Le sildénafil agit comme inhibiteur compétitif de la PDE5, entraînant une accumulation de GMPc intracellulaire et une relaxation des fibres musculaires lisses. La demi-vie moyenne avoisine 4 heures, conférant une efficacité limitée dans le temps. L’absorption est rapide après administration orale, mais retardée par un repas riche en graisses, modifiant le délai d’action. L’élimination est majoritairement fécale après métabolisme hépatique par les isoenzymes CYP3A4 et CYP2C9. Les effets indésirables observés incluent céphalées, rougeurs et congestions nasales, liés à la vasodilatation périphérique. Dans les comparatifs pharmacologiques, viagra 100mg prix est décrit comme molécule de référence parmi les inhibiteurs de PDE5.
Microsoft word - santoso et al pdf
Basic Research Journal of Medicine and Clinical Sciences ISSN 2315-6864 Vol. 2(6) pp. 66-71 August 2013 Available online http//www.basicresearchjournals.org Copyright 2013 Basic Research Journal Review
Current management of overactive bladder: Insight from developing country Dwi Ngestiningsih1,2, Santoso1, Rejeki Andayani Rahayu2
1Dept of Biochemistry Faculty of Medicine Diponegoro University Semarang, Indonesia.
2Division Geriatry Dept of Internal Medicine Faculty of Medicine Diponegoro University Semarang, Indonesia.
*Corresponding author email: [email protected]; Tel: +62-821-330-10495
Overactive bladder (OAB) is a chronic, debilitating and highly prevalent condition occurred in all age, especially among elderly affecting quality of life such as socioeconomic, psychological, occupational, domestic, physical and sexual functioning. The management of OAB can be nonpharmacologic interventions, pharmacologic interventions or combination of both. There are several substances involving smooth muscle relaxants, tricyclic antidepressants herbal medicine that can be used to encourage this OAB but still uncovered, this is a challenge for clinicians to investigate further regarding herbal medicine for OAB in order to suppress cost of OAB management because herbal medicine especially in Indonesia is cheaper than synthetic substances. The successful of management of OAB is influenced by many factors, especially from developing country such as Indonesia is the compliance of patients. The comprehensive and better understanding of this disorder is needed in order to manage OAB comprehensively. This article discuss about the comprehensive approach for managing OAB based on the clinical experience among developing country. Keyword: Overactive bladder. Elderly, herbal medicine
INTRODUCTION
Overactive bladder (OAB) defined as urgency with or
2008; Kirby et al., 2006; Dalyana, 2006; Mullins and
without urge incontinence which is usually featured with
Subak, 2005; Tapia et al., 2013; Thomas and Culley,
frequency and nocturia in the absence of other pathologic
or metabolic conditions that might explain the symptoms
There is a few number of studies regarding the
is a chronic, debilitating and highly prevalent condition
socioeconomic impact related with OAB. In United
occurred in all age. Its incidence is increased among
Kingdom annual cost of National Health Service (NHS)
elderly (MacDiarmid, 2008, Kirby et al., 2006; Dalyana,
in order to cure the symptoms of urinary tract related
disorders is approximately 536 million poundsterling, in
In more than six European countries, it was noticed that
adition, out of pocket fee from patients arround 207
this condition affects approximately 17.000 people aged
million poundsterling for pampers and other services
40 years. In addition, it was reported that 16,9% women
(Kirby et al., 2006; Tapia et al., 2013).
and 16% men above 18 years also suffered from OAB
In US, the total costs associated with overactive
(Dalyana, 2006). The severity and nature of the
bladder were estimated at US$ 12 billion. These
condition’s symptoms may be determined by gender (eg,
expenses comprise indirect costs such as lost
OAB without urge incontinence is more common in men
productivity, and direct costs, involving diagnosis,
treatment, and routine care (Mullins and Subak, 2005).
Epidemiological studies demonstrated that there is
correlation between incidence of OAB with quality of life
interventions, pharmacologic interventions or combination
such as socioeconomy, psychological, occupational,
domestic, physical and sexual functioning (MacDiarmid,
include ”bladder retraining” which generally consists of
patient education, scheduled voiding, and urge-
happened when its volume is not full enough. As
suppression techniques (Ouslander, 2004; Sandhu et al.,
consequence, the patient complains urge and unable to
A range of drugs have been used in the past for the
The symptoms of OAB are usually related to
management of OAB from smooth muscle relaxants to
unidentified causes involuntary contraction of detrusor
tricyclic antidepressants (Staskin, 2005; Pranarka, 2006).
muscle defined as detrusor hyperactivity (Andersson and
The successful of management of OAB is influenced by
Wein, 2004; Erdem and Chu, 2006; Gormley, 2008).
a lot of factors. One of important factor, especially from
There are two theory related to detrusor hyperactivity,
developing country such as Indonesia is the compliance
first is the myogenic theory. This theory depicts that the
of patients. Shyness and also false paradigm that urinary
increase of detrusor muscle excitability result increase of
related problem is normal for elderly are two of reasons
involuntary pressure of the bladder. Second theory is the
for them to not seek medical help (Pranarka, 2006;
neurogenic theory that explain that in OAB, there is
impairment of central inhibitory tract or pheripheral
Despite the considerable impact this condition has on
afferent terminal sensitization affect on primitive urination
patient’s quality of life, OAB remains underrecognized
reflexes which is stimulate overactivity of detrussor
and undertreated as a result of patient embarrassment
and reluctance to seek medical help, as well as a lack of
In OAB, it is believe that detrusor muscle hyperactivity
proactive questioning by physicians (Pranarka, 2006;
causes lack of inhibitory contraction, as a result urgency
of urination. The weakness of detrusor muscle causes
A better understanding of the negative effects of urinary
uncomplete emptying of the bladder and increase
symptoms on the economic outcomes and quality of life
frequency of mixturition (Sandhu et al., 2006; Erdem and
of patients with OAB as well the comprehensive
treatment strategies is important in order to optimize
There are several factors which influence of incidence
treatment of potential pharmacologic therapies and the
OAB. They are classified into two categories. First of all
utilization of outcomes data together with clinical
systemic factors involving metabolic status such as
assessment to determine the true strengths and
Diabetes, medication or substances causing increase of
limitations of the class of medication (Thomas and Culley,
urine production such as diuretics, caffeine, alcohol, and
neurological abnormalities resulted in damage of nerves
Despite the importance of objective assessment as well
that control urination such as stroke, infection or injury of
subjective in the management of OAB, few studies
brain or spinal cord, multiple sclerosis, and heavy metal
include subjective assessment as a primary end point.
intoxications. Second category is lower urinary tract such
Future studies with a greater emphasis on subjective
as infection, inflammation, malignancy, abnormalities or
assessment using instruments that have undergone
conditions causing urinary flow obstruction such as
validation studies, such as OAB questionnaires, are
benign prostate hyperplasia, urinary tract stones(Sandhu
needed in order to gain a better understanding related to
OAB for optimizing management of OAB, particularly
among elderly patients (Thomas and Culley, 2008).
Diagnosis of OAB Pathophysiology of OAB
The diagnosis of OAB is recognized from history taking,
complete physical examination especially on the
The two functions of the bladder are to store and void
abdomen and genital and Neurology examination for
urine. The process of micturition involves neural circuits
identification of sensory problems (Kirby et al., 2006;
in the brain and spinal cord that coordinate the anatomic
Tapia et al., 2013; Sandhu et al., 2006).
components of the lower urinary tract (Andersson and
Overactive bladder symptoms include feeling always
Wein, 2004). However, the direct connection and
want urination, Have experienced urinary urgency,
contribution of these elements are not completely
frequency, and nocturia (Tapia et al., 2013; Sandhu et al.,
Normally, as bladder volume increases, involuntary
Overactive bladder without urgency incontinence
contraction of the detrusor muscle are often associated
overactive bladder, often called dry which is about about
with overactive volume f urine voided, and the experience
two-thirds of patients with these disorders. Whereas if the
of each urination (Tapia et al., 2013; Andersson and
urinary urgency, it is often referred to as overactive
Among OAB patients, their bladder transmit false
Physical examintation is important in order to determine
impulses to the brain, resulted in immature contraction
the cause of OAB such as assessment of pelvic floor for
women to identify stress incontinence, palpation of
This exercise takes several weeks. During this training
suprapubic region for determining bladder enlargement
exercise the bladder should be recorded in a note to
and mass, digital rectal examination in men should be
monitor the progression. After a few months usually
considered to assess the size and consistency of the
patient will have normal sense of wanting to urinate or go
Laboratory examination from urine sample to check for
The successful of bladder training may be depend on
infection, glucose levels and urodynamic tests, to see the
the support of the doctors, nurses or coaches and also
function of the bladder and the ability of his emptying
the intake of enough water (Ouslander, 2004; Sandhu et
completely, uroflowmetry, the measurement of residual
al., 2006; Sussman, 2007; Thomas and Culley, 2008).
urine. Are important as routine examination (Dalyana,
Pelvic floor exercises is the main approach for stress
2006; Tapia et al., 2013; Sandhu et al., 2006).
incontinence. This exercise includes exercise to
Additional laboratory examination such as cystometry
strengthen muscles surrounded the lower part of the
to measure bladder pressure during charge. This
bladder, uterus and rectum and also suppresion the
procedure can identify the presence of involunter muscle
pelvic ground when sitting from lying to standing. It
contraction that can indicate the level of pressure which
remains unclear whether pelvic floor exercises can help
is someone feel like urinating and can measure the
urinary urgency without stress incontinence. However,
pressure needed for bladder emptying, Electromyography
pelvic floor exercises can help if it is done in conjunction
to determine the coordination of nerve impulses in the
with bladder training (Ouslander, 2004; Sandhu et al.,
muscles of the bladder and urine sphincter, urodynamics
video using x-ray or ultrasound waves to get a picture of
Another approach is usage of absorbent pad,
the bladder during charging and discharging. This test is
acupuncture and electrical stimulation. Patient may need
usually combined with the cystometry and cystoscopy.
to use diapers (absorbent pads) to protect clothing and
Used to see abnormalities on lower urinary tract for
when unable to urinate (Thomas and Culley, 2008; Oki et
example a tumor or urinary tract stones, urinary bladder
diary for 3 days to assess symptoms both before and
Emmon and Otto demonstrated that among 85 women
after the experimental treatment should be considered in
with OAB treated with acupuncture for 4 weeks has a
order to diagnose OAB (Sandhu et al., 2006; Tapia et al.,
meaningful effect for the improvement of OAB involving
on bladder capacity, urgency, frequency and quality of life
equivalently to pharmacological therapy and physical
therapy or behavior changes (Ouslander, 2004; Emmons
Management of OAB
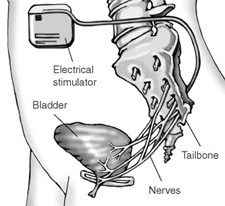
A mild electrical pulse applied through the vagina or
anus or use patches on the skin, can be used to stimulate
approach is more effective and efficient. In general, the
the nerves that control the bladder and sphincter
management of OAB divided into two approaches, first is
non pharmacological treatment involves the life style
In addition, minor surgery in order to provide electrical
changes, bladder training, and pelvic floor exercises and
stimulation can be applied by attaching an electrical wire
pharmacological treatment (Sandhu et al., 2006;
near the coccyx. In this procedure there are two stages,
Ouslander, 2004).
first the wire is placed and connected with a temporary
Life style changes involve locate the easiest way for
stimulator that can be taken for a few days. If his
toilet, drink sufficient water, avoid caffeine due to its
condition improves, it will proceed with the second step.
diuretic effect. In some people the alcohol can worsen the
Second the electric wire is placed close to the tail bone is
symptoms of overactive bladder, especially when
connected to the stimulator and permanent that is placed
combined with caffeine (Ouslander, 2004; Sandhu et al.,
under the skin (Oki et al., 2006). Figure 1.
There are several substances which can be used for
Bladder training also called bladder drill has the
treatment of OAB (Thomas and Culley, 2008; Andersson
purpose to slow down the stretch the bladder so that it
and Wein, 2004; Asimakopoulos et al., 2012; Staskin,
can enlarge the volume of the bladder and the patient
can remove the urine is only 5 – 6 times in 24 hours. At
the same time will reduce the hyperactivity of the bladder
muscles. The principle of this exercise is try to stifle and
Antimuscarinic
refrain using several ways such as sitting on hard chairs,
counting backwards from 100, doing some pelvic floor
Drug commonly used is antimuscarinic which is also
exercises (Ouslander, 2004; Sandhu et al., 2006;
commonly referred to anticholinergic. Belonging to this
Sussman, 2007; Thomas and Culley, 2008).
group are: oxybutynin, tolterodine, trospium chloride,
Figure 1. Electric Stimulator (Oki et al., 2006).
solifenacin and propiverine. These medications work by
can improve patient compliance and in some patients
way of block nerve impulses to bladder that will result in
aged prefers to wear a 'patch' rather than a pill (Emmons
the relaxation of the muscles of the bladder and will
increase the capacity of the bladder (Oki et al., 2006;
Ouslander, 2004; Hood and Andersson, 2013).
These medicines may improve symptoms in some
Tolterodine
cases. This improvement will vary on each individual. We
recommend a try given the drug for a month or so, if it
Tolterodine is an antagonist of muscarinic agent which is
helps then the medication be continued for six months or
available in the form of short-acting and long-acting.
more then the medication is stopped and seen how
Various clinical test showed that 2 mg or 4 mg per day
existing symptoms without medication (Asimakopoulos et
will be just as effective as administering oxybutynin 5 mg
The side effects of this drug are frequent but only a
light weight and can be tolerated. Frequent side effects
are dry mouth, dry eyes, constipation and blurred vision
Propiverine dantrospium
(Asimakopoulos et al., 2012, Hood and Andersson,
The drug is effective for OAB and drug side effects are
minimal compared to oxybutynin short-acting (Oki et al.,
2006, Wagg and Cohen, 2002, Asimakopoulos et al.,
Oxybutynin
Oxybutynin is the non-selective antimuscarinic that have
activity relaxing the muscles of the bladder and local
Estrogen
anesthesia. This dosage can be detached immediately (5
mg TID), off slow (5 or 10 mg O.D.) and transdermal
Local vaginal preparations are more effective than oral
patches (39 cm 2 patch in a dose of 36 mg per patch)
estrogens, but existing data about its effectiveness
that will release 2.4 mg oxybutynin per day for 3-4 days
limited (Emmons and Otto, 2005, Hood and Andersson,
Multicenter Study on Assessment of Transdermal
Therapy in Overactive Bladder With Oxybutynin
(MATRIX), has evaluated the effects of oxybutynin
Antagonis Alpha-adrenergic
transdermal system (OXY-TDS; 3.9 mg/h) towards the
quality of life and safety of the drug. On the research for 6
These agents are very useful in men with benign prostate
months to adult patients including 699 2878 age 75 years
or old. This study demonstrated that the OXY-TDS
hypotension. The dose used is raised gradually to
improves quality of life and can be well tolerated and
overcome the effects of tolerance (Hood and Andersson,
safe. OXY-TDS seems to constitute an ideal OAB
therapy in the elderly. The granting of two times per week
Imipramine
function in men with benign prostate obstruction
(Kajiwara and Mutaguchi, 2008). Another herbal medicine
An antidepressant effect of anticholinergic and tricyclic
is Ganoderma lucidum is well tolerated and there is an
with alpha-adrenergic. It may have the effect reflex
improvement of symptoms of OAB. The recommended
against Central bladder emptying so it is recommended
dose of extract of Ganoderma lucidum is 6 mg in men
to mix the urgency incontinence--stress. Its use should be
with lower urinary tract symptoms (Noguchi et al., 2008).
carefully because side effects of postural hypotension
In addition, surgery approach can be considered when
and cardiac conduction disturbances (Hood and
pharmacological or changes of life style are failed in
order to manage OAB (Gormley, 2008, Erdem and Chu,
2006). The aim of surgical treatment is to increase the
ability of the filling of the bladder and reduce pressure on
Darifanacin andsolifenacin
the bladder. By Stimulation of the nervus Sacralis which
is done by installing pacemaker under the skin of the
A antimuscarinic future with selective receptor antagonist
abdomen and connected by a small cable that is placed
Action M3 and less systemic effect anticholinergic (Jha
near the coccyx area sacralis. Modulation of nerve
impulses can improve the symptoms of OAB. Another
surgery procedure is augmentation cystoplasty. This
reconstruction procedure used to increase bladder
Capsaicin and resiniferatoxin
capacity, by using a portion of the intestine to replace
most of the bladder. On the procedure required a
An promised intravesical agent to overcome the increase
catheter to empty the bladder (Gormley, 2008).
of reflexes of detrusor muscle in neurogenic bladder.
CONCLUSION Botulinum Toxin (Botox)
To sum up, OAB is multicausal condition influencing the
There are some subtype botulinum toxin antigen which is
activity of detrussor muscle result in the urgency and
already known, namely: A, B, C1, D, E, F, and G. Types
frequency of urination with consequence on patients
A and B are used in urology. Botulinum toxin in action by
quality of life involving psychological and socioeconomic
way of inhibiting the release of acetylcholine from the
problems. The comprehensive and better understanding
nerve endings kolinergik interacting with the protein
of this disorders is needed in order to manage OAB
complex that is used to populate the acetylcholine
vesicles. Effects of botulinum toxin was losing muscle
contraction and muscle atrophy at the site of the injection.
Chemical denervation are reversible and the regeneration
Future Prospect and Suggestion
of the axon will occur within approximately 3-6 months.
Administration of botulinum toxin in sufficient quantities
Regarding pharmacological theurapeutic approach, there
will inhibit the release of acetylcholine and other
are several substances involving herbal medicine that
neurotransmitters. The molecules cannot pass through
can be used to encourage this OAB but still uncovered,
the brain barrier so it has no effect on the CNS. The use
this is a challenge for clinicians to investigate further
of botulinum toxin is rising quickly, used to treat
regarding herbal medicine for OAB in order to suppress
neurogenic detrusor idiopathic overaktivitas and by
cost of OAB management because herbal medicine
means of the injection of (Sahai et al., 2007; MacDiarmid,
especially in Indonesia is cheaper than synthetic
Herbal medicine Acknowledgement
Despite of synthetic substances, there are some herbal
This study is based on the experience of clinical practice
medicine used for the treatment of OAB. One of the most
in Sub Division of Geriatry Dept of Internal Medicine,
popular is a traditional Chinese medicine using Gosha-
Faculty of Medicine Diponegoro University - Dr. Kariadi
jinki-gan (Ogushi and Takahashi, 2007). Previous study
Hospital Semarang Indonesia. We would like to thank to
demonstrated that Goshi-jinki-gan ma be a new potential
all people in Division of Geriatry Dept of Internal Medicine,
therapeutic agent for OAB without deterioration of voiding
Faculty of Medicine Diponegoro University - Dr. Kariadi
Hospital Semarang Indonesia for the opportunity to carry
Mullins CD, Subak LL (2005). New Perspectives on Overactive Bladder:
this study in this hospital. Lastly we send our gratitude to
Quality of Life Impact, Persistency, and Medication Treatment Costs. The American Journal Of Managed Care, 11.
our team and staff of Dept of Biochemistry Faculty of
Noguchi M, Kakuma T, Tomiyasu K, Kurita Y, Kukihara H, Konishi F,
Medicine Diponegoro University, Semarang Indonesia.
Kumamoto S, Shimizu K, Kondo R, Matsuoka K (2008). Effect of an
extract of Ganoderma lucidum in men with lower urinary tract
symptoms: a double-blind, placebo-controlled randomized and dose-ranging study. Asian J Androl, 10, 651-658.
REFERENCES
Ogushi T, Takahashi S (2007). Effect of Chinese herbal medicine on
Andersson KE, Wein AJ (2004). Pharmacology of the Lower Urinary
Tract: Basis for Current and Future Treatments of Urinary
Oki T, Toma-Okura A, Yamada S (2006). NEUROPHARMACOLOGY :
Incontinence. Pharmacol Rev, 58, 581-631.
Advantages for Transdermal over Oral Oxybutynin to Treat
Asimakopoulos AD, Cerruto MA, Popolo GD, Martina ML, Artibani W,
Overactive Bladder: Muscarinic Receptor Binding, Plasma Drug
Carone R, Finazzi-Agrò E (2012). An Overview on Mixed Action
Concentration, and Salivary Secretion. JPET, 316, 1137-1145.
Drugs for the Treatment of Overactive Bladder and Detrusor
Ouslander JG (2004). Management of Overactive Bladder. N Engl J
Dalyana (2006). Overactive bladder. J. Indian Acad. Clin. Med. 7.
Pranarka K (2006). Incontinence herbs treatment in Elderly: From Basic
Emmons and Otto (2005). Acupuncture for Overactive Bladder. Obstet
to Clinical Practice. The Symposium Of Incontinence. Semarang,
Erdem N,Chu FM (2006). Management of Overactive Bladder And Urge
Sahai A, Khan MS, Gregson N, Smith K, Dasgupta P (2007). Botulinum
Urinary Incontinence In The Elderly Patient. Am. J. Med. 119, 29-36.
toxin for detrusor overactivity and symptoms of overactive bladder:
Gormley EA (2008). Overactive Bladder: Management And Treatment
where we are now and where we are going. Nature Clinical Practice
Options. The Masters in Urology Meeting. Semarang, Bermuda.
Hood B, Andersson KE (2013). Common theme for drugs effective in
Sandhu JS, Gupta A, Mohan V, Markan A, Sandhu P (2006). Approach
overactive bladder treatment: Inhibition of afferent signaling from the
to Overactive Bladder. JIACM, 7, 109-112.
Staskin DR (2005). Overactive Bladder In The Elderly: A Guide to
Jha S, Parsons M (2006). Treatment of overactive bladder in the aging
Pharmacological Management. Drugs Aging, 22, 1013-1028.
population: focus on darifenacin. Clin. Intervent in Aging, 1, 309-316.
Sussman DO (2007). Overactive Blader: Treatment options in primary
Kajiwara M, Mutaguchi K (2008). Clinical efficacy and tolerability of
gosha-jinki-gan, Japanese traditional herbal medicine, in females with
Tapia CI, Khalaf K, Berenson K, Globe D, Chancellor M, Carr LK (2013).
Health-related quality of life and economic impact of urinary
incontinence due to detrusor overactivity associated with a neurologic
Kirby M, Artibani W, Cardozo L, Chapple C, Diaz C (2006). Overactive
condition: a systematic review. BioMed Central, 11.
Bladder: the Importance of the New Guidance. Int. J. Clin. Pract. 60,
Thomas L, Culley EJ (2008). Overactive Bladder Disease: The Urge for
Better Therapies. J. Manag. Care Pharm. 14, 381-386.
Macdiarmid SA (2008). Maximizing the Treatment of Overactive Bladder
Wagg A, Cohen M (2002). Medical Therapy For The Overactive Bladder
In The Elderly. Age Ageing, 31, 241-246.
NON-INJECTABLE MEDICATIONS THAT REQUIRE AUTHORIZATION PRIOR TO COVERAGE UNDER THE ENROLLEE’S RXPRIME BENEFIT. Brand Name Requires documentation of diagnosis of anginaRequires documentation of diagnosis of testosteronedeficiency in menRequires documentation of diagnosis of Osteoarthritis orRheumatoid Arthritis and evidence of risk of gastrointestinaladverse reaction to other NSAIDs. Requi
COSTA RICA PREPARING TO GO ATM and Credit Cards – We recommend that you contact your bank in advance of departing on this tour to determine whether you will be able to use your ATM and credit cards while traveling. When contacting your bank, notify them of your travel dates so that they will anticipate charges being made outside of your hometown and do not suspend your cards for