovir)
which must be given in high doses within 72 hours of pain onset to reduce acute pain and reduce the incidence of PHN. Ramon was given acyclovir, the least expensive agent, 800 mg, 5 times a day, for 10 days. Compliance with the five doses a day may be an issue.Valacyclovir is given 1 gm, TID, and famciclovir 500 mg, TID, each for 7 days.
As an adjunct prednisone speeds healing but does not prevent complications. In this case, the diabetes mellitus and hypertension might forestall the prescription of prednisone, which is usually given at a dose of 60 mg per day for 1 week then tapered off over an additional 2 weeks.
Potent pain control medication using narcotics as tolerated remains an important component of treatment. Other treatments include aluminum acetate soaks, topical lidocaine patches, antiseizure medications (gabapentin, pregabalin), NSAIDs in various doses, and topical capsaicin. When tolerated, tricyclic antidepressants such as desipramine 100 mg, daily, appear to give the best chance of cost-effective pain relief. Costs associated with a case of shingles are significant.
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
Elderly patients who develop shingles are often on multiple medications that may interact with drugs used for pain control. Care should be taken to avoid side effects such as prolonged INRs for persons on warfarin. Drugs that reduce pain may also affect balance or cognition so must be adjusted to reduce accidents and other serious side effects.
Vaccine (Zostavax®) The risk for shingles could have been lessened had Ramon received herpes zoster vaccine (Zostavax®). This live virus vaccine contains 19,400 CFU of Oka/Merck virus, the same virus used in the chickenpox vaccine (Varivax®). Zostavax® is indicated as a one time subcutaneous immunization for persons age 60 years and older (no upper age limits). It reduces the incidence of shingles by 51to 55% overall, reduces the severity of shingles, particularly herpes ophthalmicus, in those who do develop this problem, and reduces the incidence of post-herpetic neuralgia (PHN) by 67% overall and by 39% in those who do still develop shingles despite vaccination. These statistics are remarkable for a vaccine that is not simply preventing acquisition of a new infection but rather a reemergence of an infectious agent already in the body. Although the duration of immunity is unknown, the vaccine protects for longer than 4 years. A 2011 publication compared the incidence of zoster in 75,761 vaccinees to that in 227,283 nonvaccinees. Following vaccination, the incidence of zoster was reduced 55% and included a 63% reduction in herpes ophthalmicus and 65% reduction in hospitalizations. Zostavax® is frozen and must be given within 30 minutes of reconstitution. A single dose is 0.65 ml. For Medicare it is covered under Part D (pharmacy benefits). Barriers to its use include issues of vaccine storage, timing of administration, cost ($162/dose), and reimbursement issues. Contraindications are immunocompromise, pregnancy, untreated active tuberculosis, and a history of anaphylactic/anaphylactoid reaction to any vaccine component including gelatin and neomycin (NOT including dermal reaction). Rapid anamnestic antibody response is expected following vaccination. Because almost everyone has had chickenpox, pre-vaccination testing for herpes zoster antibodies is not indicated. Persons are unlikely to have severe reactions to a vaccine virus that so closely mimics the natural virus already harbored in the body. Inquiry about a history of prior zoster illness is not necessary before vaccination.
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
3. Louisa and her mother-in-law should be vaccinated against
herpes zoster immediately although their risk of contracting shingles from Ramon is minimal, especially if they avoid direct contact with the vesicular lesions. Generally patients with zoster do not produce air-borne viral particles that are capable of infecting others. The benefit of vaccination for Ramon is unclear. Only 6% of the population with shingles have recurrences, but as individuals survive to older age, as the number of serious immune system-challenging diseases like diabetes or cancer increase, and as the agents used to fight these disease like anti-tumor necrosis factor medications become more widely prescribed, that risk may increase. Further study should clarify the benefits of vaccination at some future date for those who have already recovered from a case of shingles. Waiting at least 2 years before vaccination is a sensible approach to this frequent question. All of the uninfected grandchildren should receive 2 doses of chickenpox vaccine (Varivax®) at the recommended ages of 12 months and 4 to 6 years. The second dose may be given at an earlier age but should be at least 3 months after the first dose. If the chickenpox was confirmed by a health care professional, Concha should not receive Varivax®.
4. Complications of shingles are listed below. Complications of Shingles Neurologic
Allodynia: pain following generally nonpainful stimuli like clothes touching
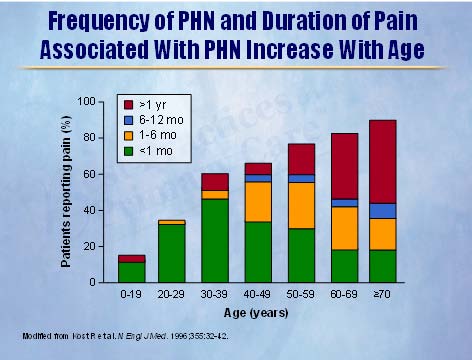
Post-herpetic neuralgic (PHN): increased incidence with advanced age,
with a large number of shingles vesicles, or with prolonged, severe prodromal pain (before the rash)
Motor nerve palsy: often facial nerve VII; eyelid ptosis; Ramsay Hunt
syndrome, involving the external ear canal
Encephalitis: rare Transverse myelitis: uncommon; intense, excruciating back pain and distal
Sensory neuropathy: common; reduced touch and pain sensation in the
affected dermatome or those adjacent to it
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
Cutaneous: extremely common Bacterial superinfection: 2% Scarring: 8% Depigmentation: common
Stromal keratitis Iritis Retinitis Visual impairment Episcleritis Keratopathy
Visceral: unusual but any internal organ may be affected
Psychiatric: common, especially with PHN
Polypharmacy to control pain with resultant multiple drug side effects and expense.
Post-Herpetic Neuralgia (PHN)
PHN has variable definition. The most common is pain that is >3 of 10 lasting for >90 days. Clearly pain that is >3 of 10 or that limits activities for shorter periods of time still requires medical attention and may reflect nerve damage. Elderly patients often have PHN that lasts 1 to 2 years and some patients never fully recover, developing chronic dysesthesias or parethesias. The annual incidence in patients over 80 years of age is roughly 10 per 1000. Older individuals have more severe, longer lasting pain, requiring multiple medications that may cause side effects or interact with other medications given for other acute or chronic diseases. PHN can be treated with antidepressants (especially the tricyclics desipramine and nortriptyline), analgesics, topical capsaicin, topical lidocaine, anticonvulsants (gabapentin, pregabalin), intrathecal corticosteroids, NMDA receptor antagonists (dextromethorphan), cryotherapy, and/or surgery. New investigational medications that inhibit mediators of pain offer some promise of improved pain
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
control. Preventive measures include Zostavax® for all persons age 60 years and above. Kost, Strauss. N Eng J Med.1996;355:32-42. Copyright 1996 Massachusetts Medical Society, used with permission. 5. Despite being in the age group of >65 years, Ramon should receive a Tdap
vaccination as should Louisa (being under age 65 years) to include protection against pertussis. 2010 data indicate both immunogenicity and safety in all persons over the age of 6 years. Adults over age 64 years who are exposed to infants under age 6 months should receive a single dose of Tdap. Adults over age 64 years may be vaccinated with Tdap if they wish to reduce their risk of obtaining pertussis or reduce transmission to other family members, especially young children. Tdap vaccine may be given at any interval following a Td vaccine.
Both should receive annual influenza vaccine.
Lacking any specific indication, Louisa should receive a PPVS23 Pneumovax®) at age 65 years. For multiple reasons including his age and diabetes mellitus, Ramone should receive a PPVS23 now. According to the
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
manufacturer, PPVS23 and herpes zoster vaccine should NOT be given concurrently because PPVS23 reduces antibody response to the shingles vaccine. These two vaccines should ideally be separated by 4 weeks. The Centers for Disease Control and Prevention does not espouse this separation and advises concurrent vaccinating to optimize vaccination rates.
6. Zoster vaccine is extremely safe. Side effects are mainly local irritation in 48%
of vaccinees compared to 16% of those given placebo and are more common in younger vaccinees. Serious adverse events in vaccinees (1.4%) match those following placebo (1.4%). Localized rash may due to the vaccine virus; systemic rash is rare and no more common in vaccinees. Shingles rash occurring within 42 days of vaccination is universally due to wild varicella, not vaccine virus. Post-vaccination viral transmission is not known to occur.
Denouement Luckily, Ramon was treated early in the course of his illness so may escape the consequence of PHN even though his vesicle count is high.
Society of Teachers of Family Medicine, Group on Immunization Education
Clinical Scenario – Shingles and Post-Herpetic Neuralgia
References 1. Mounsey AL, Matthews LG, and Slawson DC. Herpes zoster and postherpetic
neuralgia: prevention and management. AFP 2005; 72:1075-1080.
2. Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster
and postherpetic neuralgia in older adults. NEJM 2005; 352:2271-2284.
3. Insinga RP, Itzler RF, Pellissier JM, Saddler P, and Nikas AA. The incidence
of herpes zoster in a United States administrative database. J Gen Intern Med 2005; 20:748-753.
4. Simberkoff MS, Arbeit RD, Johnson GR, et al. Safety of herpes zoster
vaccine in the shingles prevention study. Ann Inter Med 2010; 152:545-554.
5. Cordeiro de Santos M, Alecrim MGC. Varicella pneumonia in an adult. NEJM
6. Dworkin RH, White R, O’Connor AB, et al. Healthcare costs of acute and
chronic pain associated with a diagnosis of herpes zoster. JAGS 2007; 55:1168-1175.
7. Hurley LP, Lindley MC, Harpaz R, et al. Barriers to the use of herpes zoster
vaccine. Ann Intern Med 2010; 152:555-560.
8. Sanford M, Keating GM. Zoster vaccine (Zostavax®). A review of its use in
preventing herpes zoster and postherpetic neuralgia in older adults. Drugs Aging 2010; 27:159-176.
9. Donahue JG, Kieke BA, Gargiullo PM, et al. Herpes zoster and exposure to
the varicella zoster virus in an era of varicella vaccination. Am J Public Health 2010; e1-e7.
10. O’Connor AB, Noyes K, Holloway RG. A cost-effectiveness comparison of
desipramine, gabapentin, and pregabalin for treating postherpetic neuralgia. JAGS 2007; 55:1176-1184.
11. CDC. Prevention of herpes zoster. MMWR 2008; 57 (05): 1-30. 12. Tseng HF, Smith N, Harpaz R, et al. Herpes zoster vaccine in older adults
and the risk of subsequent herpes zoster disease. JAMA 2011; 305: 160-166.
13. Yawn BP, Wollan PC, Kurland MJ, et al. Herpes zoster recurrences more
frequent than previously reported. Mayo Clin Proc 2011; Jan 10 epub.
14. CDC. Updated recommendations for use of tetanus toxoid, reduced
diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR 2011; 60: 13-15.
Society of Teachers of Family Medicine, Group on Immunization Education
Adhesion prevention in gynecologic surgeryTogas Tulandi and Abdulaziz Al-ShahraniThe purpose of this review is to discuss new substancesOne of the complications of abdominal surgery is intra-and techniques to prevent post-surgical adhesionabdominal adhesion formation. These adhesions cancause bowel obstruction and pain, whereas adnexaladhesions can cause infertility In an attempt toIntraper
MODELO DE BULA PARA OS PROFISSIONAIS DE SAÚDE I) IDENTIFICAÇÃO DO MEDICAMENTO: Revectina® ivermectina APRESENTAÇÕES Comprimidos (6 mg): cartuchos com 2 e 4 comprimidos VIA ORAL USO ADULTO E PEDIÁTRICO (crianças acima de 5 anos de idade ou com mais de 15 kg) COMPOSIÇÃO Cada comprimido de REVECTINA® (ivermectina) contém: ivermectina.6 mg Excipientes: ce