Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Pii: s1470-0328(02)02325-x
BJOG: an International Journal of Obstetrics and GynaecologyFebruary 2003, Vol. 110, pp. 112 – 120
Effect of timing and type of treatment on the risk of mother
to child transmission of Toxoplasma gondii
European Multicentre Study on Congenital Toxoplasmosis*
Objective To determine the effects on mother to child transmission of the timing and type of prenatal
treatment, taking into account gestational age at maternal seroconversion.
Setting European centres offering prenatal screening for toxoplasmosis.
Population Children born to a cohort of pregnant women with toxoplasma infection.
Methods We determined the effects on mother to child transmission of the interval between seroconversion
and start of treatment (treatment delay), and the type of treatment, taking into account gestational age atmaternal seroconversion.
Main outcome measure Congenital infection status confirmed by toxoplasma IgG results at one year
Results Of 1208 women analysed, 72% were first prescribed spiramycin, 19% pyrimethamine – sulphonamide
and 9% (mostly infected during the last trimester) were untreated. The odds ratios for mother to childtransmission for all women treated after a delay of four to seven weeks was 0.77 (95% CI 0.34 – 1.69), andafter eight weeks or more was 1.33 (0.56 – 2.89) compared with less than four weeks. The odds ratio perweek of treatment delay was 1.01 (0.93 – 1.08). There was no evidence that transmission risk differed inwomen first treated with pyrimethamine – sulphonamide versus spiramycin: odds ratio 1.10 (0.63 – 1.91) orin untreated versus treated women: odds ratio 0.57 (0.27 – 1.17).
Conclusion We were unable to demonstrate a beneficial effect of the timing or type of prenatal treatment on
the risk of mother to child transmission but we could not exclude a clinically important effect. Randomisedcontrolled trials are required to determine the effect of prenatal treatment on mother to child transmission.
bias, for example, in the children lost to follow up, or dueto inclusion of women tested because of suspected fetal
Prenatal testing for toxoplasma infection aims to identify
abnormalities, may have distorted the results.
women who acquired infection for the first time during
We prospectively studied a cohort of women and their
pregnancy and are at risk of transmitting infection to their
children in 11 European centres. Serological testing to
fetus. Infected women are treated in order to prevent mother
identify infection acquired during pregnancy varied from
to child transmission of infection and, if fetal infection has
three monthly in Vienna to monthly in France. Compliance
occurred, to reduce the risk of intracranial and ocular
with testing was variable and the type of treatment differed
damage. Although prenatal screening has operated for
between centres. Few women received no treatment. Such
30 years in some countries, no controlled trials have been
variation made it possible to investigate the effect of timing
conducted to evaluate prenatal treatment1. However, three
and type of treatment on mother to child transmission of
recent studies, based on cohorts of treated and untreated
women, have determined the effect of prenatal treatment onmother to child transmission after taking into account thestrong effect of gestational age at maternal infection on
transmission risk2 – 4. None of these studies reported asignificant effect of treatment on mother to child transmis-
There were 11 study centres (Table 1); 10 routinely
sion but none could exclude effects which might justify
offered prenatal screening and provided a reference service
treatment. As these studies were retrospective, selection
for toxoplasmosis in pregnancy. In Stockholm, womenwere identified as part of a research study5.
Infected women were prospectively enrolled between
January 1996 and March 2000. Clinical and microbiolog-
* Correspondence: Dr R. Gilbert, Centre for Paediatric Epidemiology
ical data were collected using standard proformas at the end
and Biostatistics, Institute of Child Health, 30 Guilford Street, LondonWC1N 1EH, UK.
of pregnancy and for infants at 1, 6 and 12 months of age.
D RCOG 2003 BJOG: an International Journal of Obstetrics and GynaecologyPII: S 1 4 7 0 - 0 3 2 8 ( 0 2 ) 0 2 3 2 5 - X
PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
Table 1. Prenatal testing and treatment protocols. PN ¼ postnatal testing of seronegative women; RT ¼ rising IgG titre; Avidity ¼ low IgG avidity; HT¼high IgG titre. All enrollments were consistent with the definite and probable criteria reported by Lebech et al.15.
a Routine postnatal testing of cord blood and/or postnatal sample in seronegative women. b Daily dose in all centres ¼ 3 g/day until delivery or until regimen changed after prenatal diagnosis. c Pyrimethamine – sulphonamide combination with folinic acid alternates with spiramycin in three or four weekly cycles until delivery except in Paris,
Reims, Marseille Toulouse and Grenoble where continuous pyrimethamine – sulphonamide is given.
d Pyrimethamine – sulphadiazine: Daily dose in Lyon, Paris and Nice ¼ 50 mg/day pyrimethamine, 3 g/day sulphadiazine; in Naples ¼ 25 mg/day
pyrimethamine, 2 g/day sulphadiazine; in Milan ¼ 50 mg/day pyrimethamine, 2 g/day sulphadiazine.
e Enrollment was restricted to women who seroconverted. f Fansidar: dose in: Marseille, Toulouse and Grenoble ¼ 50 mg/week pyrimethamine, 1 g/week sulphadoxine; Reims ¼ 75 mg/2 weeks pyrimethamine,
g Daily dose in Austria ¼ 25 mg/day pyrimethamine (50 mg for first dose), 0.75 g/day sulphadiazine (1.5 g for first dose), prescribed from 16 weeks of
gestation onwards and continued until delivery. Spiramycin given before 16 weeks gestation.
h Neonatal screening for specific IgG antibodies in Guthrie card filter paper bloodspot followed by retrospective testing of stored prenatal sera.
Women were enrolled if the collaborating clinician
whom the dates for diagnosis of maternal infection, start of
considered that prenatal treatment for toxoplasmosis was
maternal treatment, amniocentesis for fetal diagnosis and
justified. Infected women were identified using two meth-
detection of fetal or infant abnormalities were not sequential.
ods. First, by detection of seroconversion during pregnancy
The case definition for congenital toxoplasmosis was the
(change from IgG negative to IgG positive specific antibo-
persistence of specific IgG beyond 12 months postnatal age:
dies). IgG negative women were re-tested monthly in France
positive parasite culture or histology of the placenta or fetal
and approximately three monthly elsewhere (Table 1). In
tissue was accepted for perinatal or fetal deaths. Absence of
centres where seronegative women were routinely tested
congenital toxoplasmosis was defined by at least one IgG
postpartum, we included infected women diagnosed after
negative result in a child not receiving treatment.
delivery. Second, we included women with IgG and IgM
Table 1 summarises the screening and treatment proto-
positive results at their first prenatal test and, in addition, a
cols for each centre. In the French and Italian centres,
rising IgG titre, low IgG avidity, high IgG titre or positive
spiramycin was started immediately after confirmation of
IgA antibodies (referred to as ‘tests for recent infection’,
maternal infection and, following diagnosis of fetal infec-
Table 1). In Stockholm, infected women were identified by
tion, was changed to pyrimethamine – sulphonamide. In
universal neonatal screening for specific IgG antibodies
some centres, pyrimethamine – sulphonamide was pre-
followed by retrospective testing of stored antenatal sam-
scribed immediately if maternal infection occurred in the
ples5 to detect seroconversion during pregnancy or recent
third trimester as a result of a high risk of fetal infection. In
infection. All positive results were confirmed in subsequent
Vienna, all infected women above 15 weeks of gestational
samples. In order to minimise selection bias due to women
age were prescribed pyrimethamine – sulphonamide unless
who were investigated for fetal abnormalities associated
fetal diagnosis was negative. None of the Stockholm women
with congenital toxoplasmosis, we excluded women in
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
The hypothesis that the earlier treatment is given, the
close to the positive test date for women who were IgG
more likely it is to be effective, underpins the rationale for
negative at the first positive IgM test. For woman i, Ni
the monthly re-testing of susceptible women. We deter-
denoted the duration of gestation at the last negative IgM
mined the effect of the interval between seroconversion and
test and Pi the duration of gestation at the first positive IgM
the first date anti-toxoplasma treatment was prescribed.
test. Ni ¼ 1 if woman i was identified by a test of recent
This interval is subsequently called ‘treatment delay’. The
infection and, if the first test was IgM positive but IgG
odds ratio for each week of treatment delay and for four
negative, Ni ¼ Àl [but R(t) places a lower bound on the
week categories (less than four, four to seven and eight or
timing of seroconversion prior to Pi]. We defined T(x) as
more weeks) was calculated taking into account the gesta-
the probability of mother to child transmission, given
tional age at maternal seroconversion. The effects of
maternal seroconversion at time point x (Ni x Pi).
maternal age, parity, symptoms at diagnosis and country
We assumed that the effects of treatment and confounders
of study on the treatment effect were tested and as only
on T(x) were additive on a logistic scale.
maternal age was significant at the 5% level, this was
The contribution to the likelihood function for a woman i
included in the model. Reported P values (two-sided) are
who seroconverted at time point x was found by multiply-
based on the assumption that the difference in deviance of
ing R( Pi À x) if IgG antibody was found at the first positive
IgM test or 1 À R( Pi À x) if no IgG antibody was found at
In view of the hypothesis that transmission may be
the first positive IgM test with the appropriate term from
delayed in early pregnancy6, we tested for an interaction
the following list: for a woman identified through serocon-
between treatment delay and gestational age (both mea-
version and with an infected child T(x), with an uninfected
sured as continuous variables). We also examined the effect
child 1 À T(x), and with a child with unknown infection
of the interval between seroconversion and amniocentesis
status P(Z j infected child) (T(x)) þ P(Z j uninfected child)
and a positive diagnosis in infected children. An asso-
(1 À T(x)). The corresponding terms for a woman identified
ciation would provide evidence of delayed transmission.
by tests of recent infection with a probability u that
Additional analyses compared untreated with treated
seroconversion occurred during pregnancy was: uT(x), for
women and first treatment with pyrimethamine – sulpho-
an infected child, 1 À uT(x) for an uninfected child, P(Z j
namide versus spiramycin, allowing for treatment delay.
infected child) (uT(x)) þ P(Z j uninfected child) (1 À
Sensitivity analyses involved restriction of the data set to:
uT(x)) for a child with unknown infection status. The
(a) seroconverting women; and (b) mother – child pairs with
complete contribution for woman i is found by taking the
complete data for congenital infection status.
sum of all time points over the range Ni to Pi.
To avoid bias, we used a statistical method7 in which
children with missing data on congenital infection status
Table 2. Number of mother – child pairs enrolled and proportion of children
contributed to infected and uninfected groups. The contri-
bution was determined by the likelihood ratios for test
results in each child for: (1) PCR analysis of amniotic
fluid; (2) specific IgM at any age in the child; and (3)
specific IgG at any age. The likelihood ratios werecalculated using data from children with complete data.
(1) and (2) were adjusted for weeks of gestation at sero-
conversion. All equivocal results were considered to be
negative and the three tests were assumed to be indepen-
dent, given congenital infection status. Likelihood ratios
were calculated for test results alone and in combination
(defined as Z in calculations given below) and multiplied
against the pre-test probability based on gestational age at
maternal seroconversion to obtain the risk of congenital
We avoided arbitrary assumptions about the timing of
seroconversion (e.g. midpoint between the last negative and
first positive test) by using an adaptation of a model
described elsewhere8. This model considers all dates
between the last negative and the first positive test (for
seroconverting women) and between conception and thefirst positive test (for women identified by tests for recent
infection). The distribution function for the interval
* Based on 1208 mother – child pairs. Percentages vary between centres
between initial IgM and IgG positive results [defined as
due to differences in gestation at seroconversion of included women.
R(t)]8 describes the increased probability of seroconversion
Further details by centre are available from the authors.
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
firmation of maternal infection, 1 was seropositive during aprevious pregnancy and 22 had fetal diagnosis beforestarting treatment. Of the 11 twins, only the first bornwas included in the analyses. The total of 1208 mother –child pairs analysed included 16 miscarriages or stillbirthsand 21 terminations (17 for toxoplasmosis). There werethree postnatal deaths.
The mean maternal age was 28.4 years (SD 4.9). In 53%
(601/1144) this was their second or subsequent delivery. Symptoms of lymphadenopathy were reported in 82 women(7%).
Table 2 shows that 62% (743/1208) of women serocon-
verted during pregnancy. Of these, 39% (288/743) wereIgG negative and IgM positive at their first positive testindicating seroconversion close to the first positive IgMdate. The remaining 38% (465/1208) were identified bytests for recent infection which included IgG and IgMpositive results at the first pregnancy test and in descendingorder of priority: rising IgG titre in 252, low IgG avidity in
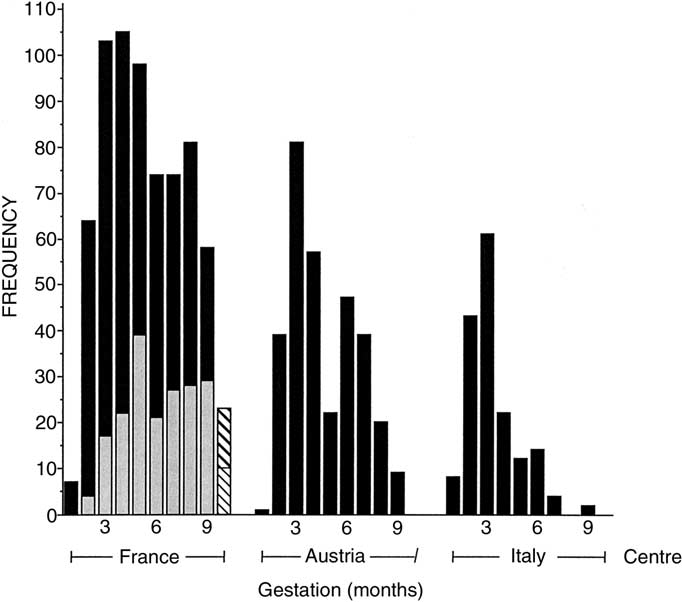
Fig. 1. The number of women is shown for each country according to
35 and other criteria in 178 (e.g. IgA positive, high IgG
month of gestation at their first positive test. In Paris, enrollment was
restricted to seroconverting women (shown in grey). The diagonal shadingdepicts women whose first positive test was at or after delivery.
Figure 1 shows all mother – child pairs by country and
gestational age at the first positive test. Except for Paris,
The study complied with research ethics requirements in
where only seroconverting women were enrolled, the
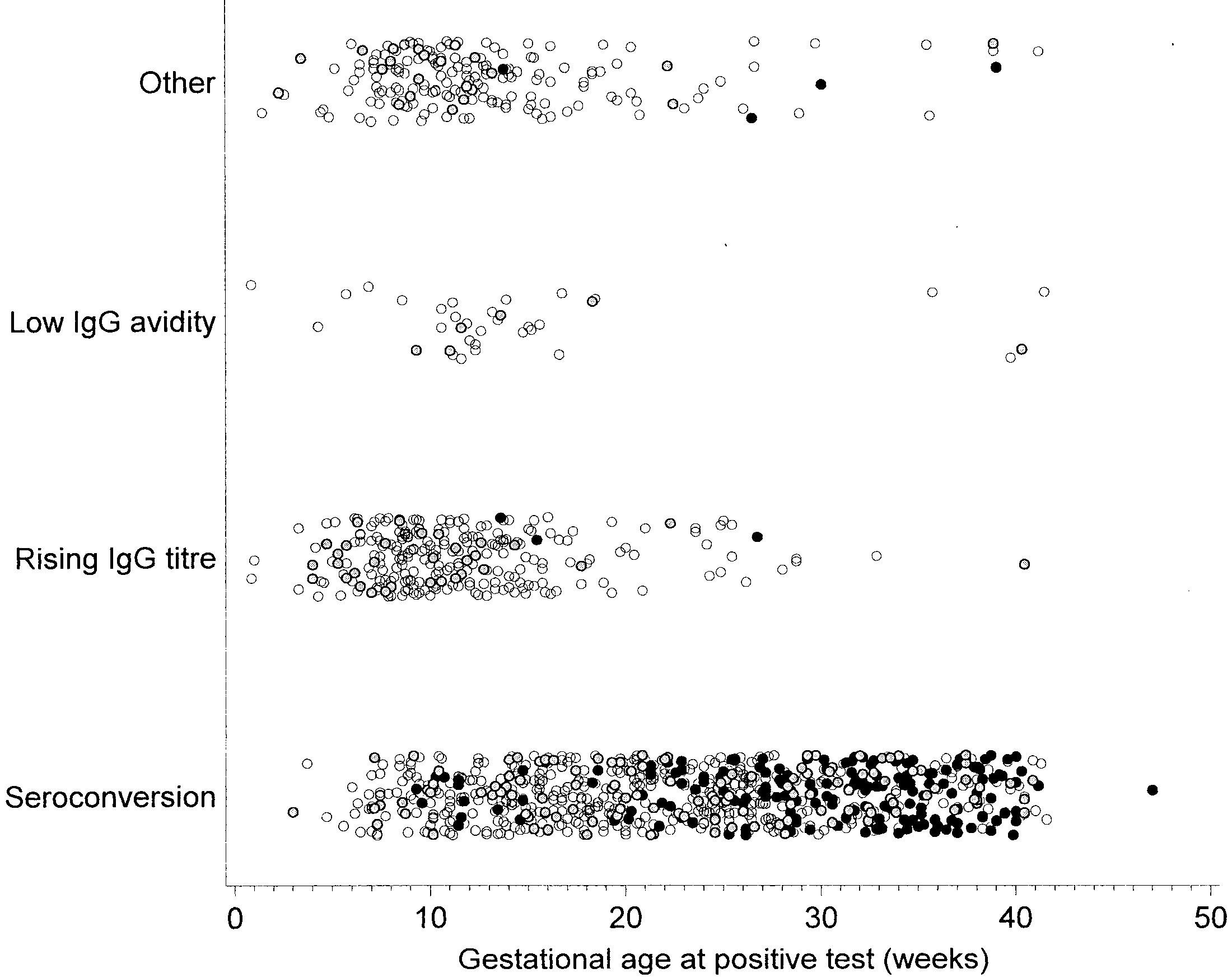
distribution was skewed towards early pregnancy. Figure2 shows the number of women identified by seroconversionand tests for recent infection (rising IgG titre, low IgG
avidity and other) by gestational age at first positive test,and child’s infection status. Only seven infected children
A total of 1260 mother – child pairs were enrolled
were born to the 465 (1.6%) women identified by tests for
between 1996 and 2000. Of these, 52 pairs were excluded:
15 were lost to follow up before pregnancy outcome, 11
Figure 3a shows the estimated number of seroconverting
were referred for fetal infection, 3 had inadequate con-
women for each week of gestation. Women identified by
Fig. 2. The scatter plot shows mother – child pairs detected by seroconversion or by tests for recent infection defined as IgM and IgG positive and: rising IgGtitre, low IgG avidity or other (e.g. IgA positive, high IgG titre). Categories are exclusive in order of priority (seroconversion excludes all others). Mother –child pairs are plotted against the weeks of gestation at the first positive test. Black dots indicate children with congenital toxoplasmosis, white dotsuninfected children and grey dots children with missing data for congenital infection status.
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
Fig. 3. The estimated number of women is plotted against the gestational age at seroconversion (weeks) according to: (a) criteria for detecting maternalinfection (seroconversion or tests for recent infection); and (b) treatment status (spiramycin, pyrimethamine – sulphonamide or no treatment).
tests for recent infection largely contributed information in
results and/or postnatal serology in 159/181 children (in
early pregnancy before the first prenatal test. Although the
22, only gestation at seroconversion was available). The
number of women enrolled by this method was large (465),
risk of mother to child transmission is shown in Fig. 4: the
their probability of postconceptional seroconversion was
risk was 9% (6.8 – 12.6) for women who seroconverted at
low. For women identified by this method before 21 weeks,
12 weeks of gestation and 83% (75.5 – 88.4) at 40 weeks of
the probability of postconceptional seroconversion was
gestation. Transmission risk, adjusted for gestation at sero-
conversion, did not differ significantly between countries
Table 2 shows the proportion of children with congenital
(Austria vs France, P ¼ 0.08; Italy vs France P ¼ 0.13).
toxoplasmosis for each centre. Classification was based on
Table 3 shows the number of women according to the
complete data in 1027/1208 (85%) children of whom 17%
type of prenatal treatment prescribed. Two-thirds were
(179/1027) had congenital toxoplasmosis. For the remain-
prescribed spiramycin alone and just over one-quarter were
ing 181 children (154 live born) with missing outcome
prescribed pyrimethamine – sulphonamide. There were few
data, the probability of congenital toxoplasmosis (24.4%,
untreated women (8.8%, 106/1208). Similar proportions of
44.2/181) was estimated using the pre-test probability of
treated and untreated women were identified by serocon-
transmission based on gestational age at maternal serocon-
version. Of 89 women who changed from spiramycin to
version, combined with the likelihood ratios for PCR
pyrimethamine – sulphonamide, most (77%, 69/89) had a
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
Fig. 4. The risk of mother to child transmission of toxoplasma infection is plotted against the gestational age (weeks) at maternal seroconversion (dotted linesshow 95% confidence intervals). The risk of transmission for seroconverting women according to trimester was: 8% (<14 weeks), 25% (14 to <28 weeks)and 60% (28 weeks to delivery).
positive fetal diagnosis. Figure 3b shows that most of the
There was no evidence for an effect of treatment delay on
untreated women seroconverted in the third trimester. In
the risk of mother to child transmission. Table 4 shows that
contrast, women first treated with spiramycin or pyrimeth-
compared with a delay of less than four weeks (between the
amine – sulphonamide seroconverted at all gestational ages
start of treatment and seroconversion), the adjusted odds
with fewest in the last month of pregnancy. The median treat-
ratio for a treatment delay of four to seven weeks was 0.77
ment delay (the interval between seroconversion and start of
(95% CI 0.34 – 1.69), and for eight weeks or more was 1.33
first treatment) for women first treated with pyrimethamine –
(0.56 to 2.89). The odds ratio for mother to child transmis-
sulphonamide was 55 days (interquartile range 33– 88) and
sion per week of treatment delay was 1.01 (0.93 – 1.08) for
for spiramycin 29 days (interquartile range 17– 46).
all women. Results were similar for seroconverting women
Women were treated promptly after their first positive
(OR 1.01; 0.93 – 1.09) and for all women with complete out-
serological test: median time six days (interquartile range
come data (OR 0.99; 0.93 – 1.06). Tests for a range of param-
1 – 17). Treatment was stopped, at least temporarily, due to
eterisations for the continuous effect of treatment delay
adverse effects in 24/1102 (2%) women of which 11 were
(fractional polynomials)9 found that none were significantly
better than the linear model used (results not shown).
Table 3. Prenatal treatment regimen prescribed to infected pregnant women. Values are expressed as n or n (%). P – S ¼ pyrimethamine – sulphonamide[sulphadiazine was prescribed to 293 women and sulphadoxine (Fansidar) to 29 women].
Amniocentesis performed for fetal diagnosis
Pyrimethamine – sulphonamideSpiramycin changed to P – S
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
Table 4. Effect of prenatal treatment on mother to child transmission of toxoplasmosis. Tests for interaction between: (a) gestational age at seroconversionand treatment delay, P ¼ 0.84; (b) type of treatment and treatment delay, P ¼ 0.23.
Effect of treatment delay*(5a) All treated women
Effect of type of treatment§(5e) All treated women
(5e) Women who seroconverted after 27 weeks of gestation
* Adjusted for gestational age at seroconversion and maternal age. y Estimated numbers of women based on weekly probability of seroconversion. z Actual number of women. § As for * and adjusted for treatment delay.
There was no difference in transmission risk between
There was also substantial variation in treatment delay for
women first prescribed pyrimethamine – sulphonamide and
both types of treatment across all centres and gestational
those prescribed spiramycin. Nor was there evidence that
ages, which increased the power of the analysis and the
transmission risk differed between untreated and treated
applicability of the results. As the study was based in
women (Table 4). This last analysis mainly applies to
regional and national reference centres, it is unlikely that
women who seroconvert late in pregnancy (see also Fig. 3b).
the lack of evidence for a treatment effect was due to sub-
We failed to detect an association between the interval be-
tween seroconversion and prenatal diagnosis and a positive
Unlike previous studies3,4,10, we included women iden-
tified by tests for recent infection to ensure that our resultsare applicable to the first trimester when few seroconver-sions occur. In routine practice, women identified in the
first trimester are an important group accounting in somecentres for up to 80% of all treated women (see Table 2).
We found no evidence for an effect of the timing or type
As many of these women acquired infection before con-
of prenatal treatment on the risk of mother to child
ception, we used a statistical model to take account of the
transmission. The results were robust to sensitivity analyses
probability of seroconversion after conception.
and are consistent with previous studies that allowed for
The main limitation of the study was the failure to exclude
gestational age at maternal seroconversion2 – 4.
benefits or harms which would be sufficient to change
The strengths of the study were prospective enrollment
clinician practice. For example, the upper and lower confi-
and data collection, the high rate of follow up and estima-
dence limits for the odds ratio for treatment delay of eight
tion of congenital infection status in mother – child pairs
weeks or more compared with less than four weeks (OR
with missing data, all of which reduced selection bias7.
1.33; 95% CI 0.56 – 2.89) are consistent with clinically
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
important beneficial (a near threefold increase) and harmful
and development of the statistical approach; R. Mears,
(a 44% decrease) effects of treatment on mother to child
M. Simic, C. Fogg and D. Tillen (London) for assisting
transmission. Based on simulations, the study had approx-
with data management; Birgit Panzenboeckshe and
imately 85% power to detect an odds ratio for transmission
Professor Dr Horst Aspo¨ck (Vienna), Christelle Depla-
of 1.5 in women treated after eight weeks versus women
tihre and Monique Baudet (Lyon), Lisa Engman, Sven
within four weeks of seroconversion (equivalent to an odds
Wiklund and Sten Ivarsson (Stockholm) for assisting
ratio of 1.1 per week of treatment delay). A further problem
with data collection; and Catherine Peckham, Rodolphe
was that the comparison of treated with untreated women
Thiebaut and Mario Cortina-Borja for their comments on
was limited to the few untreated women who seroconverted
in the last trimester and the results may not be generalisable
Collaborators in the European Multicentre Study on
to the first and second trimesters. This problem was common
to previous studies2 based on routine practice3,4,11. Des-
Clinical centres (in order of number of mother – child pairs
monts and Couvreur12 reported a 50% reduction in trans-
included): A. Prusa, M. Hayde, A. Pollak (University
mission risk in women treated with spiramycin compared
Children’s Hospital, Vienna); M. Wallon, F. Peyron (Hoˆpital
with untreated women but subsequently acknowledged that
de la Croix Rousse, Lyon); P. Thulliez, S. Romand (Institut
this crude comparison failed to take into account the fact that
de Puericulture, Paris); W. Buffolano (Universita di Napoli,
untreated women were infected later in pregnancy11. Given
Naples); J. Franck, H. Dumon, P. Bastien, E. Issert (Hoˆpital
the steep rise in transmission risk, an apparent treatment
de la Timone, Marseille); M.-H. Bessieres (Hoˆpital de Ran-
effect can easily arise if women infected late in pregnancy
gueil, Toulouse); N. Ferret, P. Marty (Hoˆpital de l’Archet,
are compared with those infected early in pregnancy without
Nice); B. Evengard, G. Malm (Huddinge Hospital, Stock-
taking into account gestational age at seroconversion.
holm); H. Pelloux, H. Fricker-Hidalgo, C. Bost-Bru (Centre
One explanation for our results is the lack of power to
Hospitalier Universitaire de Grenoble); E. Semprini, V.
detect a significant effect. Another possible explanation is
Savasi (Milan); M. Paul (University Medical Sciences,
that transmission of parasites occurs early on before treat-
Poznan); E. Petersen (Statenseruminstitut, Copenhagen).
ment is started13. Finally, although we found no evidence
Co-ordinating Centre: R. Gilbert, L. Gras, L. Valenti
for an effect according to the type of antibiotic prescribed,
(Institute of Child Health, London).
the possibility remains that some antibiotics are moreeffective than others. We considered all women treated withpyrimethamine – sulphonamide combinations together and
could not explore the effect of pyrimethamine – sulphadoxine(Fansidar) due to the small number of women treated.
1. Wallon M, Liou C, Garner P, Peyron F. Congenital toxoplasmosis:
what is the evidence that treatment in pregnancy prevents congenitaldisease? BMJ 1999;318:1511 – 1514.
2. Gilbert RE, Dunn DT, Wallon M, et al. Ecological comparison of the
risks of mother to child transmission and clinical manifestations ofcongenital toxoplasmosis according to prenatal treatment protocol.
We were unable to demonstrate a beneficial effect of the
Epidemiol Infect 2001;127:113 – 120.
timing or type of prenatal treatment on the risk of mother to
3. Foulon W, Villena I, Stray-Pedersen B, et al. Treatment of toxoplas-
child transmission, but could not exclude a clinically
mosis during pregnancy: a multicentre study of impact on fetal trans-mission and children’s sequelae at age 1 year. Am J Obstet Gynecol
important effect. There is now sufficient uncertainty to
justify randomised controlled trials of treated versus
4. Gilbert RE, Gras L, Wallon M, Peyron F, Ades AE, Dunn D. Effect
untreated women14. In addition, studies are required to
of prenatal treatment on mother to child transmission of Toxoplasma
determine whether prenatal treatment has a beneficial
gondii: a cohort study of 554 mother – child pairs in Lyon, France.
effect on the severity of clinical manifestations of congen-
Int J Epidemiol 2001;30:1303 – 1308.
5. Evengard B, Petterson K, Engman M-L, et al. Low incidence of tox-
ital toxoplasmosis and, more importantly, on the child’s
oplasma infection during pregnancy and in newborns in Sweden.
Epidemiol Infect 2001;127:121 – 127.
6. Romand S, Wallon M, Franck J, Thulliez P, Peyron F, Dumon H.
Prenatal diagnosis using polymerase chain reaction on amniotic fluid
for congenital toxoplasmosis. Obstet Gynecol 2001;97:296 – 300.
7. Magder LS, Hughes JP. Logistic regression when the outcome is
measured with uncertainty. Am J Epidemiol 1997;146:195 – 203.
This paper was prepared by R. Gilbert and L. Gras with
8. Dunn D, Wallon M, Peyron F, Petersen E, Peckham CS, Gilbert RE.
input from the collaborators in the European Multicentre
Mother to child transmission of toxoplasmosis: risk estimates for clin-
ical counselling. Lancet 1999;353:1829 – 1833.
The project was funded by the European Commission
9. Royston P, Ambler G, Sauerbrei W. The use of fractional polynomials
to model continuous risk variables in epidemiology. Int J Epidemiol
The authors would like to thank the following: David
10. Gilbert R, Dunn D, Wallon M, et al. Ecological comparison of the
Dunn, for help with the study design and implementation
risks of mother-to-child transmission and clinical manifestations of
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
congenital toxoplasmosis according to prenatal treatment protocol.
and Newborn Infant, 5th edition. Philadelphia: Saunders, 2001:
Epidemiol Infect 2001;127:113 – 120.
11. Couvreur J, Desmonts G, Thulliez P. Prophylaxis of congenital tox-
14. Peyron F, Wallon M. Options for the pharmacotherapy of toxoplasmo-
oplasmosis. Effects of spiramycin on placental infection. J Antimicrob
sis during pregnancy. Expert Opin Pharmacother 2001;2:1269 – 1274.
Chemother 1988;22(Suppl B):193 – 200.
15. Lebech M, Joynson DH, Seitz HM, et al. Classification system and
12. Desmonts G, Couvreur J. Congenital toxoplasmosis. Prospective
case definitions of Toxoplasma gondii infection in immunocompetent
study of the outcome of pregnancy in 542 women with toxoplasmosis
pregnant women and their congenitally infected offspring. Eur J Clin
acquired during pregnancy. Ann Pediatr Paris 1984;31:805 – 809.
Microbiol Infect Dis 1996;15:799 – 805.
13. Remington JS, McLeod R, Thulliez P, Desmonts G. Toxoplasmosis.
In: Remington JS, Klein J, editors. Infectious Diseases of the Fetus
D RCOG 2003 Br J Obstet Gynaecol 110, pp. 112–120
Claus-Peter Czaya Terry and Susanne Waite [[email protected]] Gesendet: Montag, 20. M ärz 2006 02:38 "Undisclosed-Recipient:;"@mta45-2.us4.outblaze.com Betreff: NIH Announces Kennedy's Disease Clinical Trial Wichtigkeit: Hoch KDA RESEARCH UPDATE _________________________________________ Date: March 19, 2006 To: All KDA Associates Subject: National Inst
Well, At this point things are not too good. I went in for surgery on 8/31. I had my pre-opt the day before and Dr. Baxt said I looked bigger than in my pictures. That made me worried especially since he seemed less confident about getting me to a C than over the phone. The procedure went fine, from what I know. I was asleep the entire time. When I woke up I felt incredably alone and I wanted my m
 PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
firmation of maternal infection, 1 was seropositive during aprevious pregnancy and 22 had fetal diagnosis beforestarting treatment. Of the 11 twins, only the first bornwas included in the analyses. The total of 1208 mother –child pairs analysed included 16 miscarriages or stillbirthsand 21 terminations (17 for toxoplasmosis). There werethree postnatal deaths.
PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
firmation of maternal infection, 1 was seropositive during aprevious pregnancy and 22 had fetal diagnosis beforestarting treatment. Of the 11 twins, only the first bornwas included in the analyses. The total of 1208 mother –child pairs analysed included 16 miscarriages or stillbirthsand 21 terminations (17 for toxoplasmosis). There werethree postnatal deaths.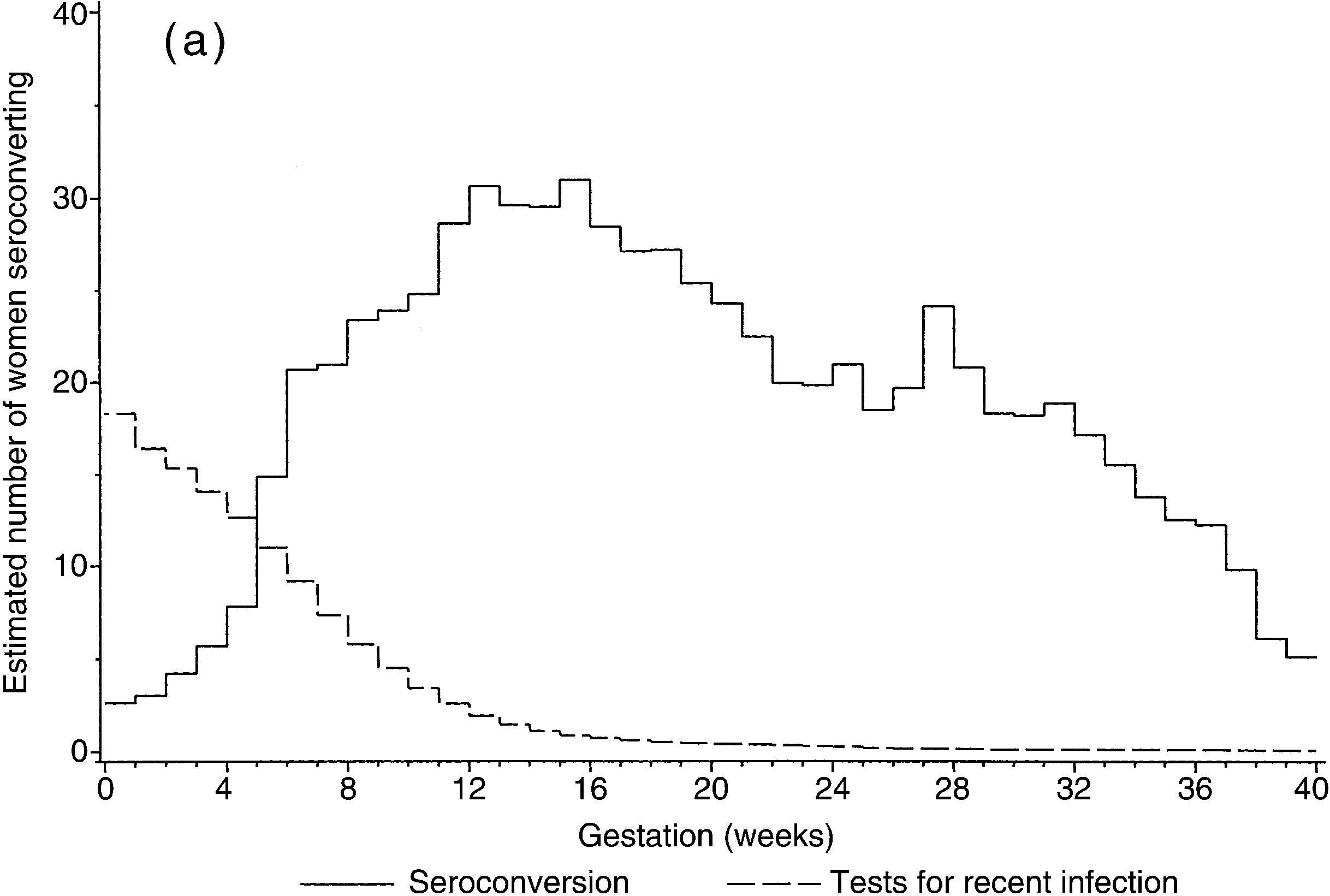
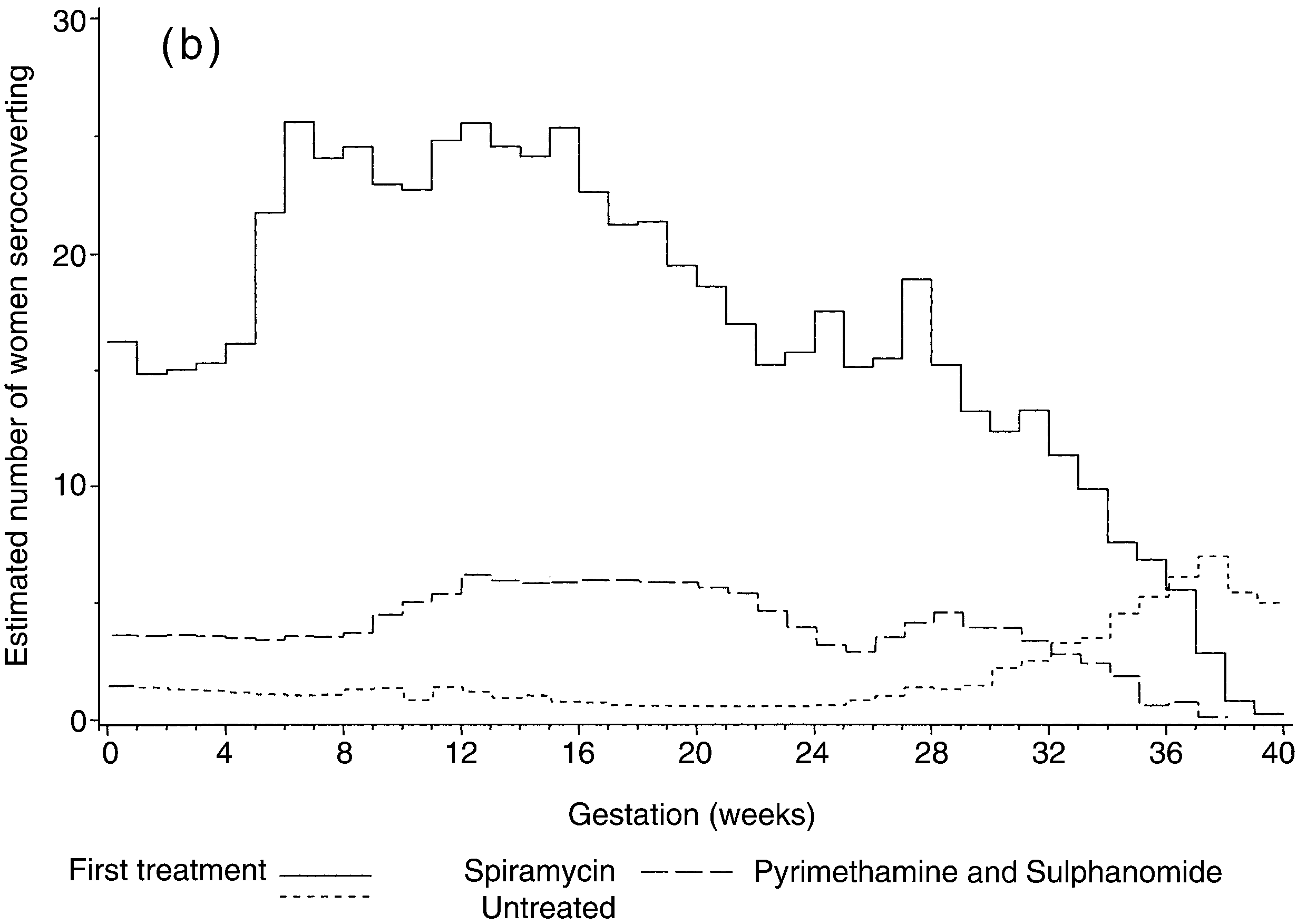 Fig. 3. The estimated number of women is plotted against the gestational age at seroconversion (weeks) according to: (a) criteria for detecting maternalinfection (seroconversion or tests for recent infection); and (b) treatment status (spiramycin, pyrimethamine – sulphonamide or no treatment).
Fig. 3. The estimated number of women is plotted against the gestational age at seroconversion (weeks) according to: (a) criteria for detecting maternalinfection (seroconversion or tests for recent infection); and (b) treatment status (spiramycin, pyrimethamine – sulphonamide or no treatment).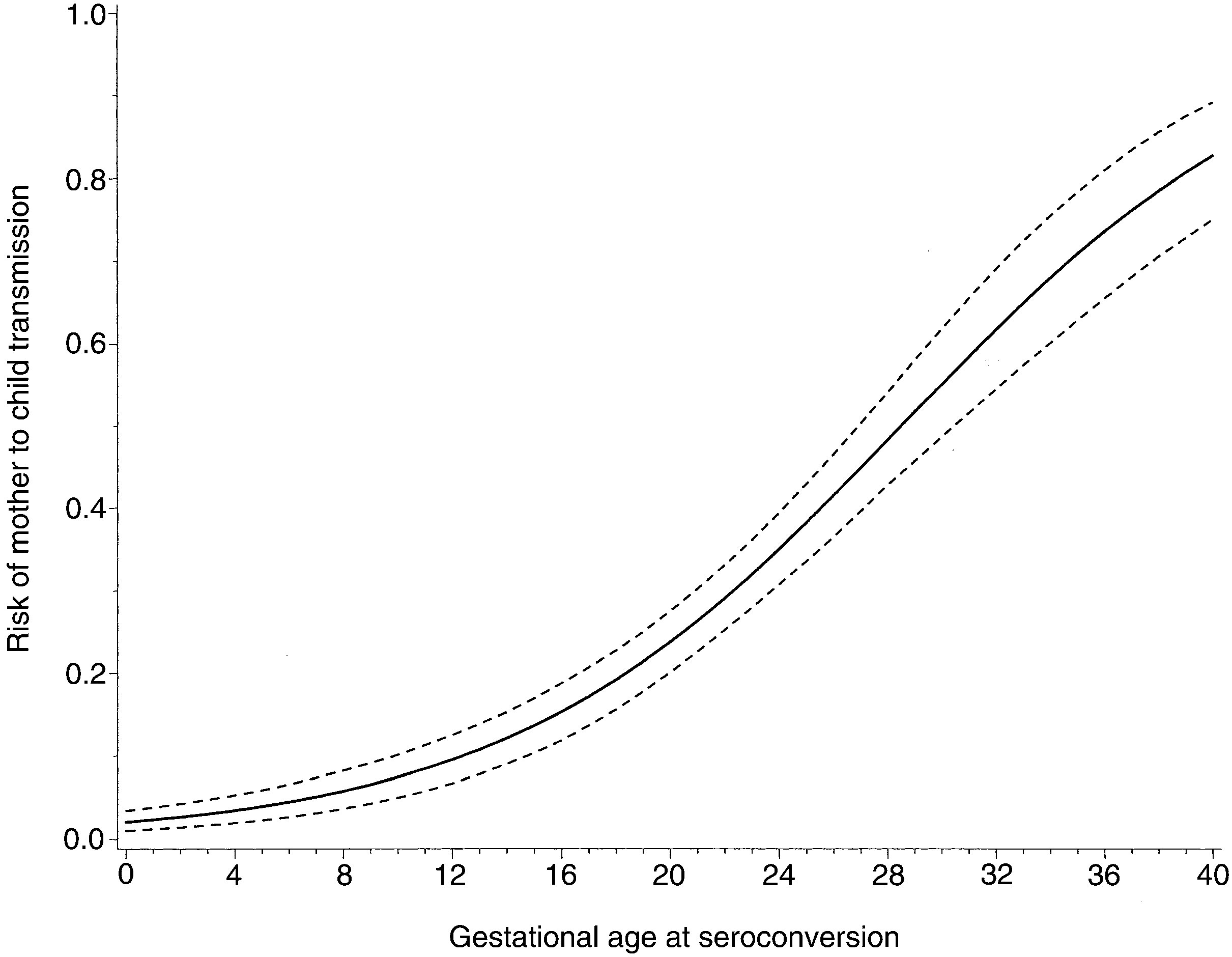 PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
Fig. 4. The risk of mother to child transmission of toxoplasma infection is plotted against the gestational age (weeks) at maternal seroconversion (dotted linesshow 95% confidence intervals). The risk of transmission for seroconverting women according to trimester was: 8% (<14 weeks), 25% (14 to <28 weeks)and 60% (28 weeks to delivery).
PRENATAL TREATMENT TO PREVENT CONGENITAL TOXOPLASMOSIS
Fig. 4. The risk of mother to child transmission of toxoplasma infection is plotted against the gestational age (weeks) at maternal seroconversion (dotted linesshow 95% confidence intervals). The risk of transmission for seroconverting women according to trimester was: 8% (<14 weeks), 25% (14 to <28 weeks)and 60% (28 weeks to delivery).