Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Layout
The Blood and Marrow Transplant Program at
Ohio State University Comprehensive Cancer Center -
James Cancer Hospital and Solove Research Institute
has recently been named as a Blue Distinction
Center for Transplantation of Adult Autologous and
Allogeneic hematopoietic cells. Previously we had
Steven M. Devine MD
only been awarded this distinction for recipients of
Director, Blood and Marrow Transplant Program Ohio State University Comprehensive Cancer Center –
Should you have a patient with medical coverage
James Cancer Hospital and Solove Research Institute
within the Blue Cross Network who may potentially
benefit from an allogeneic cell transplant, they may
New Trials Designed to Prevent
allogeneic transplantation is often a patient's best
(and sometimes only) treatment option, efforts to
Graft Versus Host Disease
reduce the risk of GVHD are of paramount impor-
tance to investigators in the field. The Ohio State
Despite overall improvements in the management
University Blood and Marrow Transplant (BMT)
of patients undergoing allogeneic blood or marrow
Program is currently involved in a number of studies
transplantation, acute graft versus host disease
(GVHD) remains the major complication of this
Our BMT Program has several ongoing or soon to
procedure and after relapse of the primary disease, is
be activated trials supported by The National
the most common cause of mortality associated with
Institutes of Health (NIH) designed in part to mitigate
transplantation. The risk of GVHD is related to the
GVHD. While most centers use pharmacological
degree of matching between donor and recipient and
agents like cyclosporine or tacrolimus to prevent
is higher following unrelated donor compared to
GVHD, T-cell depletion of the graft represents the
sibling donor transplantation. The risk rises as the
other end of the spectrum. This technique employs
donor and recipient are less well matched. Since
various physical or pharmacologic approaches to
I N T H I S I S S U E ▼ New Trials Designed to Prevent Graft OSU BMT and Myeloma Programs Blood Marrow Drives Versus Host Disease Offer Several Clinical Trials for Patients with Multiple Myeloma Patient Profile Blood and Marrow Stem Cell Transplant Program Advanced Practice Nurses
Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
New Trials Designed to Prevent Graft Versus Host Disease . . . continued on page 2)
remove the T-cells that cause GVHD from the graft
very well matched volunteer donor. In OSU 06042,
prior to transplantation. This is not a new approach
we will attempt to identify donors mismatched at the
but there are newer, more efficient methods now
HLA-C locus in order to stimulate the donors natural
available which are being evaluated. One of these
killer (NK) cells to elicit a graft versus leukemia
approaches is called positive selection. This approach
response, according to the results generated by the
uses immunoaffinity or immunomagnetic bead
transplant group in Perugia, Italy and recently updated
systems to separate the hematopoietic stem and
in The Journal of Clinical Oncology (Aversa et al,).
progenitor cells from the cells comprising the innate
This trial is being performed in collaboration with the
BMT Programs at The University of Minnesota
The approach most commonly taken uses immuno-
(UMinn), Emory University, and the Moffitt Cancer
magnetic beads containing antibodies to the CD34
Center and is funded by The National Cancer Institute
antigen which is expressed on the stem/progenitor
in conjunction with a Program Project Grant headed by
cells but not the T-cells. The beads bind to the stem
Dr. Jeffrey Miller at UMinn. Patients up to age 60
cells and are then passed through a magnetic field.
are eligible for this trial and are not required to be in
The stem/progenitor cells expressing CD34 are
retained within the magnetic field while the T/B, and
At the other end of the spectrum, we are using
NK cells are eluted away from them. This technique
novel agents to prevent GVHD. Based on encouraging
allows for a very efficient and relatively easy T-cell
preliminary data generated by the BMT team at Dana
depletion (up to 5 logs). A purified graft can then be
Farber Cancer Institute in which the combination of
transplanted into the recipient with little or no risk of
tacrolimus and sirolimus (rapamycin) has been
associated with very low risk of acute GVHD, BMT
In BMT CTN 0303, we are using this technique in
CTN 0402 is a phase III randomized clinical trial
patients with acute myeloid leukemia (AML) in first or
comparing the more standard approach using
second remission. The patients receive a relatively
tacrolimus and methotrexate to the combination of
strong conditioning regimen containing chemotherapy
tacrolimus and sirolimus. This trial is about to be
and radiation but the patients do not have to be given
opened at OSU as well as several BMT programs
any post-transplant immunosuppressive drugs. Thus,
throughout the United States. The trial is open to
the risk of mucositis and other complications is dimin-
patients with hematological malignancies undergoing
ished with this approach. The patients must be
myeloablative matched sibling donor transplantation.
between the ages of 18-60 years inclusive and have a
If shown to be superior, the tacrolimus/sirolimus
matched sibling donor available. This multi-center
combination would represent the first change in
trial is also open at The Memorial Sloan-Kettering and
standard GVHD prophylaxis in over 15 years.
Dana Farber Cancer Centers, among others. The other
The OSU BMT Program continues to expand its
T-cell depletion trial we have open involves patients
allogeneic transplant program primarily by combining
with AML, myelodysplastic syndrome, and advanced
excellent patient care with access to high quality
chronic myelogeneous leukemia who are in need of an
allogeneic transplant but who are unable to identify a
New BMT Information on Jamesline.com
Jamesline.com has added a new section about The James' Blood and Marrow Transplant program.
Patients now have access to extensive information about The James' comprehensive BMT program
including our patient care expertise, research and facilities.
You can access the new site by going to www.jamesline.com/go/bmt. OSU BMT and Myeloma Programs
to move standard risk patients not eligible for a
clinical trial on to autologous transplant followed by
Offer Several Clinical Trials for Patients with Multiple Myeloma The Ohio State Multiple Myeloma
At Ohio State, we have two active Cancer and
Clinical and Research Program
Leukemia Group B (CALGB) hematopoietic stem cell
(www.jamesline.com/cancertypes/multiple_myeloma)
transplant protocols available for myeloma patients.
is led by Craig Hofmeister M.D. and Don Benson M.D.
The first is a phase III trial evaluating the survival
Ph.D. In 2006, we performed 50 transplants for
advantage of using lenalidomide (RevlimidÍ) mainte-
myeloma and we see approximately 15 consultations per
nance after autologous transplant in patients with stable
month, most often in evaluation for hematopoietic stem
or responsive disease to induction therapy. The second
cell transplantation. OSU is an active member of CALGB
is a phase II trial investigating the efficacy of autologous
and the Multiple Myeloma Research Consortium
transplant followed by non-ablative HLA-identical
(MMRC). We have NCI/CTEP sponsored protocols with
sibling transplant in patients with no more than one prior
novel agents in myeloma as well as access to new drugs
progression after induction therapy.
through the MMRC. We are focused on accruing
We have also assembled an interesting array of
patients to trials that ask interesting questions with
clinical trials for patients with relapsed or refractory
multiple myeloma. We have five trials open for accrual:
1) A phase I trial evaluating the monoclonal antibody
We would like to work in partnership with you in the
1-7F9 that blocks the natural killer (NK) cell inhibitory
management of patients with this difficult disease.
KIR pathway and potentially activates NK cell killing of
If you would like to refer patients, please contact
myeloma cells; 2) A phase I trial evaluating the inhibitor
AVN-944 of the enzyme IMDPH involved in DNA
(614-293-7433, [email protected])
synthesis that promotes apoptosis of rapidly dividing
cells; 3) A phase I trial of the second generation
proteasome inhibitor NPI-0052; 4) A phase I trial of
(614-293-9165, [email protected])
Flavopiridol, a novel RNA polymerase inhibitor with
for non transplant referrals simply email
demonstrated efficacy in Chronic Lymphocytic Leukemia
(CLL); and 5) a dose-escalated phase I trial of
([email protected])
lenalidomide (RevlimidÍ) combined with a novel mTOR
Our partnership to support clinical trials that advance
inhibitor CCI-779 - both agents have activity in myeloma
the knowledge base in myeloma will ultimately prolong
as single agents, preclinically the combination has
synergistic activity, and this is one of the few steroid-free
As this goes to press, data will be emerging from the
Myeloma treatment sequence at Ohio State
American Society of Clinical Oncology 2007 meeting
that less steroid exposure prolongs survival in Multiple
Myeloma. Rajkumar et al. will present data showing
an improved survival and fewer toxicities using
upfront therapy with the combination of lenalidomide
(RevlimidÍ)at 25 mg daily days 1-21 and low dose
dexamethasone 40 mg weekly on days 1, 8, 15, 22 of a 28
day cycle compared to lenalidomide plus standard high
dose dexamethasone on days 1-4, 9-12, 17-20. We have
adopted this low dose dexamethasone strategy in our
upfront therapy since Jan-2007 (see table 1) and prefer
Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
Off protocol upfront therapy for multiple myeloma Risk stratification Prioritized treatments
Velcade days 1,4,8,11 + 40 mg Decadron weekly q21
Revlimid 25 mg days 1-21 + 40 mg Decadron weekly q28
Revlimid 25 mg days 1-21 + 40 mg Decadron weekly q28
Autologous stem cell transplant candidates:
Velcade days 1,4,8,11 + 40 mg Decadron weekly q21
Thalidomide 100 mg PO qHS continuous q42 days
Thalidomide 100 mg PO qHS + 40 mg Decadron weekly q28
Myeloma clinical trials available at Ohio State
[NCI] Phase I trial of Lenalidomide and CCI-779
Eligibility:
2. Bilirubin < 1.5xULN, Creatinine < 2 mg/dL
3. Must have >25% increase in M-protein after last therapy
4. Exposure to prior lenalidomide or CCI-779 OK, not both
[NCI] Phase I trial of Flavopiridol (RNA polymerase inhibitor)
Eligibility:
4. Bilirubin < 2 xULN, Creatinine < 2 mg/dL
Relapsed
[MMRC] Phase I of NPI-0052 (Proteasome inhibitor)
refractory Eligibility:
2. Hb > 8 g/dL, ANC > 1500, Platelets > 75K
3. Bilirubin < 1.5x ULN, Creatinine < 1.5xULN
Phase I trial of AVN-944 (IMDPH inhibitor)
Eligibility:
3. Bilirubin < 2 mg/dL, Creatinine < 2 mg/dL
Eligibility:
1. At least 2 months since last chemotherapy
2. Ability of patient NK cells to bind anti-KIR
3. Bilirubin < 1.5x ULN, Creatinine < 2 mg/dL Plan to open in Jun-2007
[CALGB] Autologous alone or with Revlimid maintenance
Eligibility:
1. Stable disease or responsive to 2+ mos. of any induction
2. No more than 12 mos. of any prior therapy, including Rev
3. No prior progression after initial therapy
Transplant
[CALGB] Auto- then non-myeloablative sibling transplant
Eligibility:
1. No more than 12 mos. alkylators, 18 mos. total treatment
2. No more than one prior progression after initial therapy
Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
PAT I E N T P R O F I L E : Joe Ogden
In 1996 Joe Ogden felt a lump in his groin and thought nothing of it, a short time later he received the
diagnosis of Non-Hodgkin's Lymphoma. After two different rounds of chemo and two years of remission the
Lymphoma returned. This time he needed a bone marrow transplant. His three sisters were not suitable
matches and after two years of waiting, somewhat patiently, Joe found a donor from the National Marrow
Donor Program. The transplant was successful, and then in April 2005 he discovered the cancer had once again
returned this time on his vocal chord. After several more rounds of chemo, it was determined he would again
need radiation and another bone marrow transplant. He received a second transplant from the same
anonymous donor. Putting him in remission again and hopefully for good.
Through all of this Joe never lost his positive attitude or his faith in his medical team. He attributes his
positive outlook to his family especially his grandson. Before cancer sidelined Joe he was an auctioneer, with
his cancer in remission he felt it was time to give back to the medical community that had helped him. Putting
his auctioneer skills to work in April 2006 he raised $10,000 for a bone marrow drive. So far the dollars he
raised have registered 100 people to the National Marrow Donor Program. This fall he hopes to register at least
100 more. Joe has one more thing to look forward to, this summer he hopes to finally find out who his donor
was. He thinks the least he should do is say thank you to the person that helped him not once but twice. Blood and Marrow Stem Cell Transplant Program
The nurse practitioners work in both the inpatient and
Advanced Practice Nurses
outpatient setting within the BMT program providing direct
patient care to persons undergoing transplantation.
The Blood and Marrow Transplant (BMT) program is
Each nurse practitioner collaborates with the physicians to
comprised of a multidisplinary team which includes
provide care to patients during the steps of pre-transplant
physicians, advanced practice nurses, a nurse manager,
evaluation, transplant process and post-transplant care.
a clinical nurse specialist, staff nurses, BMT patient
Each nurse practitioner is assigned to a specific physician
coordinators, research nurses, a pharmacist, a data
outpatient clinic and is able to follow the clinic patient
manager, social workers, patient care assistants, unit
through the transplant process. Responsibilities of the
clerical coordinators and many others. There are eight
nurse practitioner include obtaining an initial history and
advanced practice nurses known as nurse practitioners
physical, daily patient assessments, ordering and reviewing
who work with all of the members of the multidisciplinary
results of diagnostic tests and laboratory data, writing
team to provide care to persons undergoing a BMT.
prescriptions, assisting with the discharge planning
In addition to BMT, many areas of clinical expertise are
process, and ensuring the appropriate conduct of clinical
represented among the nurse practitioners including
research. The nurse practitioner also participates in
cancer care, symptom management, hospice, critical care,
ongoing patient and family education regarding the
family practice, case management, and teaching.
transplant process, adverse effects and complications of
transplant as well as symptom management.
The nurse practitioner collaborates with all members
of the BMT health care team to assist with the facilitation
of care through the transplant process. Patients may
meet many of the nurse practitioners, but one nurse
practitioner will be assigned to each patient to assist with
continuity of care. The role of the nurse practitioner in
BMT continues to evolve to assist in meeting the needs
of persons undergoing transplantation.
Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
Bone Marrow Drives
participation. Registration was held at the College of
Medicine and the OSU Student Union. Children's
Each year, more than 35, 000 children and adults in
Hospital held 3 sites throughout the city. The drive was
the United States develop life threatening diseases for
a great success with a total of 569 new volunteer donors
which a marrow or blood stem cell transplant could be
joining the Registry. Of the 569 donors, 49 were of a
a cure. Only 30 percent of patients in need of a stem
cell transplant find a matched donor in their family.
In addition, the Blood and Marrow Transplantation
The other 70 percent need to find an unrelated donor.
Program worked with the NMDP to hold it's own
That means, every day, thousands of patients are
Medical Center donor drive on September 29, 2006.
searching for a donor. The National Marrow Donor
We are please to report a total of 168 employees joined
Program® (NMDP) maintains a Registry of volunteer
the Registry. We encourage everyone to consider
donors that we can search. Over 6 million donors are
becoming a donor in the NMDP. You could be the one
registered with the NMDP and over 10 million donors
are registered worldwide. Sadly, we still encounter
Log onto MARROW.org for more information.
patients for whom we cannot find donors because they
have less common tissue traits. The most difficult
searches are for patients of minority races. Of the over
6 million donors in the Registry, only 1.6 million are of
minority or mixed races. The need to promote minority
The James, Ohio State University and Columbus
Children's Hospital worked in collaboration with the
NMDP to hold a bone marrow drive on November 2,
2006. The focus of the drive was to promote minority
Ohio State’s Comprehensive Cancer Center –
James Cancer Hospital and Solove Research Institute
POST-OPERATIVE INSTRUCTIONS FOR EAR SURGERY (Tympanoplasty, Mastoidectomy, ME explorations) What should be expected following EAR surgery? Please remember that your child has had surgery. Please do not allow them to participate in any heavy lifting, exercise or physical contact unless cleared by your surgeon. If they develop an upper respiratory infection, especially with coughin
“Intergenerational Occupational Mobility in Britain and the U.S. Since 1850” Abstract The U.S. both tolerates more inequality than Europe and believes its economicmobility is greater than Europe’s. These attitudes and beliefs help account fordifferences in the magnitude of redistribution through taxation and social welfarespending. In fact, the U.S. and Europe had roughly equal rates
 The Blood and Marrow Transplant Program at
Ohio State University Comprehensive Cancer Center -
James Cancer Hospital and Solove Research Institute
has recently been named as a Blue Distinction
Center for Transplantation of Adult Autologous and
Allogeneic hematopoietic cells. Previously we had
Steven M. Devine MD
The Blood and Marrow Transplant Program at
Ohio State University Comprehensive Cancer Center -
James Cancer Hospital and Solove Research Institute
has recently been named as a Blue Distinction
Center for Transplantation of Adult Autologous and
Allogeneic hematopoietic cells. Previously we had
Steven M. Devine MD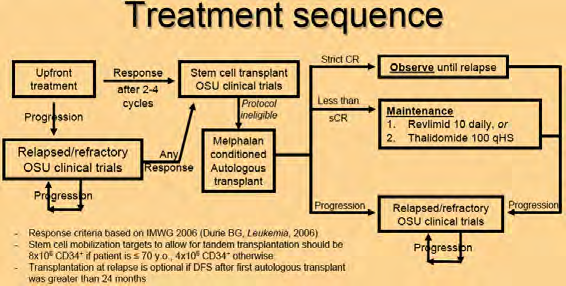 OSU BMT and Myeloma Programs
OSU BMT and Myeloma Programs Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
PAT I E N T P R O F I L E : Joe Ogden
Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
PAT I E N T P R O F I L E : Joe Ogden Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
Bone Marrow Drives
Blood and Marrow Transplant Update S U M M E R / FA L L 2 0 0 7
Bone Marrow Drives