Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Familydoctor.co.uk
Understanding Indigestion and Ulcers
Professor C.J. Hawkey and Dr N.J.D. Wight
Published by Family Doctor Publications Limitedin association with the British Medical Association
IMPORTANT
This book is intended not as a substitute for personal
medical advice but as a supplement to that advice for
the patient who wishes to understand more about his
In particular (without limit) you should note that
advances in medical science occur rapidly and some
information about drugs and treatment contained in this
booklet may very soon be out of date.
All rights reserved. No part of this publication may be reproduced, or stored in
a retrieval system, or transmitted, in any form or by any means, electronic,
mechanical, photocopying, recording and/or otherwise, without the prior
written permission of the publishers. The right of Professor C.J. Hawkey and
Dr N.J.D. Wight to be identified as the authors of this work has been asserted
in accordance with the Copyright, Designs and Patents Act 1988,
Family Doctor Publications 1999–2006
Family Doctor Publications, PO Box 4664, Poole, Dorset BH15 1NN
ISBN-13: 978-1-903474-46-9 ISBN-10: 1-903479-46-9 Professor C.J. Hawkey is Professor of Gastroenterology A very common symptom
Virtually everyone has had indigestion at some time,
and for most people it’s simply a minor nuisance. More
often than not, it happens when you’ve overindulged
in food or alcohol or eaten something that doesn’t
agree with you, and it lasts for only a relatively short
has worked in many hospitals inEngland treating and researching
In these situations, you can either wait for the
symptoms to subside or treat yourself with a remedy
Dr N.J.D. Wight is a specialist
from the pharmacist without needing to see a doctor.
For some people, however, the symptoms can be
persistent and so severe that they interfere with
everyday life. They may be caused by some undiagnosed
problem within the digestive system that needs to be
properly identified and, if necessary, treated by a
This book will help you distinguish between minor
symptoms that you can safely treat yourself with theadvice of a pharmacist and those that need furtherinvestigation.
The word ‘indigestion’ means different things to
• If your indigestion does not get better with simple
different people, but mostly it is used to describe
over-the-counter remedies, you should make a
discomfort in the central upper abdomen related in
some way to eating or swallowing. Other commonsymptoms include:
Whether or not to see your GP is discussed in detail onpages 13–15. Remember, if self-help doesn’t work, or
if you are worried, it is always best to see your GP.
• a burning sensation in the chest (heartburn) often
linked with food or liquid coming up into the throat
KEY POINTS
or the back of the mouth (known medically asgastro-oesophageal reflux)
• belching or burping gas or wind into the mouth.
affecting most people at some time intheir life
Treating indigestion
If you get such symptoms only occasionally, you should
ask your pharmacist about over-the-countertreatments, which can be used safely to treat the odd
bout of indigestion. You should also read the section in
this book on lifestyle changes (see page 16) and makeany necessary changes to reduce your chances of
■ This booklet will help you to treat yourself
further attacks. Simple measures like these will usually
and also help you decide if it is necessary
be all that is needed to solve your problem, but in
certain circumstances it is best to see your GP:
• If you have difficulty swallowing, unintentional
weight loss, abdominal swelling, persistent vomitingor vomiting blood, you should make an urgentappointment to see your GP.
• If you have indigestion and are taking certain types
of drugs, either prescribed or bought from thechemist, you should make a routine appointment tosee your GP (the types of drugs that may causeindigestion are described in detail on pages 72–4). The structure of the mouth The tongue, teeth and saliva work together to start the process of digestion. There are three pairs of salivary glands that aid the tasting, chewing and swallowing of food. How the digestive system works
Many people sometimes have only a vague idea of the
size, shape, position and function of the stomach andother digestive organs. This section of the book gives abrief outline of the normal process of digestion andwhat each of the main parts of the digestive systemdoes. If this is all familiar to you, just skip this account
and move straight on to page 10, where the maintypes of indigestion are described.
To extract nutrients from the food that we eat we
need to digest it. First the food has to be changed into
a liquid or semi-liquid form. Then, complex substancessuch as fats and proteins have to be broken down into
move food round your mouth to chew it, and it also
smaller chemical units that can be absorbed through
contains an enzyme called salivary amylase that starts
the walls of the intestine into the bloodstream.
to digest carbohydrates such as sugars and starches. It is slightly acid and, when you’re not actually eating,
The mouth
it goes on being produced and helps to keep your
The process of digestion begins in your mouth, where
mouth and teeth clean and stop plaque developing on
the teeth and tongue chop large pieces of food into
your teeth. People who have conditions in which
smaller ones. The salivary glands release saliva into the
salivary production is reduced often experience a dry
mouth to mix with the food. Saliva makes it easier to
mouth, difficulty swallowing and increased tooth decay. The stomach and intestines The major abdominal organs and digestion
Once the food is chewed and softened in the mouth,
Ingested food passes down the oesophagus and into the
the tongue pushes it to the back of the throat, where
stomach, where it is churned and mixed thoroughly withdigestive juices secreted by the stomach lining. Further digestive
muscles propel it down the oesophagus (or gullet). The
enzymes are added to the food in the duodenum.
food passes from the oesophagus into the stomachthrough a muscular one-way valve, the lower oeso-phageal sphincter, which prevents the contents of thestomach from being forced back into the chest whenthe stomach contracts or when you lie flat.
Functions of the stomachThe stomach is a muscular J-shaped sac that forms thewidest part of the digestive tract. It has three main
1. It acts as a storage container, so that within a
few minutes we can swallow all the food needed
2. It plays a large part in the physical and chemical
processes of digestion. Food in the stomach is
churned and crushed, although you notice thisonly when the activity is excessive because yourstomach does not contain the same number ofsensory nerves as other parts of the body, such
as the skin. Glands within the stomach lining
produce a powerful acid and enzymes that helpbreak down the constituents of food into simpler
chemical compounds. The walls of the stomach
are normally protected against acid attack by a
layer of protective mucus, but, if this is reduced
or damaged, it may lead to ulcer formation. Theoesophagus doesn’t have this protective liningand so is more easily damaged by acid. Section through stomach wall The swallowing process To allow you to swallow food safely, two involuntary events occur: the soft palate rises to close off the nasal cavity and the
epiglottis tilts to seal the windpipe. 3. Food may stay in the stomach for several hours,
during which time the acid will destroy most ofthe bacteria and other micro-organisms that may
have contaminated it. Very little is absorbed
directly into the bloodstream through the
stomach walls, apart from a few substances such
When the stomach has done its work the liquidised
food is then pushed onwards through another valve,the pylorus, into the duodenum – the first few inches
of the small intestine. Here further chemicals are addedto neutralise the stomach acid, together with enzymes
from the pancreas to help digest carbohydrates, fats
and proteins, and bile from the liver to help digest fats.
The digested food then passes into the remaining 20
called gastro-oesophageal reflux and is described in
feet (six metres) of small intestine, so called because,
although it is long, its diameter is smaller than that
Stomach acid may also cause problems if it attacks
of the large intestine. The chemical breakdown is
the lining of the stomach itself, known as peptic ulcer
completed in the small intestine and the chemical
disease, described in detail later (see page 61). Our
constituents of the meal are absorbed into the blood
understanding of peptic ulcer disease has changed
greatly in recent years, thanks to the discovery of an
The main tasks of the large intestine are to
infective agent called Helicobacter pylori – you’ll find
reabsorb the water that is used in digestion and to
out more about this later (see page 64).
eliminate the undigested food and fibre.
The third common cause of indigestion, called non-
ulcer dyspepsia, is something of a puzzle. This is the
What can go wrong?
diagnosis given to people who have persistent
Almost everyone experiences occasional attacks of
symptoms of indigestion but in whom the tests for
indigestion, which are usually quite brief. We may feel
gastro-oesophageal reflux and stomach ulcers are
blown out or distended after a large meal, and get
normal. Dyspepsia is actually just the medical name for
some relief when we bring up wind. Most of the wind
indigestion. Some people with this type of indigestion
that we bring up is a result of swallowing air as we
are eventually found to have a disorder affecting
eat, but some is produced by a chemical reaction in
another part of the digestive system, such as gallstones
the stomach or from carbonated, fizzy drinks. The
or the irritable bowel syndrome. In others, the pain is
solutions are to eat less, eat more slowly and go easy
found to be caused by some disorder of the lower ribs
with fizzy drinks. You may have discovered for yourself
and muscles of the abdominal wall. Most people with
that certain foods – fried onions, for example – give you
non-ulcer dyspepsia, however, seem to have sensitive
an uncomfortable sensation in the upper abdomen that
stomachs that cause symptoms at times of emotional
lasts for only an hour or so. Again the answer is obvious:
stress. The condition is described in greater detail on
don’t eat those foods, or avoid them where possible.
Very occasionally, indigestion may be the first
Causes of indigestion
symptom of a more serious condition such as stomach
More persistent indigestion is usually linked with the
cancer. Stomach cancer is becoming less common than
acid produced by the stomach. If the valve at the lower
in the past and it occurs far less frequently than peptic
end of the oesophagus becomes weak or defective,
ulcer disease or gastro-oesophageal reflux. It is
the acid juices in the stomach may be pushed back
described in greater detail on pages 93–9.
upwards into the oesophagus, causing a burningsensation (heartburn). This is often troublesome atnight, when you lie flat. The underlying condition is
KEY POINTS
■ During the normal digestion process, food
■ The stomach produces acid and pepsin to
■ If the lining of the stomach is weakened,
or if acid production is altered, thenindigestion can occur
Assessing the seriousness of your condition Probably three of every four people who suffer from indigestion never seek medical advice: they relieve their symptoms by a few changes to their lifestyle and by taking over-the-counter treatments, such as antacids or acid-blocking drugs, bought from the chemist every now and then.
One of the aims of this book is to help you decide
whether and when to consult your doctor. You shouldmake an appointment if any of the three followingsituations applies to you. Sinister symptoms See your GP without delay if you have any symptoms of the kind that doctors call ‘sinister’, by which they mean symptoms that might be caused by a serious disease such as stomach cancer. Early diagnosis and treatment give the best chance of a cure, so get prompt medical advice if you have any of the following symptoms:
D O Y O U N E E D T O S E E Y O U R D O C T O R ?
over-the-counter medicines or if you need to takethese medicines for a prolonged period of time.
Your doctor may need to arrange various tests and
investigations before beginning treatment – this iscovered on pages 28–41.
• persistent vomiting• vomiting blood or material that looks like coffee
KEY POINTS
• passing altered blood in the motions (this makes
Medicine interactions
Make a routine appointment to see your GP if you
develop indigestion while taking any of the following
• you have vomited blood or material that
• certain blood pressure drugs known as calcium
channel antagonists (nifedipine, amlodipine and
• you have passed altered blood in your
• nitrate drugs for treatment of angina (such as
• you are over 40 and have indigestion for
• your indigestion has not responded to
• bisphosphonate drugs used for the treatment of
osteoporosis (alendronate and risedronate are
• steroid tablets• non-steroidal anti-inflammatory drugs such as
Prolonged indigestion Make a routine appointment to see your GP if your indigestion does not go away despite the use of
PUBLIKATIONEN Priv.-Doz. Dr. med. Guntram W. Ickenstein 1995 - 2012 Originalarbeiten: Muders F, Friedrich E, Luchner A, Pfeifer M, Ickenstein GW , Hamelbeck B, Riegger G, Elsner D Hemodynamic changes and neurohumoral regulation during development of congestive heart failure in a model of epinephrine-induced cardiomyopathy in conscious rabbits Muders F, Luchner A, Friedrich E, Ickenstein G
Introduction GOLD 2006 PRESENTATION Tertiary bis-phosphines of the form R P-(CH ) -PR (n = 1 – 4 and R = Me, Et, t-Bu and Ph) and cis-R PCH=CHPR (R = Ph) are often used as chelating ligands for a wide range of transition metals.[1-4] These ligands have shown wider applications in metal complexation reactions and have attracted much attention, especially in the fields of medicine and cat

 Professor C.J. Hawkey is
Professor C.J. Hawkey is 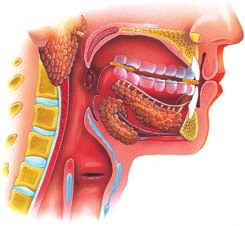 The structure of the mouth
The structure of the mouth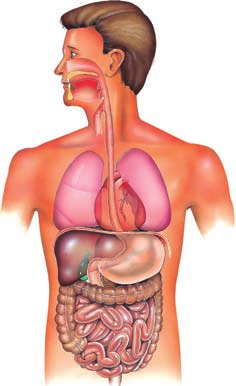 The stomach and intestines
The stomach and intestines



 Section through stomach wall
Section through stomach wall