Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Drkathleenpage.org
NIH Public Access Author Manuscript Curr Diab Rep. Author manuscript. Interventions to Preserve Beta-Cell Function in the Management and Prevention of Type 2 Diabetes Kathleen A. Page and Division of Endocrinology and Diabetes, Department of Internal Medicine, Keck School of Medicine, University of Southern California, 1333 San Pablo Street; BMT-B11, Los Angeles, CA 90033, USA Tamar Reisman Department of Internal Medicine, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
Kathleen A. Page: [email protected]; Tamar Reisman: [email protected]Abstract
The International Diabetes Federation estimates that there are currently 336 million peopleworldwide who have type 2 diabetes (T2DM), and the global prevalence of diabetes has more thandoubled since 1980. The rapid rise in rates of T2DM echoes a similar rise in rates of obesity,which causes insulin resistance and places an increased insulin secretory demand on pancreatic βcells. While diabetes is diagnosed clinically by elevated plasma glucose levels, loss of β-cellfunction is progressive over time and β-cell dysfunction is far advanced by the time diabetes isdiagnosed. Methods for preserving or restoring β-cell function are important for the preventionand treatment of T2DM. Interventions that reduce body fat or that change fat biology provide thebest evidence for slowing or arresting the deterioration of β-cell function that causes T2DM. Theseinterventions should form the basis of interventions to prevent and treat T2DM, particularly earlyin its course. Keywords
Diabetes; Prevention; β-cell function; Glucose; Type 2 diabetes
Introduction
The global prevalence of diabetes mellitus has more than doubled since 1980 and isexpected to continue to rise at alarming rates [1]. An estimated 336 million peopleworldwide now have T2DM [2]. T2DM results from an interaction between genetic andenvironmental factors that impair β-cell function and insulin action. Diabetes is diagnosedclinically by elevated plasma glucose levels, however, loss of β-cell function is progressiveover time and β-cell dysfunction is far advanced by the time diabetes is diagnosed clinically[3, 4]. Patients with impaired glucose tolerance have <50 % of normal β-cell function [5–7]and patients with T2DM have <15 % of normal β-cell function for their degree of insulinresistance [8], demonstrating the progressive nature of β-cell dysfunction in the course ofT2DM. Therefore, methods for preserving or restoring β-cell function are important in our
Springer Science+Business Media New York 2013
Correspondence to: Kathleen A. Page, [email protected]. Disclosure No potential conflicts of interest relevant to this article were reported.
attempts to prevent and treat T2DM. In this review, we discuss current evidence for causesof the progressive loss of β-cell function in T2DM, and the effects of current therapeutic
strategies on preservation of β-cell function and the prevention and treatment of T2DM. Pathogenesis of Type 2 Diabetes β-cell Compensation for Insulin Resistance
Diabetes is defined clinically as an increase in plasma glucose levels. Plasma glucose levelsare determined by the sensitivity of tissues to insulin and by the amount of insulin secretedby the pancreatic β cells. A number of factors, including lack of exercise, obesity, andvisceral fat are major determinants of insulin resistance [4].
Normally, increases in insulin resistance are matched by a compensatory increase in insulinsecretion by the β cells, and the relationship between insulin resistance and insulin secretionis defined by a hyperbola [9]. Based on this hyperbolic relationship, β-cell compensation canbe determined by the disposition index, defined as the product of insulin secretion andinsulin sensitivity [9] (Fig. 1). As long as the product of insulin secretion times insulinsensitivity remains constant, glucose tolerance is preserved. For example, in a lean, insulinsensitive individual, less insulin secretion is required to maintain normal glucose levels. Anobese, insulin resistant individual requires a compensatory increase in insulin secretion in
order to maintain normal glucose levels. Inadequate β-cell compensation for insulinresistance results in impaired glucose homeostasis and eventually to T2DM. Longitudinalstudies have shown that reduced β-cell function as reflected in the disposition index is apowerful predictor of conversion from normal glucose tolerance to T2DM in at-riskpopulations [10, 11].
Multiple factors, including genetic predisposition, glucotoxicity, lipotoxicity, and decreasedβ-cell mass and function are thought to play a role in the pathogenesis of T2DM [2, 4]. Glucotoxicity and Lipotoxicity
Glucotoxicity refers to irreversible damage to pancreatic β cells caused by chronicallyelevated glucose levels and has been demonstrated with in vitro and in vivo studies [12–14]. Similarly to chronically elevated glucose levels, chronically elevated levels of free fattyacids (FFA) are known to cause β-cell dysfunction, a concept referred to as lipotoxicity [12]. Obesity, especially abdominal adiposity, results in increased FFA levels, and has beenshown to correlate with decreased insulin gene expression and β-cell death [12]. In vitro andin vivo studies using lipid infusions have shown that chronic exposure to FFA results indecreased glucose stimulated insulin secretion, decreased insulin gene expression, and
increased β-cell apoptosis in β cell lines and isolated human islets [15–17]. Recently, theconcept of “glucolipotoxicity” has been introduced because of evidence suggesting thatlipotoxicity is dependent on the simultaneous presence of hyperglycemia, and that elevatedglucose and FFA act synergistically to impair β-cell function [12, 15, 18].
Two proposed mechanisms for glucotoxicity are endoplasmic reticulum (ER) stress andoxidative stress [15, 19]. ER Stress
The ER is the organelle responsible for folding, modification, and trafficking of proteins[20]. β cells are particularly rich in ER, given their secretory function. ER stress occurswhen the ER’s folding capacity cannot match the protein load, and unfolded or misfoldedproteins accumulate in the ER’s lumen [12]. Chronic hyperglycemia increases theproduction demand on β cells, which puts them at risk for ER stress. As the β cells of
Curr Diab Rep. Author manuscript.
hyperglycemic individuals increase their preproinsulin production to account for elevatedglucose levels, misfolded proinsulin may result in ER stress [12].
It is important to note that the processing of proinsulin into mature insulin is a critical step ininsulin production and secretion, and high proinsulin levels relative to circulating levels ofmature insulin can indicate β-cell stress. Recent genome-wide association studies (GWAS)have identified 9 genetic variants associated with fasting proinsulin that may contribute to β-cell function and susceptibility for T2DM [21].
When ER stress occurs, a number of different stress responses collectively referred to as theunfolded protein response (UPR) are activated in an attempt to restore cell function [20]. This is accomplished by (a) decreased translation, (b) increased ER folding capacity, (c) ERstress associated protein degradation and, ultimately (d) cell apoptosis if a, b, and c areunsuccessful [12].
ER stress also results in increased production of molecular chaperones, which help withprotein folding, such as 78 kDa glucose-regulated protein (GRP78) and 4-phenylbutyrate(PBA) [19]. A recent study reported that glucose infusion to rats for 48 hours increased ERstress markers and induced β-cell dysfunction, but co-infusion with the chaperone moleculePBA prevented glucose-induced β-cell dysfunction [19]. Oxidative Stress
In vitro and in vivo studies implicate oxidative stress in glucose-induced β-cell dysfunction[19, 22, 23]. As glucose is metabolized in the mitochondria via oxidative phosphorylation,reactive oxygen species (ROS) are produced. As studies involving rat islets have shown,ROS reduce the ability of the mitochondria to produce ATP, thereby decreasing glucose-stimulated insulin secretion [24]. Isolated islets from T2DM patients have increased markersof oxidative stress compared with islets from controls without T2DM, and levels ofoxidative stress correlate with the degree of impairment in glucose-stimulated insulinsecretion [23]. Moreover, exposure to the antioxidant, glutathione, for 24 hours was shownto significantly improve glucose-stimulated insulin release and resulted in decreasedmarkers of oxidative stress suggesting that reducing islet cell oxidative stress may improvethe functional impairment of T2DM islets [23]. Reduced β-Cell Mass
A number of studies have demonstrated that β-cell mass and/or volume is reduced inpatients with T2DM [25–29]. In a study examining pancreatic tissue from 124 autopsies,relative β-cell volume was found to be increased by 50 % in obese individuals without
T2DM when compared with lean individuals without T2DM. In contrast, in obeseindividuals with impaired fasting glucose (IFG) there was a 40 % deficit in β-cell volumeand in obese individuals with T2DM there was a 63 % deficit in β-cell volume whencompared with obese individuals without T2DM [27]. The presence of decreased β-cellvolume in individuals with IFG suggests that this process occurs early on in the process ofdeveloping T2DM [27]. Effects of Type 2 Diabetes Therapies on β-Cell Function
Clinical management of T2DM is currently based on achieving plasma glucose levels thatare associated with a low risk of developing long-term microvascular complications [30]. There are a number of therapies that are effective in reducing plasma glucose levels throughvarious mechanisms, however current therapeutic strategies have different effects on β-cellfunction. Interventions that reduce the load on β-cells by decreasing insulin demand havebetter durability on glycemic control and are more effective in preventing T2DM in high
Curr Diab Rep. Author manuscript.
risk patients. Below, we discuss current therapies used in the treatment of T2DM and theireffects on β-cell function, long-term durability, and effectiveness in preventing progression
Intensive Lifestyle Modification
Obesity is a major risk factor for T2DM, and the increased prevalence of obesity is largelyresponsible for the concomitant increase in T2DM [1]. Obesity and lack of physical activitycause insulin resistance and increase the workload on β cells [31]. Weight loss and exerciseinterventions increase insulin sensitivity and unload the secretory demand on β-cells.
The United States Diabetes Prevention Program (DPP) showed that implementing a programthat achieved at least a 7 % reduction in body weight through diet and exercise reduced theincidence of T2DM by 58 % in patients with impaired glucose tolerance (IGT) [32]. Theeffect of lifestyle intervention on reducing the incidence of T2DM was related to overallimprovements in β-cell function driven by its gains in insulin sensitivity, such that thehyperbola describing the relationship between insulin secretion and in insulin sensitivity wasshifted to the right [33]. The Finnish Diabetes Prevention Study (DPS) also showed a 58 %reduction in the incidence of T2DM in individuals with IGT who were assigned to a lifestyleintervention that included weight loss and increased physical activity [34] (Table 1). Arecent analysis of the DPS indicated that lifestyle intervention helps to preserve β-cell
function and prevent the development of T2DM through improvements in insulin sensitivity[35]. Pharmacological Weight Loss
The Xenical in the Prevention of Diabetes in Obese Subjects (XENDOS) Study reported thatorlistat, a gastrointestinal lipase inhibitor, added to lifestyle intervention resulted in greaterweight loss and a 37 % reduced relative risk for diabetes compared with lifestyleintervention alone in obese adults with normal and impaired glucose tolerance [36]. In obesesubjects with IGT at baseline, orlistat plus lifestyle intervention resulted in a 45 % reducedrelative risk for diabetes vs lifestyle intervention alone (Table 1).
These randomized controlled trials demonstrate the importance of lifestyle modificationsand pharmacological weight loss in T2DM prevention, but it is important to note that weightregain is common [37], even with pharmacological treatment. For example, in the XENDOStrial, mean weight loss after the first year of treatment was 10.6 kg with orlistat plus lifestyleintervention and 6.2 kg after lifestyle intervention alone, but after 4 years of treatment themean weight loss was only 5.8 kg in orlistat plus lifestyle and 3.0 kg in lifestyle interventionalone [36]. Therefore, early intervention measures, including public health initiatives aimed
at preventing obesity by promoting physical activity and healthier diets early in life may beparticularly important to prevent the upward trends in prevalence of T2DM. For obeseindividuals with impaired glucose levels, interventions aimed at more robust and sustainedweight loss, including modestly invasive bariatric surgery, deserve exploration as anapproach towards β-cell preservation for the prevention of T2DM [38] (see “On theHorizon; Newer Approaches” below). Sulfonylureas
Sulfonylureas are oral medications that stimulate insulin secretion by binding to thesulfonylurea receptor 1, resulting in membrane depolarization and calcium influx, whichtriggers exocytosis of insulin containing secretory granules [39]. While sulfonylureas arewidely used clinically in the treatment of T2DM, evidence from the Diabetes OutcomeProgression Trial (ADOPT) study demonstrates a more rapid deterioration of glycemiccontrol with the sulfonylurea, glyburide, compared with treatment with metformin and the
Curr Diab Rep. Author manuscript.
thiazolidinedione (TZD), rosiglitazone in patients with recently diagnosed T2DM [40]. Invitro studies have suggested that the lack of durability of sulfonylurea treatment observed in
clinical studies may be due to its potentially damaging effects on pancreatic β-cells [41, 42]. Studies in isolated human islets indicate that the sulfonylurea, glibenclamide, decreasesinsulin content, and induces β-cell apoptosis [41, 42]; however, 1 study suggested that thesulfonylurea, gliclazide, may protect β cells from apoptosis potentially through antioxidanteffects [42]. No clinical studies have demonstrated a beneficial effect of sulfonylureas in theprevention of T2DM, and as mentioned above, sulfonylurea monotherapy has less durableeffects on glycemic control compared with a TZD or metformin in patients recentlydiagnosed with T2DM [40]. Metformin
Metformin is effective at reducing hyperglycemia primarily by inhibiting hepatic glucoseproduction and by increasing insulin sensitivity [43]. It is currently recommended as a first-line drug for the treatment of T2DM [30]. In vitro studies demonstrated that metformincould protect isolated human islets from glucotoxicity and lipotoxicity suggesting thatmetformin may have beneficial effects on β-cell health [44, 45]. In clinical studies, the DPPshowed that metformin reduced the conversion from IGT to T2DM by 31 % [32] suggestingthat it has modest effects on slowing the progression of T2DM (Table 1). The U.K. Prospective Diabetes Study (UKPDS) showed similar rates of deterioration of β-cell
function (assessed with HOMA-B index) and loss of glycemic control with metformintreatment compared with sulfonylureas or insulin treatment in patients with recentlydiagnosed T2DM [46, 47]. The ADOPT study showed that the durability of metforminmonotherapy was better than glyburide, but it still resulted in a 21 % failure rate at 5 years inpatients with recently diagnosed T2DM [40]. Acarbose
Acarbose is an α-glucosidase inhibitor that improves post-prandial hyperglycemia byinhibiting the activity of enzymes in the small intestine resulting in reduced glucoseabsorption. The Study to Prevent NIDDM (STOP-NIDDM) found a 25 % relative riskreduction in the development of T2DM over 3.3 years in patients with impaired glucoselevels treated with acarbose compared with placebo [48] (Table 1). However, in the 3-monthobservation period after acarbose was discontinued, the incidence of diabetes in patientswho had not converted was higher in the group initially assigned to acarbose (15 %)compared with group first randomized to placebo (10 %) suggesting that the benefit ofacarbose is lost after discontinuation of active treatment [48]. Thiazolidinediones (TZDs)
TZDs are potent insulin sensitizers that improve glycemic control in patients with T2DM[43, 49]. TZDs are ligands for the nuclear transcription factor peroxisome-proliferator-activated-receptor-γ, and they have a wide spectrum of action [49]. Studies have shown thatTZDs reduce lipotoxicity [50, 51], prevent β-cell apoptosis [52], increase serum adiponectinlevels [53], and improve β-cell function [54–57]. Prevention trials have consistently shownthat TZDs are effective in preventing the onset of type 2 diabetes in high-risk patients by~50 %–75 % (DPP, Troglitazone in Prevention of Diabetes (TRIPOD), Pioglitazone inPrevention of Diabetes (PIPOD), Diabetes Reduction Assessment with Ramipril andRosiglitazone Medication (DREAM), and Actos now (ACT-NOW) [55, 56, 58–60] (seeTable 1). The TRIPOD study was the first to carefully examine changes in β-cell functionthrough treatment of insulin resistance as a way to reduce T2DM risk. Notably, the TRIPODstudy showed that protection from diabetes in women with previous gestational diabetespersisted 8 months after T2DM treatment stopped, and patients who were protected fromdiabetes during TZD treatment had stable β-cell function and insulin resistance for almost 5
Curr Diab Rep. Author manuscript.
years demonstrating that TZDs slow the natural progression of the disease [55, 56]. Theability of TZDs to slow or stop progression to T2DM was supported by DREAM and DPP,
in which the protection from diabetes that was achieved during treatment persisted aftertreatment was stopped [61].
The ADOPT Study demonstrated that TZDs had significantly greater durability for glycemiccontrol in patients with recently diagnosed T2DM when compared with both metformin andsulfonylureas [40]. Subsequent analysis of the ADOPT data showed that the reduction intreatment failure with rosiglitazone corresponded with improved β-cell function andincreased insulin sensitivity [62] supporting results from the TRIPOD prevention study andsuggesting that TZDs may preserve β-cell function by improving insulin sensitivity andunloading the secretory demand on β-cells [55].
The clinical use of TZDs for the prevention of T2DM is limited due to adverse side effects,including fluid retention and weight gain, and recent safety concerns including reports of anassociation with increased risk for bone fractures and bladder cancer [49] The developmentof safer compounds with selective PPARγ modulation offers the potential for targetedinsulin sensitization in the absence of adverse side effects [49]. GLP-1 Receptor Agonists
Glucagon-like polypeptide-1 (GLP-1) is an incretin hormone secreted by the L cells in theintestines in response to nutrient stimulation. GLP-1 possesses a number of properties thatmake it an ideal agent for the treatment of T2DM. GLP-1 potentiates glucose stimulatedinsulin secretion, suppresses glucagon secretion, delays gastric emptying and suppressesappetite [43]. GLP-1 is cleaved by the enzyme dipeptidyl peptidase-4 (DPP-4) leading to itsrapid inactivation, but DPP-4 resistant GLP-1 receptor agonists, including exenatide andliraglutide, and DPP-4 inhibitors have been developed for the treatment of T2DM [43]. Studies in animals have shown the GLP-1 analogues decrease β-cell apoptosis and increaseβ-cell mass [63–65], and human studies indicate that exenatide exerts potent anti-inflammatory effects that are independent of weight loss [66]. Findings from recentrandomized controlled trials demonstrate that exenatide improves β-cell function [67, 68,69•, 70••]. Bunck and colleagues compared the effects of exenatide with the insulin,glargine, on β-cell function over 3 years in metformin treated patients with T2DM [68, 69•]. They found that exenatide significantly improved β-cell function during 52 weeks of activetreatment compared with glargine, but after stopping the treatments for 4 weeks, β-cellfunction returned to pre-treatment values in both groups [68]. In contrast, in the 3-yearextension study, β-cell function was sustained in the exenatide group after a 4-week off-drugperiod whereas the glargine treated patients had a reduction in β-cell function suggesting
that at least 3 years of exenatide treatment may be necessary to delineate a significant,prolonged benefit on β-cell function [69•].
A recent study in obese adults showed that a 20-week treatment with liraglutide (in dosesranging from 1.8 to 3 mg per day) resulted in greater weight loss and an 84 %–96 %reduction in the prevalence of prediabetes compared with placebo [71••]. Another clinicaltrial showed that a 24-week treatment with exenatide plus lifestyle modification resulted ingreater weight loss and normalization of glucose tolerance in 77 % of obese participantswith impaired glucose homeostasis (IGT or IFG) compared with 56 % in the placebo group[72•]. Longer term prevention trials in high-risk patients are needed to determine whetherGLP-1 agonists can modify the progressive course of T2DM.
A recent randomized controlled trial suggested that the GLP-1 receptor agonist, exenatide,may have durable effects on glycemic control in patients with T2DM [70••]. The EUREXAstudy compared exenatide with glimepiride as add-on to metformin for durability of
Curr Diab Rep. Author manuscript.
glycemic control in patients with T2DM who were inadequately controlled with metforminalone [70••]. Results showed that glycemic control was maintained for longer (180 weeks
with exenatide vs 142 weeks with glimepiride) and treatment failure was lower in theexenatide (41 %) compared with glimepiride (54 %) group over the 48 month follow upperiod. The exenatide group also had a significantly greater increase in disposition indexcompared with the glimepiride group demonstrating beneficial effects of exenatide on β-cellfunction [70••]. On the Horizon; Newer Approaches Early Intensive Treatment with Insulin and/or Multiple Agents
In vitro studies investigating the effects of glucose toxicity on a pancreatic β-cell lineshowed that shortening the duration of antecedent glucose toxicity increases the likelihoodof recovering β-cell function [73]. Thus, early and more aggressive treatment strategies thatquickly normalize glucose levels in patients with newly diagnosed T2DM may preserveresidual β-cell function by reducing glucotoxicity. Clinical studies have shown beneficialeffects of early short-term (2–3 weeks) intensive insulin therapy in patients with newlydiagnosed T2DM [74–78]. A multi-center randomized trial showed that early, short-termintensive insulin treatment at the time of T2DM diagnosis led to improved β-cell functionand greater diabetes remission rates at 1 year compared with early, short-term treatment with
oral hypoglycemic agents [75]. A recent randomized control trial evaluated β-cell functionpreservation after 3.5 years of intensive therapy with insulin plus metformin compared withtriple oral therapy with metformin, glyburide, and pioglitazone after an initial 3-monthinsulin treatment period and found that both approaches were effective in preserving β-cellfunction [77]. Based on these results, the authors suggested that patients with newlydiagnosed T2DM should be treated with an initial period of intensive insulin therapy tomaximize β-cell recovery and then continued either on insulin therapy or switched to acombination of oral agents with complementary mechanisms of action [77].
The Outcome Reduction with an Initial Glargine Intervention (ORIGIN) trial recentlyreported results of the comparison between treatment with insulin glargine to normalizefasting plasma glucose levels compared with standard care on cardiovascular outcomes,cancer, and incident diabetes in over 12,000 patients with cardiovascular disease risk factorsplus IFG or T2DM who were followed for a median of 6.2 years [79]. They found thatglargine had a neutral effect on cardiovascular outcomes and cancers, but that it reducednew-onset diabetes among the participants without diabetes at randomization providingsupport for the idea that the early use of insulin may preserve β-cell function in patients withimpaired glucose homeostasis.
There is a growing interest in the early use of combination therapies for the treatment ofpatients with IGT and T2DM [67, 80]. A recent clinical study examined the effects ofcombination therapy with exenatide and rosiglitazone vs each therapy alone on insulinsensitivity and β-cell function in patients with T2DM already on metformin [67]. The 20-week combination therapy with exenatide and rosiglitazone resulted in greaterimprovements in insulin sensitivity and β-cell function and better glycemic controlcompared with either treatment alone suggesting a beneficial effect of the combinationtherapy [67]. However, randomized controlled studies are needed to determine whether earlyuse of a combination of oral agents is effective in preventing T2DM in high risk patients andthe long-term durability of this treatment strategy on glycemic control. Bariatric Surgery
Bariatric surgery is an effective and durable treatment for obesity and provides substantialimprovements in glycemic control in obese patients with T2DM [81]. Four bariatric surgical
Curr Diab Rep. Author manuscript.
procedures are used conventionally, including Roux-en-Y gastric bypass (RYGB),laparoscopic adjustable gastric banding (LAGB), biliopancreatic diversion (BPD), and
laparoscopic sleeve gastrectomy (LSG), and RYGB and LAGB are the most widely usedsurgical procedures [81]. A meta-analysis indicated that bariatric surgery results inresolution of diabetes in 78 % of patients with T2DM demonstrating its significant impacton T2DM remission [82]. The effects of bariatric surgery on β-cell function were recentlysummarized in a review by Bradley et al [83], and indicate that LAGB surgery increases thedisposition index following modest weight loss, RYGB surgery increases the dispositionindex after significant weight loss, BPD surgery increases early insulin secretion anddisposition index in patients with T2DM, and LSG surgery increases early insulin secretionin patients with T2DM, but its effects on disposition index are currently unknown [83].
Three randomized controlled trials have compared the effects of bariatric surgery to medicaltherapy on remission of T2DM, and all 3 studies showed that bariatric surgery wassignificantly more effective than medical therapy in achieving remission of T2DM within 1to 2 years following surgery [84, 85••, 86••]. The first randomized controlled trial showedthat LAGB surgery resulted in T2DM remission in 73 % of patients vs only 13 % whoreceived standard medical treatment [84]. In a recent randomized controlled trial, 42 % ofobese patients with T2DM who underwent RYGB surgery and 37 % of those whounderwent LSG surgery achieved remission of T2DM compared with 12 % of patients
treated with conventional medical therapy [85••]. In another recent randomized controlledtrial, 95 % of individuals with T2DM who underwent BPD and 75 % of those whounderwent RYGB surgery, but none of those who received standard medical therapyachieved remission of T2DM [86••].
The long- term effects of bariatric surgery on T2DM remission were examined in theSwedish Obese Subjects Study (SOS), a nonrandomized prospective case-control study inover 4,000 obese patients who underwent bariatric surgery [87]. They found that 72 % ofT2DM patients achieved remission at 2 years after surgery, and 36 % had maintained T2DMremission at 10 years after surgery [87]. Similar results were found in another smaller studywhich showed durable remission of T2DM (>5 years) in over half of the 89 % of patientswho had achieved early following RYBG remission [88], and a meta-analysis whichreported that 62 % of patients with T2DM remained free of diabetes for more than 2 yearsfollowing bariatric surgery [82].
The effect of bariatric surgery (LAGB, VBG, RYGB) on the prevention of T2DM in obeseadults was recently examined in the SOS study which followed surgically treated andmatched controls for 15 years [89••]. Bariatric surgery compared with standard care reduced
the long-term relative risk of T2DM by 78 % in obese adults, and among those with IFG itreduced the relative risk of T2DM by 82 %. The postoperative mortality was 0.2 %, and 2.8% of patients had complications that required a reoperation [89••]. These findings indicatethat bariatric surgery has effective and durable effects on the prevention of T2DM in obeseadults, particularly among those with IFG. Randomized controlled trials are needed toconfirm whether bariatric surgery is an effective and safe approach for preventing T2DM inhigh-risk individuals. Conclusions
T2DM is characterized by a progressive loss of β-cell function that occurs against abackground of chronic insulin resistance. The rapid rise in rates of T2DM echoes a similarrise in rates of obesity, which causes insulin resistance and may have additional effects on β-cell health. Interventions that reduce body fat (such as diet and exercise, GLP-1 receptoragonists, or bariatric surgery) or that change fat biology (TZDs) provide the best evidence
Curr Diab Rep. Author manuscript.
for slowing or arresting the deterioration of β-cell function that causes T2DM. Theseinterventions should form the basis of interventions to prevent and treat T2DM, particularly
References
Papers of particular interest that have been published recently have been highlighted as:
1. Chen L, Magliano DJ, Zimmet PZ. The worldwide epidemiology of type 2 diabetes mellitus–present
and future perspectives. Nat Rev Endocrinol. 2012; 8:228–36.
2. Ashcroft FM, Rorsman P. Diabetes mellitus and the beta cell: the last ten years. Cell. 2012;
3. Buchanan TA. Pancreatic beta-cell loss and preservation in type 2 diabetes. Clin Ther. 2003;
4. Kahn SE. The relative contributions of insulin resistance and beta-cell dysfunction to the
pathophysiology of Type 2 diabetes. Diabetologia. 2003; 46:3–19. [PubMed: 12637977]
5. Abdul-Ghani MA, Tripathy D, DeFronzo RA. Contributions of beta-cell dysfunction and insulin
resistance to the pathogenesis of impaired glucose tolerance and impaired fasting glucose. DiabetesCare. 2006; 29:1130–9. [PubMed: 16644654]
6. Buchanan TA, Xiang AH, Peters RK, Kjos SL, Berkowitz K, Marroquin A, et al. Response of
pancreatic beta-cells to improved insulin sensitivity in women at high risk for type 2 diabetes. Diabetes. 2000; 49:782–8. [PubMed: 10905487]
7. Bergman RN, Ader M, Huecking K, Van Citters G. Accurate assessment of beta-cell function: the
hyperbolic correction. Diabetes. 2002; 51 (Suppl 1):S212–20. [PubMed: 11815482]
8. Porte D Jr, Kahn SE. beta-cell dysfunction and failure in type 2 diabetes: potential mechanisms.
Diabetes. 2001; 50 (Suppl 1):S160–3. [PubMed: 11272181]
9. Bergman RN, Phillips LS, Cobelli C. Physiologic evaluation of factors controlling glucose tolerance
in man: measurement of insulin sensitivity and beta-cell glucose sensitivity from the response tointravenous glucose. J Clin Invest. 1981; 68:1456–67. [PubMed: 7033284]
10. Weyer C, Hanson RL, Tataranni PA, Bogardus C, Pratley RE. A high fasting plasma insulin
concentration predicts type 2 diabetes independent of insulin resistance: evidence for a pathogenicrole of relative hyperinsulinemia. Diabetes. 2000; 49:2094–101. [PubMed: 11118012]
11. Lyssenko V, Almgren P, Anevski D, Perfekt R, Lahti K, Nissen M, et al. Predictors of and
longitudinal changes in insulin sensitivity and secretion preceding onset of type 2 diabetes. Diabetes. 2005; 54:166–74. [PubMed: 15616025]
12. Kim MK, Kim HS, Lee IK, Park KG. Endoplasmic reticulum stress and insulin biosynthesis: a
review. Exp Diabetes Res. 2012; 2012:509437. [PubMed: 22474424]
13. Bonner-Weir S, Trent DF, Weir GC. Partial pancreatectomy in the rat and subsequent defect in
glucose-induced insulin release. J Clin Invest. 1983; 71:1544–53. [PubMed: 6134752]
14. Leahy JL, Bonner-Weir S, Weir GC. Beta-cell dysfunction induced by chronic hyperglycemia.
Current ideas on mechanism of impaired glucose-induced insulin secretion. Diabetes Care. 1992;15:442–55. [PubMed: 1559411]
15. Poitout V, Robertson RP. Glucolipotoxicity: fuel excess and beta-cell dysfunction. Endocr Rev.
16. Lupi R, Dotta F, Marselli L, Del Guerra S, Masini M, Santangelo C, et al. Prolonged exposure to
free fatty acids has cytostatic and pro-apoptotic effects on human pancreatic islets: evidence thatbeta-cell death is caspase mediated, partially dependent on ceramide pathway, and Bcl-2 regulated. Diabetes. 2002; 51:1437–42. [PubMed: 11978640]
Curr Diab Rep. Author manuscript.
17. Oprescu AI, Bikopoulos G, Naassan A, Allister EM, Tang C, Park E, et al. Free fatty acid-induced
reduction in glucose-stimulated insulin secretion: evidence for a role of oxidative stress in vitroand in vivo. Diabetes. 2007; 56:2927–37. [PubMed: 17717282]
18. Prentki M, Joly E, El-Assaad W, Roduit R. Malonyl-CoA signaling, lipid partitioning, and
glucolipotoxicity: role in beta-cell adaptation and failure in the etiology of diabetes. Diabetes. 2002; 51 (Suppl 3):S405–13. [PubMed: 12475783]
19. Tang C, Koulajian K, Schuiki I, Zhang L, Desai T, Ivovic A, et al. Glucose-induced beta cell
dysfunction in vivo in rats: link between oxidative stress and endoplasmic reticulum stress. Diabetologia. 2012; 55:1366–79. [PubMed: 22396011]
20. Back SH, Kaufman RJ. Endoplasmic reticulum stress and type 2 diabetes. Annu Rev Biochem.
21. Strawbridge RJ, Dupuis J, Prokopenko I, Barker A, Ahlqvist E, Rybin D, et al. Genome-wide
association identifies nine common variants associated with fasting proinsulin levels and providesnew insights into the pathophysiology of type 2 diabetes. Diabetes. 2011; 60:2624–34. [PubMed:21873549]
22. Robertson RP. Chronic oxidative stress as a central mechanism for glucose toxicity in pancreatic
islet beta cells in diabetes. J Biol Chem. 2004; 279:42351–4. [PubMed: 15258147]
23. Del Guerra S, Lupi R, Marselli L, Masini M, Bugliani M, Sbrana S, et al. Functional and molecular
defects of pancreatic islets in human type 2 diabetes. Diabetes. 2005; 54:727–35. [PubMed:15734849]
24. Li N, Brun T, Cnop M, Cunha DA, Eizirik DL, Maechler P. Transient oxidative stress damages
mitochondrial machinery inducing persistent beta-cell dysfunction. J Biol Chem. 2009;284:23602–12. [PubMed: 19546218]
25. Sakuraba H, Mizukami H, Yagihashi N, Wada R, Hanyu C, Yagihashi S. Reduced beta-cell mass
and expression of oxidative stress-related DNA damage in the islet of Japanese Type II diabeticpatients. Diabetologia. 2002; 45:85–96. [PubMed: 11845227]
26. Yoon KH, Ko SH, Cho JH, Lee JM, Ahn YB, Song KH, et al. Selective beta-cell loss and alpha-
cell expansion in patients with type 2 diabetes mellitus in Korea. J Clin Endocrinol Metab. 2003;88:2300–8. [PubMed: 12727989]
27. Butler AE, Janson J, Bonner-Weir S, Ritzel R, Rizza RA, Butler PC. Beta-cell deficit and
increased beta-cell apoptosis in humans with type 2 diabetes. Diabetes. 2003; 52:102–10. [PubMed: 12502499]
28. Marchetti P, Del Guerra S, Marselli L, Lupi R, Masini M, Pollera M, et al. Pancreatic islets from
type 2 diabetic patients have functional defects and increased apoptosis that are ameliorated bymetformin. J Clin Endocrinol Metab. 2004; 89:5535–41. [PubMed: 15531508]
29. Ritzel RA, Butler AE, Rizza RA, Veldhuis JD, Butler PC. Relationship between beta-cell mass and
fasting blood glucose concentration in humans. Diabetes Care. 2006; 29:717–8. [PubMed:16505537]
30. Standards of medical care in diabetes-2011. Diabetes Care. 2011; 34(Suppl 1):S11–61. [PubMed:
31. Bergman RN. Minimal model: perspective from 2005. Horm Res. 2005; 64 (Suppl 3):8–15.
32. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al.
Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl JMed. 2002; 346:393–403. [PubMed: 11832527]
33. Kitabchi AE, Temprosa M, Knowler WC, Kahn SE, Fowler SE, Haffner SM, et al. Role of insulin
secretion and sensitivity in the evolution of type 2 diabetes in the diabetes prevention program:effects of lifestyle intervention and metformin. Diabetes. 2005; 54:2404–14. [PubMed: 16046308]
34. Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-Parikka P, et al.
Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impairedglucose tolerance. N Engl J Med. 2001; 344:1343–50. [PubMed: 11333990]
35. de Mello VD, Lindstrom J, Eriksson J, Ilanne-Parikka P, Keinanen-Kiukaanniemi S, Sundvall J, et
al. Insulin secretion and its determinants in the progression of impaired glucose tolerance to type 2
Curr Diab Rep. Author manuscript.
diabetes in impaired glucose-tolerant individuals: the Finnish Diabetes Prevention Study. DiabetesCare. 2012; 35:211–7. [PubMed: 22210578]
36. Torgerson JS, Hauptman J, Boldrin MN, Sjostrom L. XENical in the prevention of diabetes in
obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changesfor the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004; 27:155–61. [PubMed:14693982]
37. Venditti EM, Bray GA, Carrion-Petersen ML, Delahanty LM, Edelstein SL, Hamman RF, et al.
First versus repeat treatment with a lifestyle intervention program: attendance and weight lossoutcomes. Int J Obes (Lond). 2008; 32:1537–44.
38. Buchanan TA. Stemming the tide of type 2 diabetes: bring on the “big guns”. Obesity (Silver
39. Lang V, Youssef N, Light PE. The molecular genetics of sulfonyl-urea receptors in the
pathogenesis and treatment of insulin secretory disorders and type 2 diabetes. Curr Diab Rep. 2011; 11:543–51. [PubMed: 21968738]
40. Kahn SE, Haffner SM, Heise MA, Herman WH, Holman RR, Jones NP, et al. Glycemic durability
of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006; 355:2427–43. [PubMed: 17145742]
41. Maedler K, Carr RD, Bosco D, Zuellig RA, Berney T, Donath MY. Sulfonylurea induced beta-cell
apoptosis in cultured human islets. J Clin Endocrinol Metab. 2005; 90:501–6. [PubMed:15483097]
42. Del Guerra S, Marselli L, Lupi R, Boggi U, Mosca F, Benzi L, et al. Effects of prolonged in vitro
exposure to sulphonylureas on the function and survival of human islets. J DiabetesComplications. 2005; 19:60–4. [PubMed: 15642492]
43. Tahrani AA, Bailey CJ, Del Prato S, Barnett AH. Management of type 2 diabetes: new and future
developments in treatment. Lancet. 2011; 378:182–97. [PubMed: 21705062]
44. Lupi R, Del Guerra S, Fierabracci V, Marselli L, Novelli M, Patane G, et al. Lipotoxicity in human
pancreatic islets and the protective effect of metformin. Diabetes. 2002; 51 (Suppl 1):S134–7. [PubMed: 11815472]
45. Patane G, Piro S, Rabuazzo AM, Anello M, Vigneri R, Purrello F. Metformin restores insulin
secretion altered by chronic exposure to free fatty acids or high glucose: a direct metformin effecton pancreatic beta-cells. Diabetes. 2000; 49:735–40. [PubMed: 10905481]
46. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with
sulphonylureas or insulin compared with conventional treatment and risk of complications inpatients with type 2 diabetes (UKPDS 33). Lancet. 1998; 352:837–53. [PubMed: 9742976]
47. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with
metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998; 352:854–65. [PubMed: 9742977]
48. Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, Laakso M. Acarbose for prevention of
type 2 diabetes mellitus: the STOP-NIDDM randomised trial. Lancet. 2002; 359:2072–7.
49. Cariou B, Charbonnel B, Staels B. Thiazolidinediones and PPARgamma agonists: time for a
reassessment. Trends in endocrinology and metabolism: TEM. 2012; 23:205–15. [PubMed:22513163]
50. Lupi R, Del Guerra S, Marselli L, Bugliani M, Boggi U, Mosca F, et al. Rosiglitazone prevents the
impairment of human islet function induced by fatty acids: evidence for a role of PPARgamma2 inthe modulation of insulin secretion. Am J Physiol Endocrinol Metab. 2004; 286:E560–7. [PubMed: 14625208]
51. Prieur X, Mok CY, Velagapudi VR, Nunez V, Fuentes L, Montaner D, et al. Differential lipid
partitioning between adipocytes and tissue macrophages modulates macrophage lipotoxicity andM2/M1 polarization in obese mice. Diabetes. 2011; 60:797–809. [PubMed: 21266330]
52. Akiyama M, Hatanaka M, Ohta Y, Ueda K, Yanai A, Uehara Y, et al. Increased insulin demand
promotes while pioglitazone prevents pancreatic beta cell apoptosis in Wfs1 knockout mice. Diabetologia. 2009; 52:653–63. [PubMed: 19190890]
Curr Diab Rep. Author manuscript.
53. Yu JG, Javorschi S, Hevener AL, Kruszynska YT, Norman RA, Sinha M, et al. The effect of
thiazolidinediones on plasma adiponectin levels in normal, obese, and type 2 diabetic subjects. Diabetes. 2002; 51:2968–74. [PubMed: 12351435]
54. Gastaldelli A, Ferrannini E, Miyazaki Y, Matsuda M, Mari A, DeFronzo RA. Thiazolidinediones
improve beta-cell function in type 2 diabetic patients. Am J Physiol Endocrinol Metab. 2007;292:E871–83. [PubMed: 17106061]
55. Buchanan TA, Xiang AH, Peters RK, Kjos SL, Marroquin A, Goico J, et al. Preservation of
pancreatic beta-cell function and prevention of type 2 diabetes by pharmacological treatment ofinsulin resistance in high-risk hispanic women. Diabetes. 2002; 51:2796–803. [PubMed:12196473]
56. Xiang AH, Peters RK, Kjos SL, Marroquin A, Goico J, Ochoa C, et al. Effect of pioglitazone on
pancreatic beta-cell function and diabetes risk in Hispanic women with prior gestational diabetes. Diabetes. 2006; 55:517–22. [PubMed: 16443789]
57. Hanley AJ, Zinman B, Sheridan P, Yusuf S, Gerstein HC. Effect of Rosiglitazone and Ramipril on
{beta}-cell function in people with impaired glucose tolerance or impaired fasting glucose: theDREAM trial. Diabetes Care. 2010; 33:608–13. [PubMed: 20009095]
58. Gerstein HC, Yusuf S, Bosch J, Pogue J, Sheridan P, Dinccag N, et al. Effect of rosiglitazone on
the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: arandomised controlled trial. Lancet. 2006; 368:1096–105. [PubMed: 16997664]
59. DeFronzo RA, Tripathy D, Schwenke DC, Banerji M, Bray GA, Buchanan TA, et al. Pioglitazone
for diabetes prevention in impaired glucose tolerance. N Engl J Med. 2011; 364:1104–15.
60. Knowler WC, Hamman RF, Edelstein SL, Barrett-Connor E, Ehrmann DA, Walker EA, et al.
Prevention of type 2 diabetes with troglitazone in the Diabetes Prevention Program. Diabetes. 2005; 54:1150–6. [PubMed: 15793255]
61. Buchanan TA. (How) can we prevent type 2 diabetes? Diabetes. 2007; 56:1502–7. [PubMed:
62. Kahn SE, Lachin JM, Zinman B, Haffner SM, Aftring RP, Paul G, et al. Effects of rosiglitazone,
glyburide, and metformin on beta-cell function and insulin sensitivity in ADOPT. Diabetes. 2011;60:1552–60. [PubMed: 21415383]
63. Rolin B, Larsen MO, Gotfredsen CF, Deacon CF, Carr RD, Wilken M, et al. The long-acting
GLP-1 derivative NN2211 ameliorates glycemia and increases beta-cell mass in diabetic mice. AmJ Physiol Endocrinol Metab. 2002; 283:E745–52. [PubMed: 12217892]
64. Drucker DJ. Glucagon-like peptide-1 and the islet beta-cell: augmentation of cell proliferation and
inhibition of apoptosis. Endocrinology. 2003; 144:5145–8. [PubMed: 14645210]
65. Li Y, Hansotia T, Yusta B, Ris F, Halban PA, Drucker DJ. Glucagon-like peptide-1 receptor
signaling modulates beta cell apoptosis. J Biol Chem. 2003; 278:471–8. [PubMed: 12409292]
66. Chaudhuri A, Ghanim H, Vora M, Sia CL, Korzeniewski K, Dhindsa S, et al. Exenatide exerts a
potent antiinflammatory effect. J Clin Endocrinol Metab. 2012; 97:198–207. [PubMed: 22013105]
67. DeFronzo RA, Triplitt C, Qu Y, Lewis MS, Maggs D, Glass LC. Effects of exenatide plus
rosiglitazone on beta-cell function and insulin sensitivity in subjects with type 2 diabetes onmetformin. Diabetes Care. 2010; 33:951–7. [PubMed: 20107105]
68. Bunck MC, Diamant M, Corner A, Eliasson B, Malloy JL, Shaginian RM, et al. One-year
treatment with exenatide improves beta-cell function, compared with insulin glargine, inmetformin-treated type 2 diabetic patients: a randomized, controlled trial. Diabetes Care. 2009;32:762–8. [PubMed: 19196887]
69•. Bunck MC, Corner A, Eliasson B, Heine RJ, Shaginian RM, Taskinen MR, et al. Effects of
exenatide on measures of beta-cell function after 3 years in metformin-treated patients with type2 diabetes. Diabetes Care. 2011; 34:2041–7. This randomized clinical trial showed that following3 years of treatment with exenatide, β-cell function was sustained after a 4-week off-drug periodsuggesting a benefical effect of exenatide on β-cell health in metformin-treated patients withT2DM. [PubMed: 21868779]
70••. Gallwitz B, Guzman J, Dotta F, Guerci B, Simo R, Basson BR, et al. Exenatide twice daily
versus glimepiride for prevention of glycaemic deterioration in patients with type 2 diabetes with
Curr Diab Rep. Author manuscript.
metformin failure (EUREXA): an open-label, randomised controlled trial. Lancet. 2012;379:2270–8. A large multicenter open label randomized controlled trial showing that exenatidehad more durable effects on glycemic control compared to glimepiride over a 48 month follow
up period in patients with T2DM inadequately controlled with metformin alone. [PubMed:22683137]
71••. Astrup A, Rossner S, Van Gaal L, Rissanen A, Niskanen L, Al Hakim M, et al. Effects of
liraglutide in the treatment of obesity: a randomised, double-blind, placebo-controlled study. Lancet. 2009; 374:1606–16. A large multicenter randomized controlled trial showing thattreatment with liraglutide resulted in signicantly greater weight loss and a reduction in theprevalence of prediabetes in obese adults. [PubMed: 19853906]
72•. Rosenstock J, Klaff LJ, Schwartz S, Northrup J, Holcombe JH, Wilhelm K, et al. Effects of
exenatide and lifestyle modification on body weight and glucose tolerance in obese subjects withand without pre-diabetes. Diabetes Care. 2010; 33:1173–5. Randomized trial showing that a 24-week treatment with exenatide plus lifestyle modification resulted in greater weight loss andnormalization of glucose tolerance in 77 % of obese participants with impaired glucosehomeostasis compared to 56 % in the placebo group. [PubMed: 20332357]
73. Gleason CE, Gonzalez M, Harmon JS, Robertson RP. Determinants of glucose toxicity and its
reversibility in the pancreatic islet beta-cell line, HIT-T15. Am J Physiol Endocrinol Metab. 2000;279:E997–1002. [PubMed: 11052953]
74. Ilkova H, Glaser B, Tunckale A, Bagriacik N, Cerasi E. Induction of long-term glycemic control in
newly diagnosed type 2 diabetic patients by transient intensive insulin treatment. Diabetes Care.
75. Weng J, Li Y, Xu W, Shi L, Zhang Q, Zhu D, et al. Effect of intensive insulin therapy on beta-cell
function and glycaemic control in patients with newly diagnosed type 2 diabetes: a multi-centrerandomised parallel-group trial. Lancet. 2008; 371:1753–60. [PubMed: 18502299]
76. Chen HS, Wu TE, Jap TS, Hsiao LC, Lee SH, Lin HD. Beneficial effects of insulin on glycemic
control and beta-cell function in newly diagnosed type 2 diabetes with severe hyperglycemia aftershort-term intensive insulin therapy. Diabetes Care. 2008; 31:1927–32. [PubMed: 18556343]
77. Harrison LB, Adams-Huet B, Raskin P, Lingvay I. beta-cell function preservation after 3.5 years of
intensive diabetes therapy. Diabetes Care. 2012; 35:1406–12. [PubMed: 22723578]
78. Hu Y, Li L, Xu Y, Yu T, Tong G, Huang H, et al. Short-term intensive therapy in newly diagnosed
type 2 diabetes partially restores both insulin sensitivity and beta-cell function in subjects withlong-term remission. Diabetes Care. 2011; 34:1848–53. [PubMed: 21680726]
79. Gerstein HC, Bosch J, Dagenais GR, Diaz R, Jung H, Maggioni AP, et al. Basal insulin and
cardiovascular and other outcomes in dysglycemia. N Engl J Med. 2012; 367:319–28. [PubMed:22686416]
80. DeFronzo RA, Abdul-Ghani MA. Preservation of beta-cell function: the key to diabetes
prevention. J Clin Endocrinol Metab. 2011; 96:2354–66. [PubMed: 21697254]
81. Dixon JB, le Roux CW, Rubino F, Zimmet P. Bariatric surgery for type 2 diabetes. Lancet. 2012;
82. Buchwald H, Estok R, Fahrbach K, Banel D, Jensen MD, Pories WJ, et al. Weight and type 2
diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009; 122:248–56e5. [PubMed: 19272486]
83. Bradley D, Magkos F, Klein S. Effects of bariatric surgery on glucose homeostasis and type 2
diabetes. Gastroenterology. 2012; 143:897–912. [PubMed: 22885332]
84. Dixon JB, O’Brien PE, Playfair J, Chapman L, Schachter LM, Skinner S, et al. Adjustable gastric
banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299:316–23. [PubMed: 18212316]
85••. Schauer PR, Kashyap SR, Wolski K, Brethauer SA, Kirwan JP, Pothier CE, et al. Bariatric
surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012;366:1567–76. Randomized controlled single center trial showing that RYGB surgery was moreeffective than intensive medical therapy in achieving remission of diabetes at 12 months offollow up in obese adults. [PubMed: 22449319]
Curr Diab Rep. Author manuscript.
86••. Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Leccesi L, et al. Bariatric
surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012; 366:1577–85.Randomized controlled single center trial that showed at 2 years of follow up diabetes
remission had occurred in no patients in the medical therapy group versus 75 % in the RYGBsurgery group and 95 % in the biliopancreatic-diversion group
87. Sjostrom L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B, et al. Lifestyle,
diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–93. [PubMed: 15616203]
88. Chikunguwo SM, Wolfe LG, Dodson P, Meador JG, Baugh N, Clore JN, et al. Analysis of factors
associated with durable remission of diabetes after Roux-en-Y gastric bypass. Surg Obes RelatDis. 2010; 6:254–9. [PubMed: 20303324]
89••. Carlsson LM, Peltonen M, Ahlin S, Anveden A, Bouchard C, Carlsson B, et al. Bariatric surgery
and prevention of type 2 diabetes in Swedish obese subjects. N Engl J Med. 2012; 367:695–704. Large prospective case–control study showing that bariatric surgery as compared to usual caresignificanlty reduced the incidence of diabetes in obese patients, particularly among obesepatients with impaired fasting glucose. [PubMed: 22913680]
Curr Diab Rep. Author manuscript. Fig 1. The Disposition Index (DI) is the product of insulin secretion and insulin sensitivity. Normally, increases in insulin resistance (due to factors such as weight gain and inactivity) are matched by a compensatory increase in insulin secretion in a hyperbolic relationship (A to B) and DI remains constant. Inadequate insulin secretion to compensate for insulin resistance results in a reduction in DI and impaired glucose homeostasis (A to C) and eventually to type 2 diabetes (A to D). (Data adapted from: Bergman RN, Phillips LS, Cobelli C. Physiologic evaluation of factors controlling glucose tolerance in man: measurement of insulin sensitivity and beta-cell glucose sensitivity from the response to intravenous glucose. J Clin Invest. 1981;68(6):1456–67) [9]. Curr Diab Rep. Author manuscript. Participants at high-risk for diabetes Intervention Relative reduction in risk of diabetesa DPP Diabetes Prevention Program, DPS Diabetes Prevention Study, TRIPOD troglitazone in prevention of diabetes, DREAM diabetes reductionassessment with ramipril and rosiglitazone medication, ACT NOW Actos now, IGT impaired glucose tolerance, GDM gestational diabetes mellitus
Curr Diab Rep. Author manuscript.
Gebrauchsinformation: Information für Patienten Telmicard 40 mg-Tabletten Lesen Sie die gesamte Packungsbeilage sorgfältig durch, bevor Sie mit der Einnahme dieses Arzneimittels beginnen, denn sie enthält wichtige Informationen. - Heben Sie die Packungsbeilage auf. Vielleicht möchten Sie diese später nochmals lesen. Wenn Sie weitere Fragen haben, wenden Sie sich an Ihren Ar
The Contraceptive Patch What is the contraceptive patch? The contraceptive patch (Ortho Evra™ transdermal system) is a weekly hormonal birth control method that you place on your skin like a large Band-Aid®. It is a thin, smooth, beige square that is about the size of a matchbook. The patch contains hormones that are released through the skin and into the bloodstream. How doe
 NIH Public Access
NIH Public Access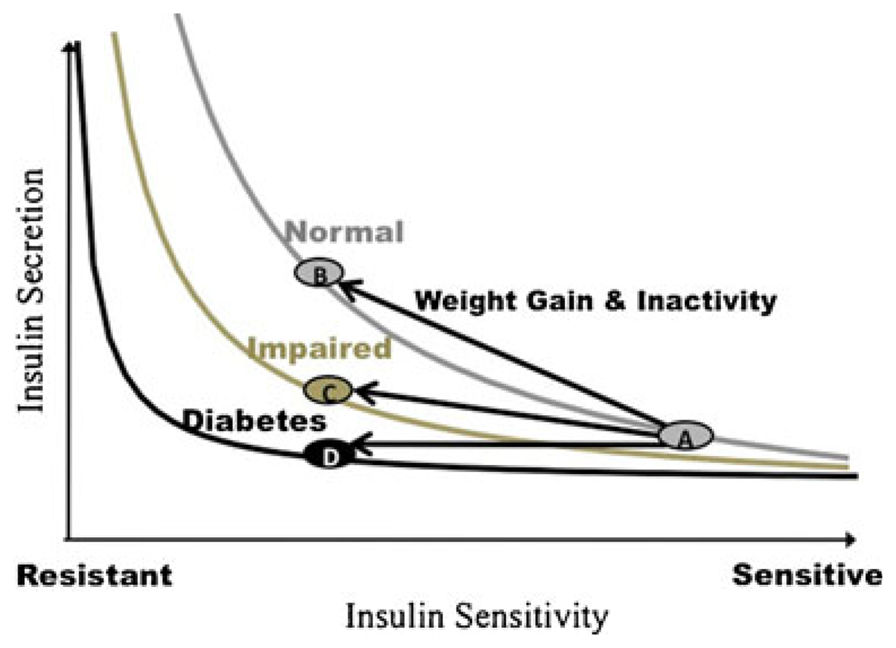 Fig 1.
Fig 1.