Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Exemfoamkit.co.uk
Human Reproduction vol.12 no.7 pp.1582–1588, 1997 The spontaneous pregnancy prognosis in untreated subfertile couples: the Walcheren primary care study H.K.A.Snick1, T.S.Snick1, J.L.H.Evers2,4 and
new forms of treatment, or to wait further for a spontaneous
J.A.Collins3
pregnancy to occur. Clinical prediction models have beendeveloped in order to assist the clinician in estimating a
1Department of Obstetrics and Gynaecology, Ziekenhuis Walcheren,
couple’s spontaneous baseline pregnancy chance (Cramer et al.,
Koudekerkseweg 88, 4382 EE Vlissingen, 2Department ofObstetrics and Gynaecology, Academisch Ziekenhuis Maastricht,
1979; Leridon and Spira, 1984; Comhaire, 1987; Bostofte
and The University of Maastricht, P.O. Box 5800, 6202 AZ
et al., 1993; Eimers et al., 1994; Collins et al., 1995). Prediction
Maastricht, The Netherlands and 3Department of Obstetrics and
models based on empirical observations are more useful to
Gynecology and Department of Clinical Epidemiology and
clinicians if the inception cohort is similar to the patients in
Biostatistics, McMaster University, 1200 Main Street West, Room
their practice and if there is an unambiguous outcome such as
live birth (Collins et al., 1995). Ideally therefore, one should
4To whom correspondence should be addressed
derive an empirical prediction model from data collected in a
The spontaneous pregnancy prognosis of couples in a
group of subfertility patients, living in a well-defined geograph-
primary care situation has never been studied. Prognostic
ical area and visiting a primary care fertility centre. Walcheren,
models have been developed for referral populations only.
a former island in the Dutch province of Zeeland, appears to
We wished to develop a prognostic model to estimate the
be almost ideally suited for this kind of research. The composi-
likelihood of live birth and the impact of prognostic factors
tion of its population of 110 000 is a genuine reflection of the
among untreated subfertile couples in a primary care
population of The Netherlands as a whole, both in demographic
situation. With this aim, we conducted a cohort follow-up
and socio-economic respects. It has only one hospital, where
study of 726 couples in the peninsula of Walcheren, a
one and the same gynaecologist (H.K.A.S.) has been respons-
geographically isolated, but demographically and socio-
ible for all subfertility care delivered between 1985 and today. economically representative area of an industrialized West-
Only persistent factors with a proven fertility-impairing effect
ern society, The Netherlands. Of the Walcheren population,
are treated, and only if a treatment is available which is based
9.9% exhibit subfertility complaints at least once during
on sound scientific evidence. The lines of communication
their lifetime. There were 201 live birth conceptions during
between general physicians and specialist care providers are
9915 months of untreated observation. The cumulative rate
short. For all patients the care they receive at the hospital
of conceptions leading to live births was 52.5% when all
constitutes the first contact with specialist fertility investigation
of the untreated observations were considered, and 72.0%
and treatment. It may be considered primary fertility care,
in the subgroup of 342 couples who remained untreated
since general physicians do not start fertility treatment in the
throughout their follow-up. The relevant prognostic factors
Walcheren region. The social situation on this former island
in this primary care subfertility population were: abnormal
allows for an almost complete long-term follow-up. post-coital test, tubal defect, ovulation defect, and duration of subfertility. A prediction score based on these factors would be accurate in ~76–79% of cases. Live birth prognosis Materials and methods can be estimated with sufficient accuracy to be useful in Setting counselling subfertility patients, and in planning clinical management.
The former island of Walcheren is situated in the south-west of TheNetherlands. To the south the river Schelde flows. A ferry boat
Key words: infertility/prognostic factors/prognostic model/
service provides a connection to the mainland of The Netherlands
spontaneous pregnancy prognosis/subfertility
and Belgium. To the west is the North Sea, and to the north a damconnects Walcheren to another small former island, Noord-Beveland,which does not possess a hospital. Finally to the east a dam givesaccess to the former island of Zuid-Beveland, with a hospital at
Introduction
Recent years have brought numerous new treatment modalities
Walcheren has 110 000 inhabitants, 24 200 of whom are females
for subfertile couples, many of which have subsequently
between 15 and 44 years of age (mean of the figures for 1990–93).
disappeared, but some of which appear to offer realistic
1319 births take place per year (mean of the figures for 1989–93).
improvements. All assisted reproduction treatments, apart from
In 1994, 39 170 people were employed for Ͼ15 h a week. Per 1000
their medical advantages, also carry a medical, financial,
inhabitants, the following numbers were active in the respective
emotional and social burden. Therefore, clinicians are in need
employment categories (numbers for The Netherlands in parentheses):
of guidelines to counsel their patients whether to accept these
agriculture and fishing 3.1 (6.5), industry, building, construction and
European Society for Human Reproduction and Embryology
Spontaneous pregnancy prognosis
transport 124 (118), trade and travel 65 (73), services 160 (170)
activities until registration at the clinic; female and male partner’s
(Source: Dutch Central Office of Demography Statistics, CBS, 1993).
age, age at the time of registration.
Only one hospital serves the whole population of Walcheren. The
The diagnostic protocol was according to the recommendations of
four consultant gynaecologists in the hospital see all gynaecological
the ESHRE workshop on ‘unexplained infertility’ (Crosignani et al.,
and obstetric cases by themselves. There are no residents or house
1993; ESHRE, 1995), and included clinical examination of both
officers employed. One gynaecologist (H.K.A.S.) coordinates all
partners, one (i.e. the first) semen analysis according to WHO (1987)
fertility investigations and sees all problem cases himself. He super-
criteria, recording of a basal body temperature (BBT) chart, a mid-
vises the fertility laboratory, and performs all morphology assessments
luteal progesterone determination, a post-coital test (PCT), and
in the semen analyses in person. The department of internal medicine/
hysterosalpingography (HSG). HSG was substituted by laparoscopy
endocrinology and the department of urology refer all subfertility
as the initial tubal factor investigation if the history was suggestive
patients for evaluation to the senior author. The special interest in
of a serious pelvic infection or if abnormal findings were encountered
subfertility in the Walcheren hospital, and the availability of an
at pelvic examination. If HSG was abnormal, a laparoscopy was done
artificial insemination service with donor spermatozoa, cause an influx
in one of the subsequent cycles. If HSG was normal, laparoscopy
of patients from Noord- and Zuid-Beveland into the region. These
patients, ~30 in number, were excluded from the present analysis as
Semen analysis was judged normal if sperm concentration was
their inclusion would have created an erroneously high incidence of
Ͼ20ϫ106/ml, if grade A progressive motility was Ͼ25% and if the
infertility complaints. General physicians in Walcheren do not refer
percentage of normal morphology was ജ20% (WHO, 1987). A WHOsemen defect was diagnosed if one or more of these criteria were not
subfertility patients to hospitals outside Walcheren. This enabled the
met. Oligozoospermia was defined as Ͻ5ϫ106 motile sperm in the
study of a primary population with fertility problems in a geographic-
ally well-defined and demographically and socio-economically repres-
The menstrual cycle was considered ovulatory if serum progesterone
entative area of The Netherlands with an almost complete follow-up.
was Ͼ18 nmol/l and the duration of the menstrual cycle was Ͻ8weeks. An ovulation defect was diagnosed if one or both criteria
Patients
Patients were admitted to the study if they wished to conceive and
The PCT was considered positive if more than one forward-moving
had a history of at least 1 year of unprotected intercourse without
spermatozoon was found in the whole cervical mucus sample, between
pregnancy, if no pregnancy existed at the moment of registration, and
8 and 16 h after intercourse. In patients with regular menstrual cycles
if they were permanent inhabitants of Walcheren. Patients who had
the PCT was scheduled on day 15 or 16 before the expected onset
had a sterilization were excluded, as were patients from outside
of the next menstrual period. In patients with irregular cycles the
PCT was timed after tracking the appearance of the cervical mucus.
Between 1 January 1985 and 31 December 1993, 726 couples
As soon as the mucus was considered to reflect the preovulatory
fulfilled these criteria, for a mean of 81 couples per year. This means
state, the couple was advised to have intercourse. Clear cervical
that in a 30 year reproductive life span (ages 15–44), if this number
mucus, with Ͼ6 cm spinnbarkeit, without leukocytes, was considered
were to remain stable, 2430 couples would seek fertility care, or
preovulatory. The PCT was repeated every 48 h until the BBT chart
9.9% of the population (Hull et al., 1985). Follow-up ended on 1
showed a persistent rise and/or (from 1988 onwards) the dominant
September 1995. Of 724 couples (99.7%), the reproductive outcome
follicle (ജ20 mm) had disappeared on ultrasound examination. A
was available at that moment, either by direct contact with the couple,
PCT defect (abnormal PCT) was diagnosed if the best PCT showed
when they still frequented the clinic, or by their completing a written
0 or 1 forward-moving spermatozoon. Data analysis of PCT by χ2-
questionnaire, or by the senior author calling them or their general
test indicated that this test performs much better as a predictor of
physician by telephone. Only two couples were lost to follow-
infertility in a primary care population than in the patient groups
from which prognostic models are more usually derived.
During the period of investigation, 94 patients qualified for in-
Endometriosis was scored according to the revised American
vitro fertilization (IVF) treatment and were referred to an IVF centre
Fertility Society classification (1985). Only stages 3 and 4, or cysts
(outside Walcheren). Another 19 couples were referred for further
Ͼ6 cm diameter were taken into account in defining endometriosis
analysis or specialized treatment to referral centres outside the region:
in the present investigation. Laparoscopy was performed according
for microsurgical repair of epididymal (n ϭ 8) or tubal (n ϭ 8)
to the ESHRE (1995) guidelines for the investigation of the infertile
obstruction, or for specialized diagnosis of andrological problems
couple. This implies that an unknown proportion of patients with
(n ϭ 2). One couple was referred to a centre outside Walcheren for
endometriosis (undefined by stage, but unlikely to harbour stage 3 or
gonadotrophin treatment of difficult ovulatory disturbances.
4 disease) may exist within the unexplained infertility group. This is
During the period of investigation, seven couples sought a second
typical of most studies based on similar investigative protocols.
opinion in a hospital outside Walcheren without referral by the
A normal tubal status was diagnosed as no abnormalities on HSG
gynaecologist concerned. None of them became pregnant. No patient
and/or laparoscopy: no obstruction of either tube, no fertility-impairing
was seen for obstetric care at the Walcheren hospital after infertility
peritubal adhesions. A tubal defect was diagnosed if one or more of
investigation or treatment elsewhere without referral. Notwithstanding
the Dutch system of home deliveries, of all pregnant patients in
Pregnancy was defined as amenorrhoea of ജ6 weeks in combination
Walcheren 80% are seen at some time during their pregnancy by one
with a positive urine pregnancy test, or positive ultrasound findings.
For a diagnosis of abortion or ectopic pregnancy to be made, surgicalpathology confirmation was required. The product of conception was
Definitions and management
defined as a child from a pregnancy duration of 28 weeks onwards.
The following definitions were used: infertility, no conception after
For the purpose of these analyses, success was defined as live birth;
1 year of unprotected intercourse; primary infertility, no prior preg-
cases in which unsuccessful pregnancy occurred were considered
nancy in this partnership; secondary infertility, a prior pregnancy in
failures and observations were censored at the time of the last
this partnership, regardless of the pregnancy outcome; duration of
menstrual period. A live birth was defined further as a living child 1
infertility, the interval in months from discontinuation of contraceptive
H.K.A.Snick et al.
for minimal endometriosis by a locum tenens gynaecologist, onceclomiphene citrate was prescribed to a woman with a normal ovulatorymenstrual cycle.
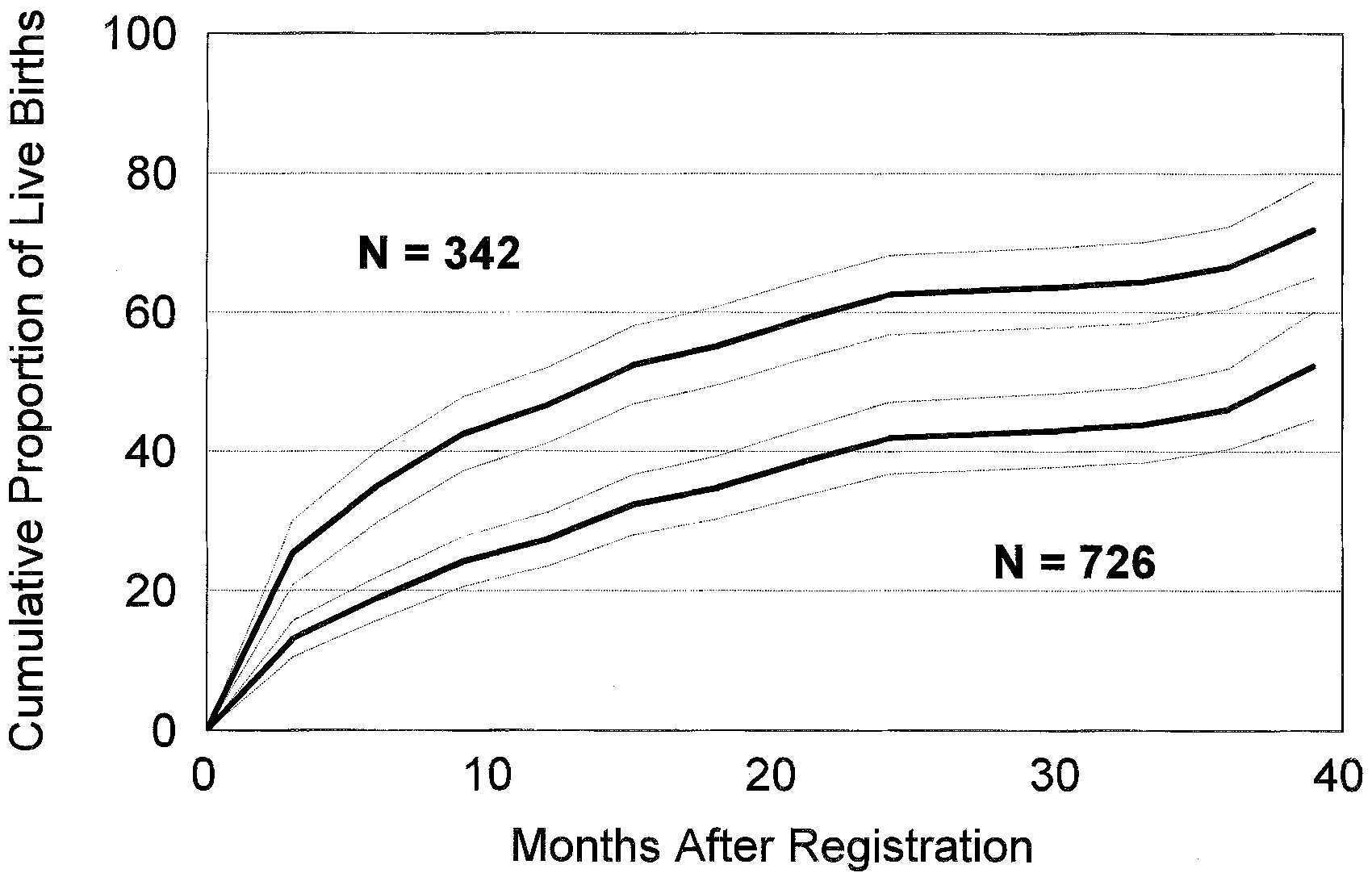
To concentrate on untreated conceptions, all calculated rates
excluded conceptions that occurred if either partner was treated afterregistration. For live birth calculations, all couples were included inthe denominator, and the numerator was the number of untreatedconceptions. In the life-table and approximate fecundity calculations,the observation months among untreated couples were combined withthe observation months before the first treatment among treatedcouples. Cumulative live birth rate was the life-table estimate of timeto conception in cases associated with live births. Approximatefecundity was the number of live births per 100 months of untreated
Figure 1. Cumulative rate of live births (and 95% CI) among 342
untreated couples (upper curve) and 726 couples (lower curve). Theupper curve excludes observations prior to treatment among the 384
Statistical analysis
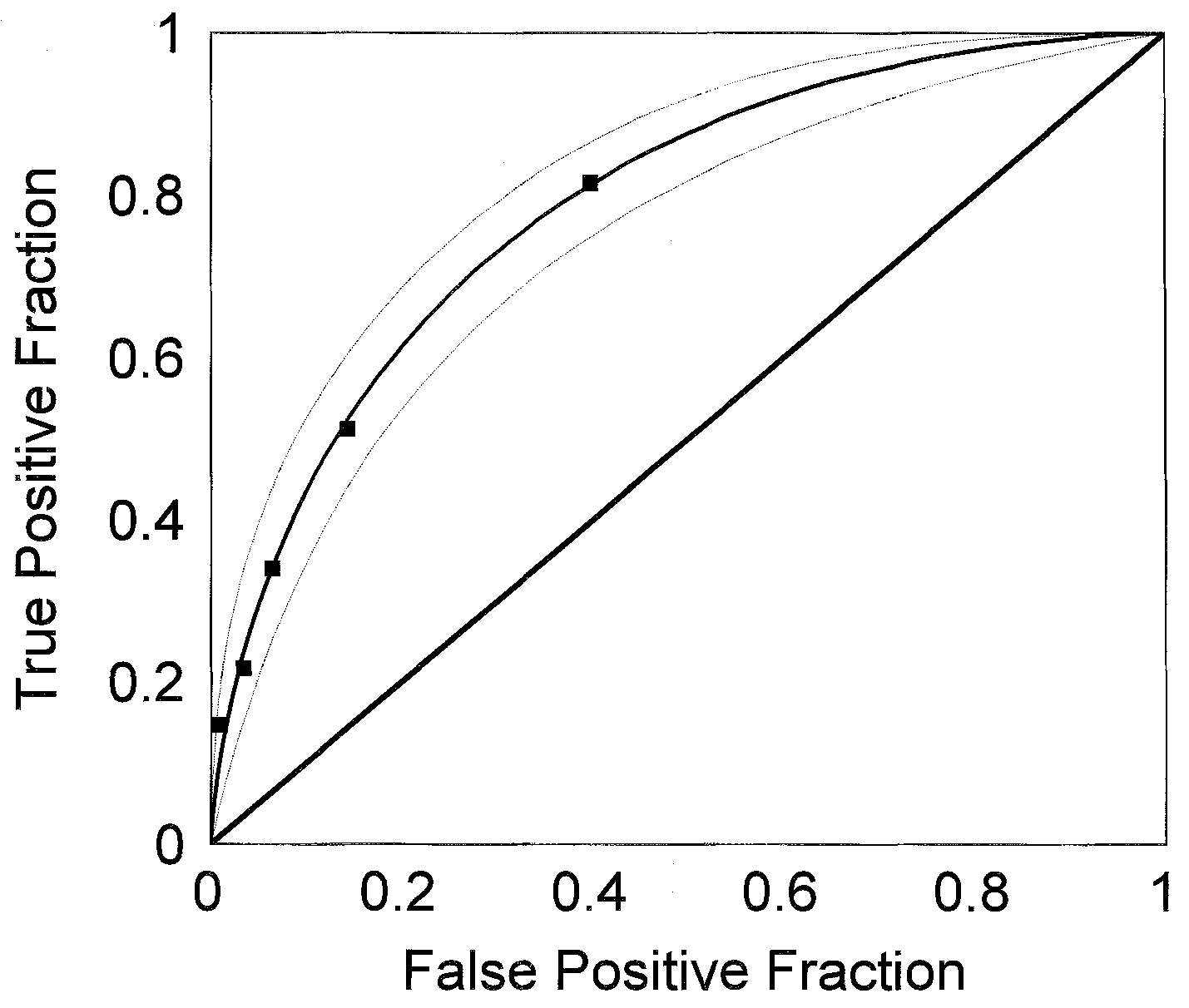
Prognostic variables were evaluated by means of Pearson’s χ2(categorical variables) or analysis of variance (continuous variables). The strategy for selecting variables to include in the proportionalhazards analysis was based on these univariate analyses (Cox, 1972),and on life-table analysis of live birth during follow-up. Termsrepresenting pregnancy history, duration of infertility, female age,and diagnosis were considered. Binary variables for duration (cut-offpoint at 24 months) and female age (cut-off point at 30 years) wereconstructed in order to estimate relative risks. Semen analysis wasentered as normal or abnormal depending on published criteria forsperm concentration, progressive motility and normal morphology(WHO, 1987). Semen variables also were used to calculate totalmotile sperm count per ejaculate. The significance level for enteringcovariates into the proportional hazards analysis models was 0.05,and for removing covariates 0.051. Figure 2. Receiver operating characteristics curve for the
The prediction score was computed from the β coefficients of the
prediction of live birth based on the proportional hazards model in
terms in the model. In order to assess the accuracy of the prediction
Table III. Closed squares are the observed operating points and the
model, receiver-operating characteristics (ROC) curves were estimated
smoothed line is the estimated binormal receiver-operating
for the prediction of live births in the data, and the area under the
curve (AUC) with 95% confidence intervals (95% CI) was calculated. The reproducibility of the prediction score was evaluated by applyingthe model to a previously published independent set of data (Collins
Table I. Live birth and other outcomes among 726 infertile couples by Observation and outcome data
The mean duration of infertility was 20.7 (SD 13.9) months
and the mean age was 29.1 (SD 4.5) years for 726 female
partners and 31.2 (SD 5.3) for 511 male partners (the latter
being collected only from December 1988 onward). Twenty-
nine per cent of the couples had secondary infertility defined
as infertility after a previous pregnancy in the partnership andin a further 7% the female partner had a pregnancy in a
All treatment was ‘evidence-based’. As a rule of practice, only
previous partnership. The status of all patients at 1 September
persistent factors with a proven fertility-impairing effect were treated,
1995 is shown in Table I. The mean time under observation
and only if a treatment was available which was based on sound
or treatment was 24.5 months (SD 27.6, median 15.0, range
scientific evidence. The only exception to this rule was embolization
1–124.9). Of the 495 pregnancies, 411 were live births; these
of a varicocele grade III, which was performed in couples with
live birth conceptions occurred after a mean of 13.2 months
severe sperm abnormalities after ജ2 years of otherwise unexplained
of observation before and during treatment (SD 15.5, median
Patients’ preferences or requests for treatments other than those
There were 342 (47%) untreated couples, and they contrib-
based on scientific evidence were not honoured. The patient was
uted 5918 months of observation (mean 17.3, SD 22.5, median
counselled extensively on the findings instead. As a consequence, onan individual basis, apart from embolization of a varicocele, unproven
9.0, range 1–120 months). There were also 3997 months of
treatment was used only twice: once danazol was prescribed
observation before treatment for 384 treated couples (mean
Spontaneous pregnancy prognosis Table II. Live birth rate, cumulative live birth rate and approximate fecundity by diagnosis group
10.4, SD 15.2, median 5.0, range 1–124 months). The resulting
Table III. Relative likelihood of live birth among 726 infertile couples
9915 months of untreated observations accounted for 56% of
the total of 17 797 months of observations. The untreatedcouples had 239 conceptions and 201 live births; the mean
time to conception for untreated couples who had a live birth
was 8.1 months (SD 10.0, median 4.0, range 1–73 months). The 201 live births among the 342 untreated couples accounted
The cumulative rate of conceptions leading to live birth
was 52.5% (95% CI 44.7–60.2) when all of the untreated
observations were considered and 72.0% (95% CI 65.0–79.0)
in the subgroup of couples who remained untreated throughout
Effect of prognostic factors on live birth
Live birth rate, cumulative live birth rate at 36 months
Data from follow-up in the Walcheren region. Model statistics were:
and approximate fecundity were highest in couples with
selected model, χ2 ϭ 88.129, 4 degrees of freedom, P Ͻ 0.0001; alternate
unexplained infertility (Table II). These rates also were high
model, χ2 ϭ 70.106, 6 degrees of freedom, P Ͻ 0.0001. The endometriosis
in the less severe subgroup of the male defect diagnostic
variable did not enter either model. PCT ϭ post-coital test.
category. Live birth rates also were high in couples withshorter duration of infertility and secondary infertility and lowin couples with an abnormal PCT. Female age was not
Table IV. Area under the curve for receiver-operating curve (ROC) analyses
significantly associated with live birth rates among these
for prediction scores and observed live births in untreated infertile couples
A proportional hazards analysis to evaluate the independent
contribution of prognostic factors included four covariates inthe final model (Table III). The relevant variables are PCT
result, tubal status, ovulation status and duration of infertility
respectively, in order of importance. This model is referred to
as the ‘selected model’. The PCT result variable entered the
model, while variables defining semen defect by World Health
aWalcheren: the present data; CITES: untreated prognosis among 2198
Organization standards (WHO, 1987) or by the presence of a
couples in the Canadian Infertility Therapy Evaluation Study (Collins et al.,
total motile count Ͻ5ϫ106 per ejaculate did not enter the
model. An ‘alternate model’ was developed in which the PCTresult variable was not offered to the analysis. The alternate
model would be accurate in 79% of cases. AUC values Ͻ50%
model included three additional variables, one representing
imply an inoperative model, and 100% would constitute a
male function (the WHO semen variable), one representing
perfect prediction model. Confidence limits for areas under
female function (female partner’s age Ͻ30 years) and one
the ROC curves indicate that the small observed difference
representing undefined couple factors (secondary infertility).
between the selected (four-variable) model and the alternate(six-variable) model is not significant (Table IV). The perform-
Evaluation of the prediction score
ance of the prediction model was validated in an independent
The prediction score based on the proportional hazards model
data set which has been published previously (Collins et al.,
in the sample of 726 couples was evaluated by ROC analysis
1995). Because the comparison data did not include PCT
(Figure 2). The AUC indicates that the selected prediction
results, the alternate model was used for this validation test. H.K.A.Snick et al.
The AUC was 67% when the alternate model was evaluatedagainst observed live birth rates in the previously publisheddata set. The AUC with the previously published score waslower when it was applied either in the original group ofCanadian couples or in the present data set. Discussion
Only large prospective studies of subfertile couples visitingprimary care fertility centres with a long-term (and complete)follow-up may shed light on the baseline pregnancy prognosisin untreated subfertility. Studies from tertiary care facilities
Figure 3. Cumulative live birth rate with 95% CI for infertile
may present less reliable data in this respect since their patient
couples in Walcheren (n ϭ 726) and in the Canadian Infertility
populations may be selected, and their composition skewed
Therapy Evaluation Study (CITES, n ϭ 2198), truncated after 2years of observation for this figure only.
towards those with as yet undiscovered — but persistent —fertility-impairing factors. Many new treatment options forsubfertile couples have been introduced in recent years. Only
one calculated from secondary and tertiary care populations
some of them have been subjected to controlled trials in which
(e.g. 21.2% in the Canadian Infertility Therapy Evaluation
one group was randomly allocated to receive a placebo or no
Study (CITES; Figure 3), reflecting a different composition of
treatment. On the other hand, only in the minority of cases,
the respective study populations, notwithstanding their identical
i.e. those associated with azoospermia, prolonged amenorrhoea
inclusion criteria of subfertility. When applying models, this
or bilateral tubal obstruction, can the cause of infertility be
difference should impact on the decision about when to resort
identified easily. For the remaining couples, the interpretation
of diagnostic test results is not straightforward, and the choice
Proportional hazards analysis showed the likelihood of live
of treatment often lacks a rationale. Growing concern exists
birth during untreated observation to be influenced predomi-
regarding the potential disadvantages, and even risks, of some
nantly by three diagnostic variables (abnormal PCT, tubal
of the newer treatment modalities, especially since they appear
defect and ovulation defect) and by one clinical variable
to be applied ever more liberally in patients whose fertility
(duration of infertility Ͻ24 months). These four variables
may sometimes be only marginally impaired. Under such
were included in the so-called ‘selected model’ (Table III). If
circumstances (often counterproductive) overtreatment is
abnormal PCT was not offered to the model, its place could
be taken by abnormal semen (WHO, 1987) or oligozoospermia
The Walcheren follow-up study presents data collected in
(total motile count Ͻ5ϫ106), but if all three variables were
726 couples in the course of a 9 year review period of primary
available, only abnormal PCT entered. Even when we used a
fertility care in the only hospital of a geographically isolated,
cut-off point for total motile count at Ͻ 1ϫ106 per ejaculate
but demographically and socio-economically representative
[identifying 91 (12.5%) of cases as abnormal] its contribution
area of an industrialized Western country, The Netherlands.
was only marginally significant. The presence of this variable
The 726 couples represent 9.9% of the Walcheren population,
reduced the significance of the abnormal PCT variable, so that
seeking medical care for subfertility problems at least once
it was associated with P ϭ 0.0089 and a χ2 to remove equal
during their reproductive life span. Strict diagnosis and treat-
to 6.83. When abnormal PCT was not offered to the model,
ment protocols were adhered to, and only evidence-based
the information that it contributed seems to have been replaced
treatment was instituted. If no such treatment was available
by one male variable (WHO semen defect), one female variable
for the couple under consideration, they were counselled
(age Ͻ30 years), and one couple variable (secondary infertility)
extensively on the findings instead. Management was expectant
(‘alternate model’; Table III). In the Walcheren data, median
in such cases. This allows for the calculation of the baseline
duration of infertility is 16 months, compared with the Canadian
pregnancy prognosis in untreated subfertility couples from a
data where the median was 36 months. In our group, diagnostic
representative population in a developed country. The couples
assessments have much more powerful effects on the prognosis,
described in this study had a shorter duration of infertility
and indefinite variables are less important (female age, second-
(mean 20.7 Ϯ 13.9 months) than in most published studies,
ary infertility and duration of infertility simply indicating the
which may be explained by the fact that most other studies
presence of unknown factors). Apparently, as the duration of
considered patients from referral institutions, whereas our
infertility increases, factors which are as yet undiscovered
patients visited the Walcheren hospital for their initial fertility
become more important than known factors in estimating
work-up. Given the short lines of communication between
general physicians and specialist care providers in Walcheren,
Only a handful of prognostic models have yet accrued
the regional organization of fertility care, and the demographic
adequate evidence of accuracy, generality, and effectiveness
characteristics of the population in the present investigation,
(Anonymous, 1995). The prediction model based on the
we propose our study to reliably reflect baseline fertility
observations in the Walcheren population was tested by means
prognosis in untreated couples. This baseline prognosis is
of ROC curves and AUC. It was then validated in an independ-
much better (2 year cumulative live birth rate 41.9%) than the
ent previously published population, the CITES group of
Spontaneous pregnancy prognosis
subfertility patients (Collins et al., 1995). To allow for evaluat-
Table Va. Average baseline prognosis of live birth
ing our prediction model in the CITES group, which did not
(ABPLB) after 3, 6, 12, 24 and 36 months of
require PCT results to be collected, the PCT parameter was
made unavailable, and this resulted in our alternate (six-
variable) model (Table III), which included the WHO semendefect parameter. The predicted likelihood of live birth derived
from our alternate (six-variable) prediction model was com-
pared with the observed births in the Walcheren and the
Canadian patient groups respectively. These live birth event
rates were submitted to an ROC analysis program generatingROC curves and AUCs plus their 95% CI (Table IV): theAUC was 76% when the Walcheren alternate model was
Table Vb. Effect of prognostic factors, expressed in
applied to the Walcheren data, and, significantly worse, 67%
multiplication factors (MF) of the baseline prognosis
when our model was applied to the Canadian data. It should
be remembered that the Canadian model applied to the
Canadian data rendered an AUC of 62% in a split training/
validation sample set-up (Collins et al., 1995). The Canadian
model applied to the Walcheren data reached 65%, indicating
that the probability of the Canadian model correctly predicting
which of two Walcheren couples will conceive first is 65%,
as compared to 67% when our model is used in two Canadian
couples. There was no significant difference between the AUC
of our selected (four-variable) model, 79%, and of our alternate
(six-variable) model, 76%, when applied to our own data.
In the 1995 CITES publication, ovulation defect was not
Live birth rate prognosis after 3 to 36 months ϭABPLBϫMF(s).
selected into the model, whereas ovulation defect was asignificant component of both the selected and alternateWalcheren models. As noted above, the duration of infertility
of a pregnancy, would be a frequent reason for couples
in the Canadian couples was longer than in the Walcheren
selectively dropping out of prediction studies, this might reduce
couples. Ovulation defects are easily treated in primary care,
the accuracy of the models derived from these studies to
and only the most difficult cases would be referred. Therefore
predict spontaneous live births. In contrast to many studies
a lower proportion of the Canadian ovulation defects would
reporting prediction models, in the present study loss to follow-
be likely to resolve spontaneously and lead to untreated
up was virtually non-existent (0.3%).
The present study offers a model for the prediction of live
It has already been mentioned that the couples described in
birth among untreated subfertile couples, seeking reproductive
this study had a shorter duration of infertility than those in
health care for the first time, in a developed western country.
the Canadian study. With longer duration of infertility, the
In order to allow prediction for an individual couple, we
most fertile couples will have conceived and the most easily
constructed a simplified model for the clinical prediction of
treatable disorders will have been successfully treated. These
average cumulative live birth rate for various future time
couples therefore do not come to the secondary or tertiary
periods and prognostic factors (Tables Va and Vb). This model
care clinics that usually publish prediction models and do not
allows estimation of the fertility prognosis of a couple by
contribute to the data set published from these clinics. This
multiplying their baseline prognosis by the relative hazard for
will have profound effects on the composition of the study
each clinical predictor present in that particular couple. For
population, on the conception figures in this group and on the
example, a couple with primary infertility of 1 year duration,
prediction models derived from data obtained in this group.
a female partner aged 28 years, a normal PCT, and oligozoo-
Those not conceiving by a median of 36 months are less likely
spermia has an estimated 12 month cumulative live birth
to conceive. This group with persistent infertility is more likely
rate equivalent to 41.1% (27.4%ϫ1.5) in the selected (four-
to harbour unknown factors which are as yet undiscovered.
variable) model, and to 34.5% (27.4%ϫ1.5ϫ1.4ϫ0.6) in the
These factors are relatively more important in the untreated
alternate (six-variable) model. In this way, the prognostic
prognosis than the known factors, but they are unknown and
model presented here combines important items of patient data
therefore are not included in the prediction score. Thus the
to predict untreated clinical outcome in patients with impaired
prediction score developed in the Canadian long-duration
fertility. The model is of potential value in counselling patients,
group explains less of the observed live birth prognosis in the
in deciding on their referral for secondary care, in estimating
short-duration Walcheren population seeking primary care
the effect of treatment, and in selecting uniform comparison
groups of patients for clinical trials. Also, if no results from
Another factor which may affect reliability of prediction
randomized clinical trials are available, the outcome of a
models is the proportion of patients lost to follow-up. If the
particular treatment modality can be compared to the approxi-
occurrence of a pregnancy, or for that matter the non-occurrence
mated spontaneous pregnancy rate in the group of subfertility
H.K.A.Snick et al.
patients studied. In our opinion, the most important asset ofthe present study is that it offers the possibility to estimatelive birth rates among untreated subfertile couples from aprimary care environment with sufficient accuracy to be usefulin the clinical management of subfertility patients by primaryfertility care providers. The difference between the resultsfrom the present study and those from academic fertility centrespublished before, underlines the importance of assessing thesimilarity of the inception cohort of the study to the patientsin one’s own practice. Acknowledgement
F.H.Comhaire MD, Department of Internal Medicine, State UniversityHospital, Ghent, Belgium, is acknowledged for his help in thepreparatory phase of this project. References American Fertility Society (1985) Revised classification of endometriosis. Fertil. Steril., 43, 351–352.
Anonymous (1995) Commentary: Prognostic models: clinically useful or
quickly forgotten? Br. Med. J., 311, 98–100.
Bostofte, E., Bagger, P., Michael, A. et al. (1993) Fertility prognosis for
infertile couples. Fertil. Steril., 59, 102–107.
Collins, J.A., Burrows, E.A. and Willan, A.R. (1995) The prognosis of live
birth among untreated infertile couples. Fertil. Steril., 64, 22–28.
Comhaire, F.H. (1987) Simple model and empirical method for the estimation
of spontaneous pregnancies in couples consulting for infertility. Int. J. Androl., 10, 671–680.
Cox, D.R. (1972) Regression models and life tables. J. R. Statist. Soc., 34,
Cramer, D.W., Walker, A.M. and Schiff, I. (1979) Statistical methods in
evaluating the outcome of infertility therapy. Fertil. Steril., 32, 80–86.
Crosignani, P.G., Collins, J., Cooke, I.D. et al. (1993) Recommendations of
the ESHRE workshop on ‘unexplained infertility’. Hum. Reprod., 8, 977–000.
Eimers, J.M., Te Velde, E.R., Gerritse, R. et al. (1994) The prediction of the
chance to conceive in subfertile couples. Fertil. Steril., 61, 44–52.
ESHRE (European Society for Human Reproduction and Embryology) (1995)
Investigation and treatment of infertile couples: ESHRE guidelines for good clinical and laboratory practice. Hum. Reprod., 10, 1246–1271.
Hull, M.G.R., Glazener, C.M.A., Kelly, N.J. et al. (1985) Population study of
causes, treatment, and outcome of infertility. Br. Med. J., 291, 1693–1697.
Leridon, H. and Spira, A. (1984) Problems in measuring the effectiveness of
infertility therapy. Fertil. Steril., 41, 580–586.
World Health Organization (1987) Laboratory Manual for the Examinationof Human Semen and Semen–Cervical Mucus Interaction. CambridgeUniversity Press, Cambridge. Received on January 6, 1997; accepted on May 6, 1997
translated from the Swedish by McKinley Burnett ‘When you hear the tone – ding-a-ling – it means it’s time to turn the page. Now we’ll begin.’ The voice on the tape had changed. It almost sounded like a man now, although he knew it was a lady. Once again he openedthe Bambi book to the first page and listened to the story on thetape player. He knew it by heart. He had known it fo
• Schleimhaut-Candidosen, einschließlichErgebnisse von Kulturen und andere Labor-Diflucan ® i.v. 2 mg/ml, Infusionslösungverfügbar sind, sollte die antiinfektive The-rapie entsprechend angepasst werden. Die offiziellen Leitlinien zum angemessenenGebrauch von Antimykotika sind zu berück-1 Durchstechflasche mit 50 ml Infusionslö-1 Durchstechflasche mit 100 ml Infusionslö-1 Durchs
 H.K.A.Snick et al.
H.K.A.Snick et al.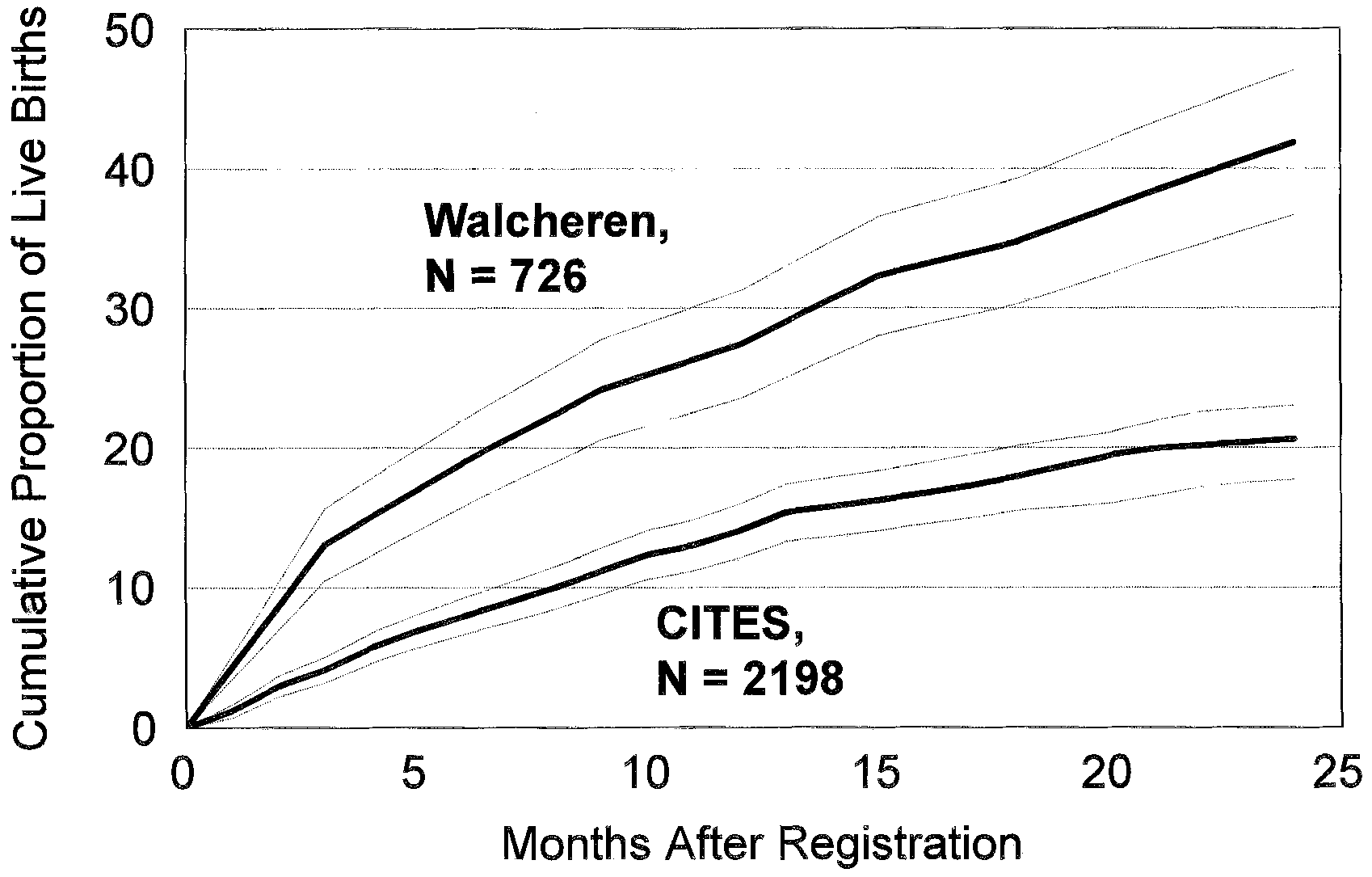 H.K.A.Snick et al.
H.K.A.Snick et al.